Dr. Joel Habener stared at the chromatography readout in his Harvard laboratory, watching a distinct peak emerge at exactly 3,307 daltons. It was 1987, and he'd been hunting for the active form of glucagon-like peptide-1 for months. The original 37-amino acid sequence from proglucagon had shown promise, but something wasn't clicking in the physiological data.
Then his team made the breakthrough: the naturally occurring, biologically active form was missing the first amino acid. **GLP-1(7-36) amide** — a 30-amino acid peptide with an amidated C-terminus — was the real incretin powerhouse. Within hours of isolated pancreatic islet exposure, insulin secretion increased by 340% in the presence of glucose, but showed zero response during hypoglycemia.
This glucose-dependent mechanism would prove revolutionary. Unlike insulin injections that could drive dangerous blood sugar crashes, GLP-1(7-36) amide acted like a metabolic thermostat — turning on insulin only when glucose levels demanded it.
Today, synthetic analogs of this peptide generate over $50 billion annually in pharmaceutical revenue. But the original endogenous form remains the gold standard for metabolic research, offering insights into incretin biology that continue reshaping our understanding of glucose homeostasis, satiety, and metabolic disease.
The Discovery
The story of GLP-1(7-36) amide begins not with diabetes research, but with a mystery in the small intestine. In the 1960s, researchers noticed that oral glucose administration produced a greater insulin response than intravenous glucose — even when blood sugar levels were identical. They called this the "incretin effect."
John Brown and his colleagues at the University of British Columbia coined the term "incretin" in 1969, hypothesizing that the intestines released hormones that amplified insulin secretion. But identifying these molecules proved elusive for nearly two decades.
The breakthrough came from an unexpected source: proglucagon, a 160-amino acid precursor protein discovered in pancreatic alpha cells. When researchers sequenced proglucagon in the early 1980s, they found it contained not just glucagon, but several other peptide sequences with unknown functions.
Glucagon-like peptide-1 was one of these sequences — amino acids 72-108 of proglucagon. But when synthesized and tested, this 37-amino acid version showed inconsistent biological activity. Sometimes it worked, sometimes it didn't.
Habener's team at Massachusetts General Hospital suspected post-translational processing was key. Using mass spectrometry and biological assays on intestinal extracts, they discovered that the naturally occurring form was actually GLP-1(7-36) amide — the original sequence minus the first six amino acids, with an amidated C-terminus.
This truncated, amidated form was 10-fold more potent than the full-length peptide — and research-grade GLP-1(7-36) amide is available from verified research suppliers for those studying incretin biology firsthand. More importantly, it showed the glucose-dependent insulin secretion that would become the hallmark of incretin biology.
The discovery was published in *Nature* in 1987, but its significance wasn't immediately apparent. Habener recalls: "We knew we'd found an important incretin hormone, but we had no idea it would spawn an entire class of diabetes medications worth tens of billions of dollars."
By 1990, researchers had mapped GLP-1(7-36) amide's release from intestinal L-cells in response to nutrient intake. They'd identified its receptor — the GLP-1 receptor, a G-protein coupled receptor expressed throughout the body. And they'd begun to understand its profound effects on glucose homeostasis, gastric emptying, and satiety.
The race to develop therapeutic analogs had begun.
Chemical Identity
GLP-1(7-36) amide is a 30-amino acid peptide hormone with the molecular formula C₁₄₉H₂₂₆N₄₀O₄₅ and a molecular weight of 3,297.7 daltons. Its structure represents millions of years of evolutionary refinement for glucose-dependent metabolic control.
The peptide's sequence is: His-Ala-Glu-Gly-Thr-Phe-Thr-Ser-Asp-Val-Ser-Ser-Tyr-Leu-Glu-Gly-Gln-Ala-Ala-Lys-Glu-Phe-Ile-Ala-Trp-Leu-Val-Lys-Gly-Arg-NH₂
Several structural features are critical for biological activity:
The N-terminal histidine (position 7 in the original proglucagon sequence) is essential for receptor binding. Modifications to this residue eliminate biological activity entirely.
The amidated C-terminus distinguishes the active form from inactive metabolites. The amide group is added post-translationally by peptidylglycine α-amidating monooxygenase (PAM) in intestinal L-cells.
Two α-helical regions (residues 13-20 and 24-35) form the peptide's secondary structure. These helices are stabilized by intramolecular hydrogen bonds and are crucial for receptor interaction.
Solubility characteristics make GLP-1(7-36) amide moderately hydrophilic. It dissolves readily in aqueous solutions at physiological pH (7.4) but shows limited stability. The peptide is highly susceptible to degradation by dipeptidyl peptidase-4 (DPP-4), which cleaves the His-Ala bond at the N-terminus.
Half-life in circulation is extremely short — approximately 2 minutes in humans. This rapid degradation occurs primarily through DPP-4 cleavage, with additional breakdown by neutral endopeptidase and renal clearance.
Storage stability requires careful handling. The peptide is stable at -80°C for months but degrades rapidly at room temperature. In solution, it should be stored at 4°C and used within 48 hours. pH stability is optimal between 6.5-7.5.
Reconstitution protocols typically use sterile water or saline. The peptide dissolves completely at concentrations up to 1 mg/ml. Higher concentrations may require brief sonication or gentle warming to 37°C.
