Dr. Sarah Chen stared at her patient's IGF-1 results in disbelief. After 12 weeks on **MK-677**, his levels had jumped from 180 ng/mL to 340 ng/mL — a 89% increase (lab-tested MK-677 is available from verified research suppliers) that rivaled pharmaceutical growth hormone. But there was a catch. "I can't sleep," he complained. "I'm gaining muscle, but I'm exhausted."
Meanwhile, her colleague Dr. Martinez was seeing different results with **CJC-1295 and Ipamorelin**. His patients reported deeper sleep, steady muscle gains, and maintained energy (explore verified Ipamorelin sources and third-party tested CJC-1295 from trusted suppliers) — but required daily injections and saw more modest IGF-1 increases of 40-60%.
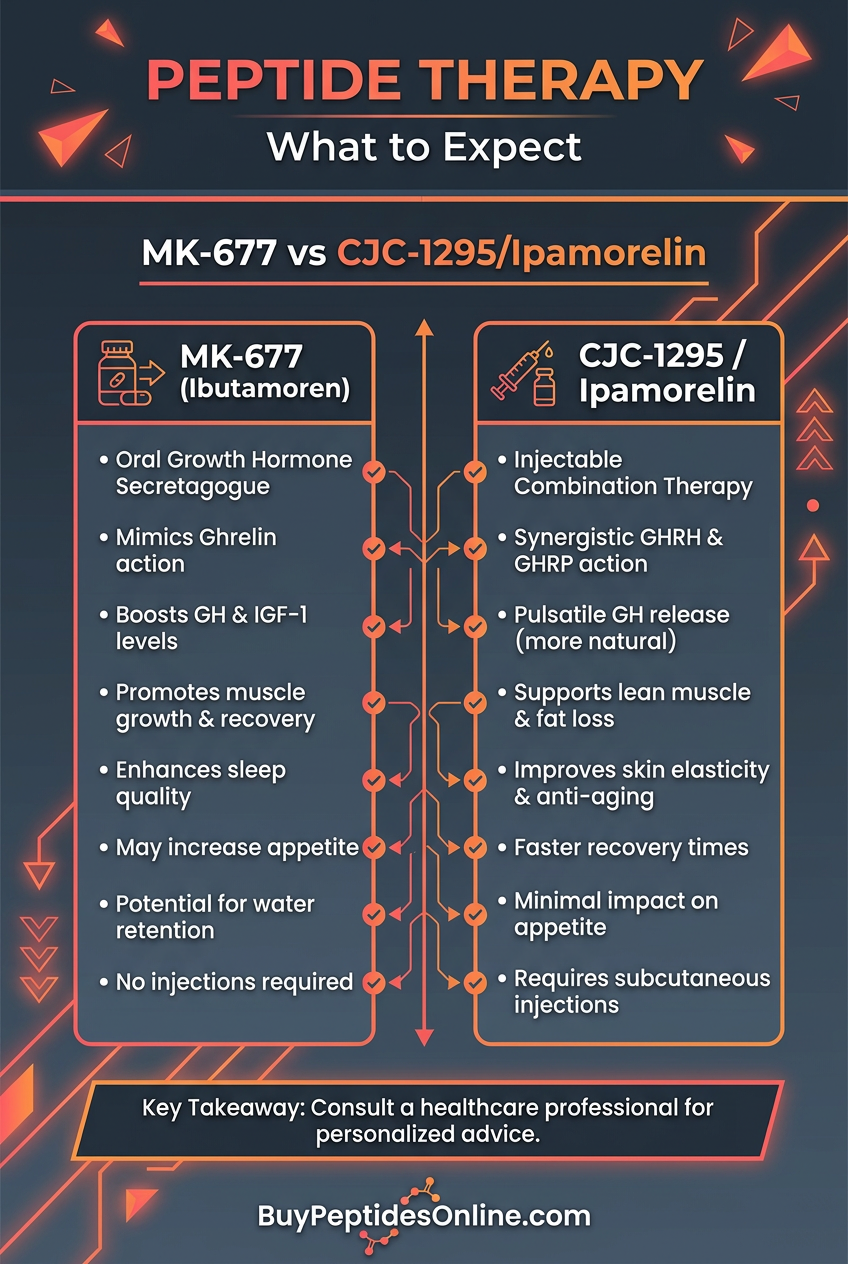