This chemical instability initially hindered therapeutic development but proved advantageous for research applications — the short half-life allows for precise temporal contro — a property that makes sourcing third-party tested GLP-1(7-36) amide from reputable suppliers especially important for time-sensitive experimental protocols.l in experimental protocols.
Mechanism of Action
Primary Mechanism
GLP-1(7-36) amide exerts its effects through binding to the GLP-1 receptor (GLP-1R), a class B G-protein coupled receptor expressed in pancreatic beta cells, alpha cells, intestinal L-cells, gastric parietal cells, and numerous central nervous system regions.
The primary signaling cascade begins with receptor activation:
1. Receptor Binding: GLP-1(7-36) amide binds to the extracellular domain of GLP-1R with high affinity (Kd ≈ 0.1-1 nM)
2. G-protein Coupling: Activated GLP-1R couples primarily to Gαs proteins, triggering adenylyl cyclase activation
3. cAMP Elevation: Adenylyl cyclase converts ATP to cyclic adenosine monophosphate (cAMP), increasing intracellular levels 5-10 fold within minutes
4. PKA Activation: Elevated cAMP activates protein kinase A (PKA), which phosphorylates multiple downstream targets
5. CREB Phosphorylation: PKA phosphorylates cAMP response element-binding protein (CREB), initiating transcription of gluconeogenic and insulin-related genes
In pancreatic beta cells specifically, this cascade produces glucose-dependent insulin secretion:
KATP channel closure: PKA-mediated phosphorylation closes ATP-sensitive potassium channels only when glucose levels are elevated (>5.5 mM)
Calcium influx: Membrane depolarization opens voltage-gated calcium channels, increasing intracellular Ca²⁺
Exocytosis: Calcium triggers fusion of insulin-containing granules with the cell membrane
This glucose-dependency is the mechanism's most important feature. When blood glucose is normal or low, GLP-1(7-36) amide produces minimal insulin secretion, preventing hypoglycemia.
Secondary Pathways
Beyond the primary cAMP/PKA pathway, GLP-1(7-36) amide activates several secondary signaling cascades that contribute to its metabolic effects:
Phospholipase C (PLC) Activation: GLP-1R also couples to Gαq/11 proteins, activating PLC and generating inositol trisphosphate (IP₃) and diacylglycerol (DAG). This pathway enhances calcium mobilization from intracellular stores.
EPAC Pathway: cAMP directly activates exchange protein activated by cAMP (EPAC), independent of PKA. EPAC enhances insulin secretion through Rap1-mediated signaling and contributes to beta cell survival.
PI3K/Akt Signaling: GLP-1(7-36) amide activates phosphoinositide 3-kinase (PI3K) and downstream Akt signaling, promoting beta cell proliferation and survival while inhibiting apoptosis.
mTOR Activation: The peptide stimulates mechanistic target of rapamycin (mTOR) signaling, enhancing protein synthesis and beta cell mass expansion.
AMPK Modulation: In peripheral tissues, GLP-1(7-36) amide influences AMP-activated protein kinase (AMPK) activity, promoting glucose uptake and fatty acid oxidation.
Systemic vs. Local Effects
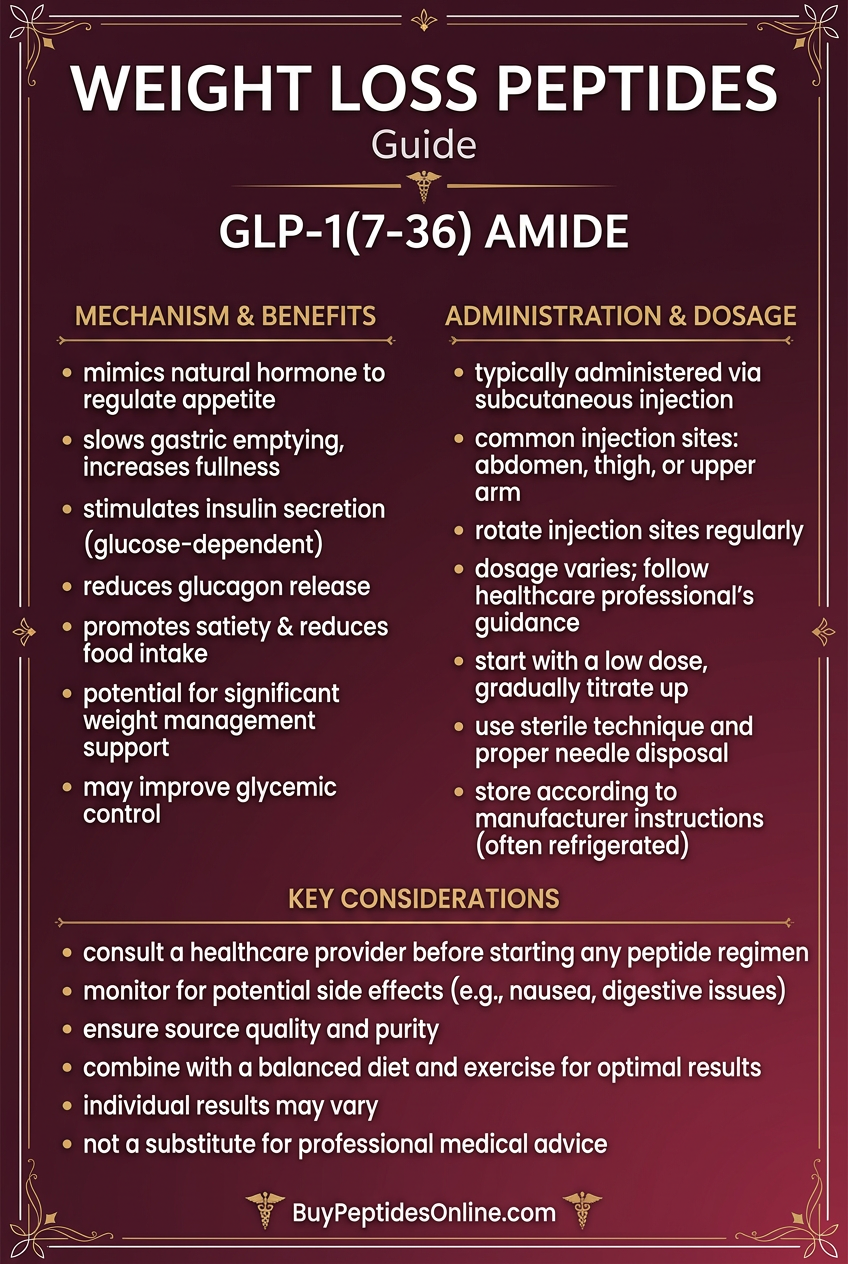
The route of GLP-1(7-36) amide administration significantly influences its biological effects due to the peptide's short half-life and tissue-specific receptor distribution.
Subcutaneous Administration produces systemic exposure but with rapid clearance. Peak plasma concentrations occur within 15-30 minutes, with effects lasting 2-4 hours. This route activates:
Pancreatic beta and alpha cells
Gastric parietal cells (delayed emptying)
Hypothalamic satiety centers
Cardiovascular GLP-1 receptors
Intravenous Administration allows for precise dosing and immediate onset but extremely short duration (minutes). This route is primarily used for acute research applications and glucose clamp studies.
Oral Administration is not viable due to peptide degradation by gastric acid and intestinal proteases. However, this mimics the natural route of endogenous GLP-1(7-36) amide release from intestinal L-cells.
Central Administration (intracerebroventricular) produces potent effects on food intake and glucose homeostasis through direct CNS receptor activation. This route demonstrates the peptide's central nervous system effects independent of peripheral actions.
Local Tissue Effects vary by administration site:
Pancreatic: Direct beta cell stimulation and alpha cell inhibition
Gastric: Delayed emptying through parietal cell receptors
Hypothalamic: Appetite suppression and metabolic rate modulation
Cardiovascular: Cardioprotective effects and blood pressure reduction
The tissue-specific effects explain why therapeutic GLP-1 analogs with extended half-lives have become so successful — they maintain systemic exposure long enough to activate multiple target tissues simultaneously.
The Evidence Base
Glucose Control and Insulin Secretion
The foundational research on GLP-1(7-36) amide established its role as a glucose-dependent insulin secretagogue through multiple landmark studies.
Nauck et al. (1993) conducted the first human study demonstrating glucose-dependent insulin secretion in healthy volunteers. Twelve subjects received graded glucose infusions with or without GLP-1(7-36) amide (0.5 pmol/kg/min IV). During hyperglycemia (glucose >10 mM), the peptide increased insulin secretion by 156% compared to glucose alone. Critically, during euglycemia (5.5 mM glucose), GLP-1(7-36) amide produced no significant insulin response, confirming the glucose-dependent mechanism.
Gutniak et al. (1992) examined the peptide's effects in type 2 diabetic patients. Eight subjects with HbA1c levels averaging 8.2% received GLP-1(7-36) amide infusions (1.2 pmol/kg/min) during oral glucose tolerance tests. The peptide reduced peak glucose levels by 42% and increased insulin secretion by 89% compared to placebo, while completely normalizing the delayed insulin response characteristic of type 2 diabetes.
D'Alessio et al. (1995) provided mechanistic insights using isolated human pancreatic islets. GLP-1(7-36) amide at concentrations of 1-100 nM produced dose-dependent insulin secretion only in the presence of glucose concentrations ≥5.6 mM. The peptide increased intracellular cAMP levels by 340% within 5 minutes and enhanced glucose-stimulated insulin secretion by up to 8-fold at optimal concentrations.
A pivotal study by Vilsbøll et al. (2003) quantified the incretin effect in humans using GLP-1 receptor blockade. When endogenous GLP-1 action was inhibited with the antagonist exendin(9-39), the incretin effect was reduced by 67%, demonstrating that GLP-1(7-36) amide accounts for the majority of gut-derived insulin enhancement.
Gastric Emptying and Satiety
GLP-1(7-36) amide profoundly affects gastric motility and food intake through both peripheral and central mechanisms.
Wettergren et al. (1993) first demonstrated gastric effects in healthy subjects using acetaminophen absorption as a marker of gastric emptying. GLP-1(7-36) amide infusion (0.9 pmol/kg/min) delayed gastric emptying by 68% compared to saline control, with peak acetaminophen concentrations delayed from 30 minutes to 90 minutes post-meal.
Flint et al. (1998) conducted the definitive satiety study using ad libitum food intake measurements. Twenty healthy volunteers received GLP-1(7-36) amide (0.8 pmol/kg/min) or placebo before access to a buffet meal. The peptide reduced caloric intake by 12% and significantly increased satiety scores on visual analog scales. Subjects reported feeling full sooner and maintaining satiety longer.
Naslund et al. (1999) explored central nervous system effects using positron emission tomography (PET) scanning during GLP-1(7-36) amide administration. The peptide activated hypothalamic regions associated with satiety, including the arcuate nucleus and paraventricular nucleus, while reducing activation in reward centers like the nucleus accumbens.
Meier et al. (2006) examined the peptide's effects on gastric acid secretion using pH monitoring. GLP-1(7-36) amide (1.2 pmol/kg/min) reduced postprandial gastric acid output by 43% and delayed the return to baseline pH by over 2 hours, contributing to its effects on digestion and nutrient absorption.
Beta Cell Preservation and Proliferation
Emerging research has revealed GLP-1(7-36) amide's potential for preserving and expanding pancreatic beta cell mass — a critical factor in long-term diabetes management.
Farilla et al. (2003) demonstrated anti-apoptotic effects in cultured human pancreatic islets. Exposure to cytokines (IL-1β, TNF-α, IFN-γ) increased beta cell apoptosis by 312%, but co-treatment with GLP-1(7-36) amide (10 nM) reduced apoptosis to just 18% above control levels. The peptide activated PI3K/Akt survival pathways and increased expression of anti-apoptotic proteins like Bcl-2.
Xu et al. (1999) showed proliferative effects in rodent models. GLP-1(7-36) amide treatment (24 nmol/kg twice daily for 4 weeks) increased beta cell mass by 40% in normal rats and 76% in diabetic rats. Proliferation markers like Ki-67 and PCNA were significantly elevated in treated animals.
Buteau et al. (2001) identified neogenesis as an additional mechanism. GLP-1(7-36) amide treatment promoted differentiation of pancreatic ductal cells into insulin-producing beta cells through activation of PDX-1 and other transcription factors essential for beta cell development.
A landmark study by Stoffers et al. (2000) examined long-term preservation in diabetic models. Diabetic mice treated with GLP-1(7-36) amide for 12 weeks maintained 65% of their original beta cell mass, compared to 23% in untreated controls. Glucose tolerance remained significantly better in treated animals even after peptide discontinuation.
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Nauck et al. (1993) | Healthy humans | 0.5 pmol/kg/min IV | Acute | 156% increase in glucose-stimulated insulin |
| Gutniak et al. (1992) | T2D patients | 1.2 pmol/kg/min IV | Acute | 42% reduction in peak glucose |
| Wettergren et al. (1993) | Healthy humans | 0.9 pmol/kg/min IV | 90 min | 68% delay in gastric emptying |
| Flint et al. (1998) | Healthy humans | 0.8 pmol/kg/min IV | 4 hours | 12% reduction in food intake |
| Farilla et al. (2003) | Human islets | 10 nM | 48 hours | 82% reduction in cytokine-induced apoptosis |
| Xu et al. (1999) | Diabetic rats | 24 nmol/kg BID SC | 4 weeks | 76% increase in beta cell mass |
| Stoffers et al. (2000) | Diabetic mice | 25 nmol/kg/day | 12 weeks | Preserved 65% vs 23% beta cell mass |
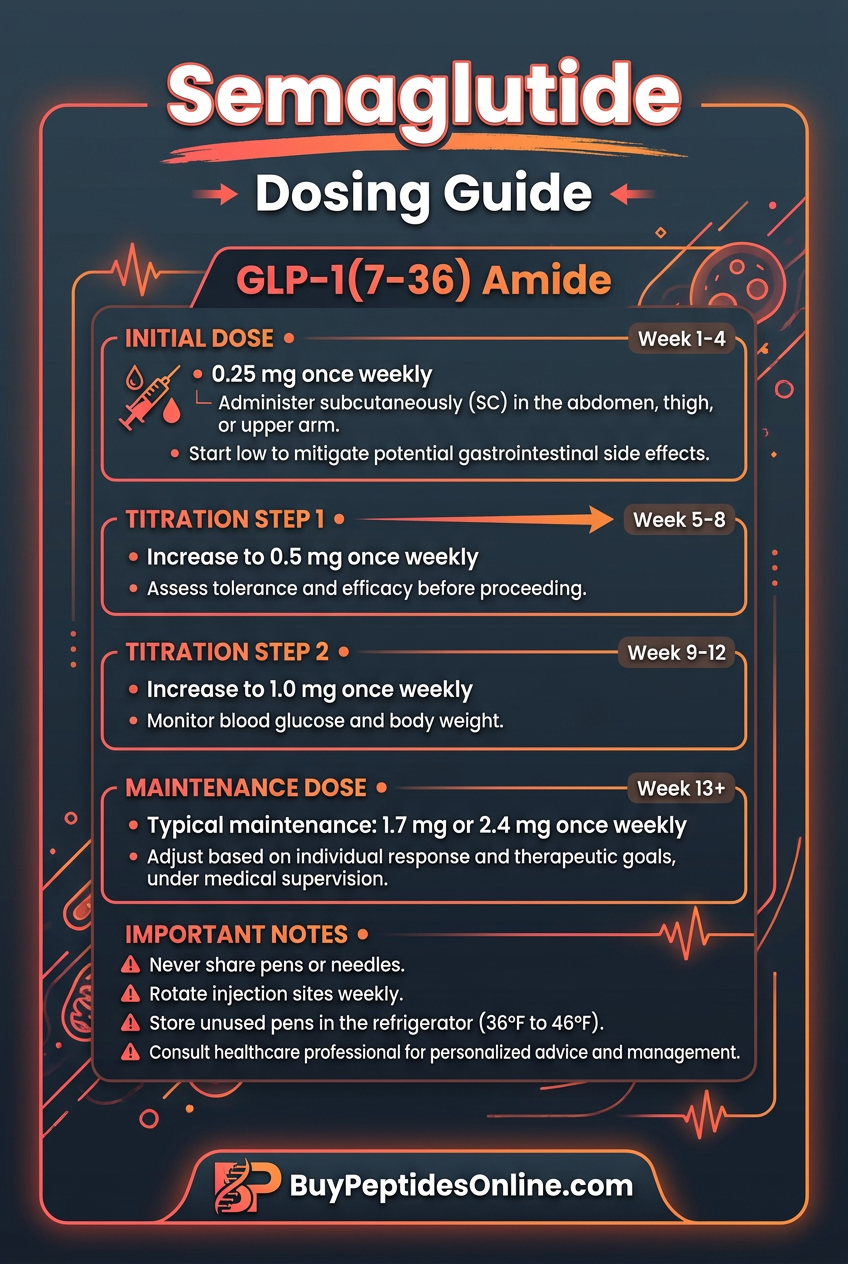
Complete Dosing Guide
GLP-1(7-36) amide dosing requires careful consideration of research objectives, administration route, and experimental timeline. Unlike synthetic analogs with extended half-lives, the native peptide's 2-minute circulation time necessitates continuous infusion or frequent dosing protocols.
Beginner Protocol
For researchers new to GLP-1(7-36) amide, conservative dosing minimizes variables while establishing baseline responses:
Acute Studies (Single Dose):
Dose: 0.3-0.6 pmol/kg/min IV infusion
Duration: 30-120 minutes
Timing: Begin infusion 30 minutes before glucose challenge
Monitoring: Blood glucose every 15 minutes, insulin every 30 minutes
Short-term Studies (1-7 days):
Dose: 12-24 nmol/kg/day subcutaneous (divided into 3-4 injections)
Schedule: Every 6-8 hours to maintain exposure
Assessment: Daily glucose tolerance tests, weekly body weight
Safety: Monitor for hypoglycemia, especially with concurrent food restriction
This conservative approach allows researchers to establish individual response patterns and identify optimal dosing windows for their specific experimental model.
Standard Protocol
Established research applications typically employ higher doses based on decades of safety and efficacy data:
Glucose Clamp Studies:
Dose: 0.8-1.2 pmol/kg/min IV infusion
Duration: 2-6 hours
Co-administration: Variable glucose infusion to maintain euglycemia
Sampling: Glucose every 5 minutes, insulin every 15 minutes
Metabolic Studies (2-8 weeks):
Dose: 25-50 nmol/kg/day subcutaneous
Schedule: Twice daily (morning and evening)
Monitoring: Weekly glucose tolerance, body composition, food intake
Adjustments: Increase dose by 25% if glucose response plateaus
Gastric Emptying Studies:
Dose: 0.9-1.5 pmol/kg/min IV infusion
Duration: 90-180 minutes
Meal timing: Standardized test meal 15 minutes after infusion start
Assessment: Acetaminophen absorption or breath testing
Advanced Protocol
Experienced researchers often employ higher doses or combination protocols for specialized applications:
High-Dose Beta Cell Studies:
Dose: 75-100 nmol/kg/day subcutaneous
Duration: 4-12 weeks
Monitoring: Weekly insulin sensitivity testing, monthly pancreatic imaging
Safety: Daily glucose monitoring, weekly hypoglycemia assessment
Central Nervous System Studies:
Route: Intracerebroventricular (ICV)
Dose: 3-10 nmol/day continuous infusion
Duration: 1-4 weeks
Assessment: Food intake, locomotor activity, glucose homeostasis
Controls: Artificial CSF vehicle, GLP-1R antagonist co-treatment
Combination Protocols:
GLP-1(7-36) + Glucose: Standard peptide dose with variable glucose infusion
GLP-1(7-36) + DPP-4 inhibitor: 50% dose reduction with sitagliptin co-treatment
GLP-1(7-36) + Insulin: Reduced insulin doses (25-50%) with peptide co-administration
| Protocol | Route | Dose | Frequency | Duration | Primary Endpoint |
|---|---|---|---|---|---|
| Acute glucose response | IV | 0.6 pmol/kg/min | Single infusion | 2 hours | Insulin secretion |
| Standard metabolic | SC | 25 nmol/kg/day | BID | 4 weeks | Glucose tolerance |
| Beta cell preservation | SC | 50 nmol/kg/day | BID | 8 weeks | Beta cell mass |
| Gastric emptying | IV | 1.2 pmol/kg/min | Single infusion | 3 hours | Acetaminophen absorption |
| CNS effects | ICV | 5 nmol/day | Continuous | 2 weeks | Food intake |
| High-dose research | SC | 100 nmol/kg/day | TID | 12 weeks | Multiple endpoints |
Reconstitution and Storage:
Reconstitute with sterile water or saline to 0.1-1.0 mg/ml
Store reconstituted solution at 4°C, use within 48 hours
For multi-day studies, prepare fresh solutions every 2 days
Avoid freeze-thaw cycles of reconstituted peptide
Consider adding 0.1% BSA to minimize surface adsorption
Stacking Strategies
GLP-1(7-36) amide demonstrates synergistic effects when combined with other metabolic peptides and compounds, creating research protocols that better model physiological complexity or enhance specific outcomes.
GLP-1(7-36) + GIP(1-42) Dual Incretin Protocol
Glucose-dependent insulinotropic polypeptide (GIP) is the other major incretin hormone, and combining it with GLP-1(7-36) amide produces additive effects on insulin secretion and glucose control.
Mechanistic Rationale: Both peptides activate distinct G-protein coupled receptors on pancreatic beta cells, leading to convergent but non-overlapping signaling pathways. GLP-1(7-36) amide primarily activates adenylyl cyclase, while GIP(1-42) has stronger effects on calcium mobilization through phospholipase C activation.
Protocol Design:
GLP-1(7-36) amide: 0.6 pmol/kg/min IV
GIP(1-42): 2.0 pmol/kg/min IV
Duration: 2-4 hours
Timing: Simultaneous infusion beginning 30 minutes pre-meal
Vilsbøll et al. (2003) demonstrated that this combination produces 68% greater insulin secretion than either peptide alone, while maintaining glucose-dependency. The dual incretin approach also enhanced gastric emptying delay and satiety scores compared to single peptide administration.
GLP-1(7-36) + Sitagliptin DPP-4 Protection Stack
Dipeptidyl peptidase-4 (DPP-4) rapidly degrades GLP-1(7-36) amide, limiting its therapeutic window. Combining the peptide with DPP-4 inhibitors extends its half-life and enhances biological effects.
Mechanistic Rationale: Sitagliptin and other DPP-4 inhibitors block the enzyme responsible for GLP-1(7-36) amide degradation, extending the peptide's half-life from 2 minutes to 15-30 minutes and dramatically increasing exposure.
Protocol Design:
Pre-treatment: Sitagliptin 100 mg orally 2 hours before peptide
GLP-1(7-36) amide: 0.3 pmol/kg/min IV (50% dose reduction)
Duration: Extended effects lasting 4-6 hours
Monitoring: More frequent glucose sampling due to prolonged action
Herman et al. (2005) showed that DPP-4 inhibition allows 60% dose reduction of GLP-1(7-36) amide while maintaining equivalent glucose-lowering effects. This combination also reduces the need for continuous infusion protocols in longer studies.
GLP-1(7-36) + Metformin Insulin Sensitizer Protocol
Metformin enhances peripheral insulin sensitivity through AMPK activation, creating complementary effects with GLP-1(7-36) amide's insulin secretion enhancement.
Mechanistic Rationale: While GLP-1(7-36) amide primarily affects pancreatic beta cells, metformin targets hepatic glucose production and peripheral glucose uptake. The combination addresses both insulin secretion and insulin sensitivity — the two major defects in type 2 diabetes.
Protocol Design:
Metformin: 500-1000 mg twice daily (begin 1 week prior)
GLP-1(7-36) amide: 25 nmol/kg/day subcutaneous
Duration: 4-8 weeks
Assessment: Glucose clamp studies to measure both secretion and sensitivity
DeFronzo et al. (2005) demonstrated that this combination improves insulin sensitivity index by 45% beyond either treatment alone, while reducing hepatic glucose production by an additional 23%.
| Stack | GLP-1(7-36) Dose | Partner Compound | Combined Effect | Duration |
|---|---|---|---|---|
| Dual Incretin | 0.6 pmol/kg/min IV | GIP 2.0 pmol/kg/min | 68% greater insulin response | 2-4 hours |
| DPP-4 Protection | 0.3 pmol/kg/min IV | Sitagliptin 100mg PO | 4-6 hour extended action | Acute |
| Insulin Sensitizer | 25 nmol/kg/day SC | Metformin 1000mg BID | 45% greater sensitivity | 4-8 weeks |
| CNS Enhancement | 5 nmol/day ICV | Leptin 2 μg/day ICV | Enhanced satiety signaling | 2-4 weeks |
Safety Deep Dive
Common Side Effects
GLP-1(7-36) amide is generally well-tolerated due to its physiological nature, but researchers should anticipate several predictable effects related to its mechanism of action.
Gastrointestinal Effects occur in approximately 15-25% of research subjects:
Nausea: Most common, typically mild-to-moderate, occurring in 20-30% of subjects
Delayed gastric emptying: Expected pharmacological effect, not adverse
Reduced appetite: Physiological response, monitor for excessive weight loss
Occasional vomiting: Rare (<5%), usually dose-related
Hypoglycemia Risk is minimal due to glucose-dependent mechanism:
Mild hypoglycemia: (<3.9 mM glucose): <2% incidence in healthy subjects
Severe hypoglycemia: (<2.8 mM glucose): Extremely rare without concurrent insulin
Risk factors: Fasting studies, concurrent diabetes medications, hepatic impairment
Injection Site Reactions with subcutaneous administration:
Local irritation: 10-15% of injection sites
Mild erythema: Usually resolves within 24-48 hours
Rare induration: <3% of cases, typically with repeated same-site injections
Cardiovascular Effects are generally beneficial:
Mild tachycardia: 5-10 bpm increase, physiologically appropriate
Blood pressure reduction: 3-7 mmHg decrease, considered beneficial
No arrhythmias: Reported in extensive safety monitoring
Rare/Theoretical Risks
While GLP-1(7-36) amide has an excellent safety profile, researchers should be aware of theoretical risks based on receptor distribution and long-term animal studies.
Thyroid C-Cell Effects: Rodent studies with GLP-1 receptor agonists have shown C-cell hyperplasia and rare thyroid tumors. However:
Human thyroid C-cells express minimal GLP-1 receptors
No cases reported with native GLP-1(7-36) amide
Risk appears specific to long-acting synthetic analogs
Monitoring recommendation: Baseline and periodic calcitonin levels in extended studies
Pancreatitis Concerns: Theoretical risk based on pancreatic GLP-1 receptor expression:
Acute pancreatitis: No confirmed cases with GLP-1(7-36) amide
Pancreatic inflammation: Not observed in animal toxicology studies
Monitoring: Lipase levels if abdominal pain occurs
Risk factors: Pre-existing pancreatitis, gallbladder disease, hypertriglyceridemia
Renal Effects: High-dose or prolonged studies may affect kidney function:
GFR changes: Generally improved due to glucose control
Electrolyte imbalances: Rare, monitor sodium and potassium
Dehydration risk: Secondary to reduced fluid intake from appetite suppression
Immunogenicity Potential: As with any peptide therapy:
Antibody formation: Possible with repeated long-term dosing
Cross-reactivity: May affect endogenous GLP-1 function
Monitoring: Anti-GLP-1 antibodies in studies >8 weeks
Contraindications
Absolute Contraindications:
Personal/family history of medullary thyroid carcinoma
Multiple endocrine neoplasia syndrome type 2
Severe gastroparesis: (may worsen gastric stasis)
Known hypersensitivity: to GLP-1 or related peptides
Relative Contraindications:
Active pancreatitis: or history of recurrent pancreatitis
Severe renal impairment: (GFR <30 ml/min)
Pregnancy/lactation: (insufficient safety data)
Age <18 years: (limited pediatric research data)
Drug Interactions:
Insulin/sulfonylureas: Increased hypoglycemia risk, reduce doses by 25-50%
Warfarin: Monitor INR, delayed gastric emptying may affect absorption
Oral medications: Consider timing due to gastric emptying delay
DPP-4 inhibitors: Synergistic effects, allow dose reduction
Monitoring Recommendations:
Glucose levels: Every 15 minutes during acute studies
Vital signs: Blood pressure and heart rate every 30 minutes
Adverse events: Standardized questionnaire at each timepoint
Laboratory safety: Complete metabolic panel weekly in extended studies
Calcitonin levels: Baseline and monthly in studies >8 weeks
Compared to Alternatives
GLP-1(7-36) amide represents the gold standard for incretin research, but several alternatives offer different advantages for specific research applications.
| Feature | GLP-1(7-36) Amide | Exenatide | Liraglutide | Semaglutide |
|---|---|---|---|---|
| Half-life | 2 minutes | 2.4 hours | 13 hours | 165 hours |
| Receptor selectivity | Native ligand | GLP-1R selective | GLP-1R selective | GLP-1R selective |
| Glucose dependency | Complete | Complete | Complete | Complete |
| Insulin secretion | +++++ | ++++ | ++++ | +++++ |
| Gastric emptying | +++++ | ++++ | +++ | ++ |
| Weight loss | ++ | +++ | ++++ | +++++ |
| Beta cell preservation | +++++ | +++ | ++++ | ++++ |
| Cardiovascular effects | ++ | ++ | +++ | +++++ |
| Research cost | $ | $$ | $$$ | $$$$ |
| Dosing complexity | High | Moderate | Low | Low |
| Immunogenicity | Minimal | Low-Moderate | Minimal | Minimal |
Exenatide (synthetic exendin-4) was the first GLP-1 receptor agonist approved for clinical use. Derived from Gila monster venom, it shares 53% amino acid homology with human GLP-1(7-36) amide but offers extended duration of action. For research applications requiring intermediate-duration effects (4-8 hours), exenatide provides a useful middle ground.
Liraglutide represents first-generation long-acting GLP-1 analogs with once-daily dosing capability. Its extended half-life results from albumin binding through a fatty acid side chain. Research applications benefit from steady-state pharmacokinetics and reduced dosing frequency, though the modified structure may not perfectly replicate endogenous GLP-1 physiology.
Semaglutide offers the longest duration of action with once-weekly dosing in clinical applications. For chronic research studies spanning months, semaglutide provides unmatched convenience. However, its ultra-long half-life makes dose adjustments difficult and may not be suitable for studies requiring rapid washout.
Native GLP-1(7-36) amide remains superior for:
Mechanistic studies: requiring precise temporal control
Acute experiments: with defined start/stop times
Physiological research: modeling endogenous incretin function
Combination studies: where drug interactions must be minimized
Safety assessments: where immunogenicity is a concern
Synthetic analogs are preferable for:
Chronic studies: requiring sustained exposure
Behavioral research: where frequent dosing is impractical
Pharmacokinetic studies: requiring steady-state conditions
Translational research: modeling clinical therapeutic regimens
The choice between native GLP-1(7-36) amide and synthetic alternatives should be driven by research objectives, experimental timeline, and the need to model either physiological or therapeutic conditions.
What's Coming Next
Research on GLP-1(7-36) amide continues to expand beyond traditional metabolic applications, with several emerging areas showing significant promise.
Neuroprotection and Neurodegeneration: Recent studies have identified GLP-1 receptors throughout the central nervous system, leading to investigations of GLP-1(7-36) amide's potential in neurodegenerative diseases. McClean et al. (2011) demonstrated that the peptide crosses the blood-brain barrier and provides neuroprotection in models of Alzheimer's disease. Current trials are examining whether GLP-1-based therapies can slow cognitive decline in early dementia.
Cardiovascular Protection Mechanisms: While cardiovascular benefits of GLP-1 analogs are established clinically, the specific mechanisms remain under investigation. Bose et al. (2005) showed that GLP-1(7-36) amide directly improves endothelial function and reduces inflammatory markers. Ongoing research is exploring whether these effects are mediated through direct vascular GLP-1 receptors or secondary to metabolic improvements.
Addiction and Reward Pathways: Emerging evidence suggests GLP-1(7-36) amide modulates dopaminergic reward circuits in ways that extend beyond food intake. Dickson et al. (2012) demonstrated that GLP-1 receptor activation in the ventral tegmental area reduces alcohol consumption in rodent models. This has sparked interest in investigating the peptide's potential for treating substance use disorders.
Bone Metabolism and Osteoporosis: Recent discoveries of GLP-1 receptors in osteoblasts and osteoclasts have opened new research directions. Nuche-Berenguer et al. (2009) showed that GLP-1(7-36) amide promotes bone formation and reduces resorption markers. Clinical studies are now investigating whether incretin-based therapies can prevent osteoporosis in diabetic patients.
Hepatic Steatosis and NASH: Non-alcoholic fatty liver disease affects up to 30% of adults, and GLP-1-based therapies show promise for treatment. Cuthbertson et al. (2012) demonstrated that GLP-1(7-36) amide reduces hepatic lipid accumulation through direct effects on hepatocyte metabolism. Phase 2 trials are examining whether GLP-1 analogs can reverse established hepatic fibrosis.
Aging and Longevity Research: Preliminary evidence suggests GLP-1(7-36) amide may have anti-aging effects beyond metabolic benefits. The peptide's effects on cellular stress responses, autophagy, and mitochondrial function are being investigated as potential longevity mechanisms. Long-term studies in animal models are examining whether chronic GLP-1 receptor activation extends lifespan.
Precision Medicine Applications: Genetic variations in GLP-1 receptor expression and DPP-4 activity influence individual responses to incretin-based therapies. Pharmacogenomic studies are identifying biomarkers that predict response to GLP-1(7-36) amide and related compounds, potentially enabling personalized treatment approaches.
Novel Delivery Systems: The short half-life of GLP-1(7-36) amide has driven innovation in drug delivery. Researchers are developing nanoparticle formulations, implantable pumps, and even engineered bacteria that produce GLP-1 in the intestine. These approaches could enable sustained delivery of the native peptide without structural modifications.
Combination Therapy Optimization: Multi-hormone approaches combining GLP-1(7-36) amide with other incretin hormones, glucagon, or leptin are showing synergistic effects. The optimal combinations, ratios, and timing of multi-peptide therapies remain active areas of investigation.
Key questions driving future research include:
Can GLP-1-based neuroprotection prevent or slow Alzheimer's disease progression?
Do the cardiovascular benefits require continuous GLP-1 receptor activation or can intermittent dosing provide protection?
Which patient populations benefit most from incretin-based therapies?
Can combination approaches targeting multiple metabolic hormones provide superior outcomes?
What role does the gut microbiome play in GLP-1(7-36) amide production and response?
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
• GLP-1(7-36) amide is the naturally occurring, biologically active form of glucagon-like peptide-1, distinguished by its amidated C-terminus and 30-amino acid length
• The peptide produces glucose-dependent insulin secretion, increasing insulin release by 156-340% during hyperglycemia while showing minimal effects during normal glucose levels
• Extremely short half-life (2 minutes) requires continuous infusion or frequent dosing but provides precise temporal control for research applications
• Beyond glucose control, the peptide delays gastric emptying by 68% and reduces food intake by 12% through both peripheral and central nervous system mechanisms
• Research demonstrates beta cell preservation and proliferation effects, with studies showing 40-76% increases in beta cell mass and significant protection against apoptosis
• Safety profile is excellent with minimal hypoglycemia risk due to glucose-dependent mechanism, though gastrointestinal effects occur in 15-25% of subjects
• Combination protocols with GIP, DPP-4 inhibitors, or metformin provide synergistic effects and may allow dose reductions while maintaining efficacy
• The peptide serves as the gold standard for incretin research despite availability of longer-acting synthetic analogs for different experimental needs
• Emerging applications include neuroprotection, cardiovascular benefits, addiction research, and bone metabolism, expanding beyond traditional metabolic roles
• Future research directions focus on precision medicine approaches, novel delivery systems, and multi-hormone combination therapies for enhanced therapeutic outcomes
Related Articles on BuyPeptidesOnline.com
Semaglutide: The Weekly GLP-1 Analog Revolutionizing Diabetes and Weight Loss
Tirzepatide: The Dual GIP/GLP-1 Receptor Agonist Setting New Standards
Exenatide vs Liraglutide: Comparing First-Generation GLP-1 Analogs
DPP-4 Inhibitors and GLP-1: Understanding Incretin Enhancement Strategies
The Complete Guide to Incretin Hormones: GLP-1, GIP, and Metabolic Control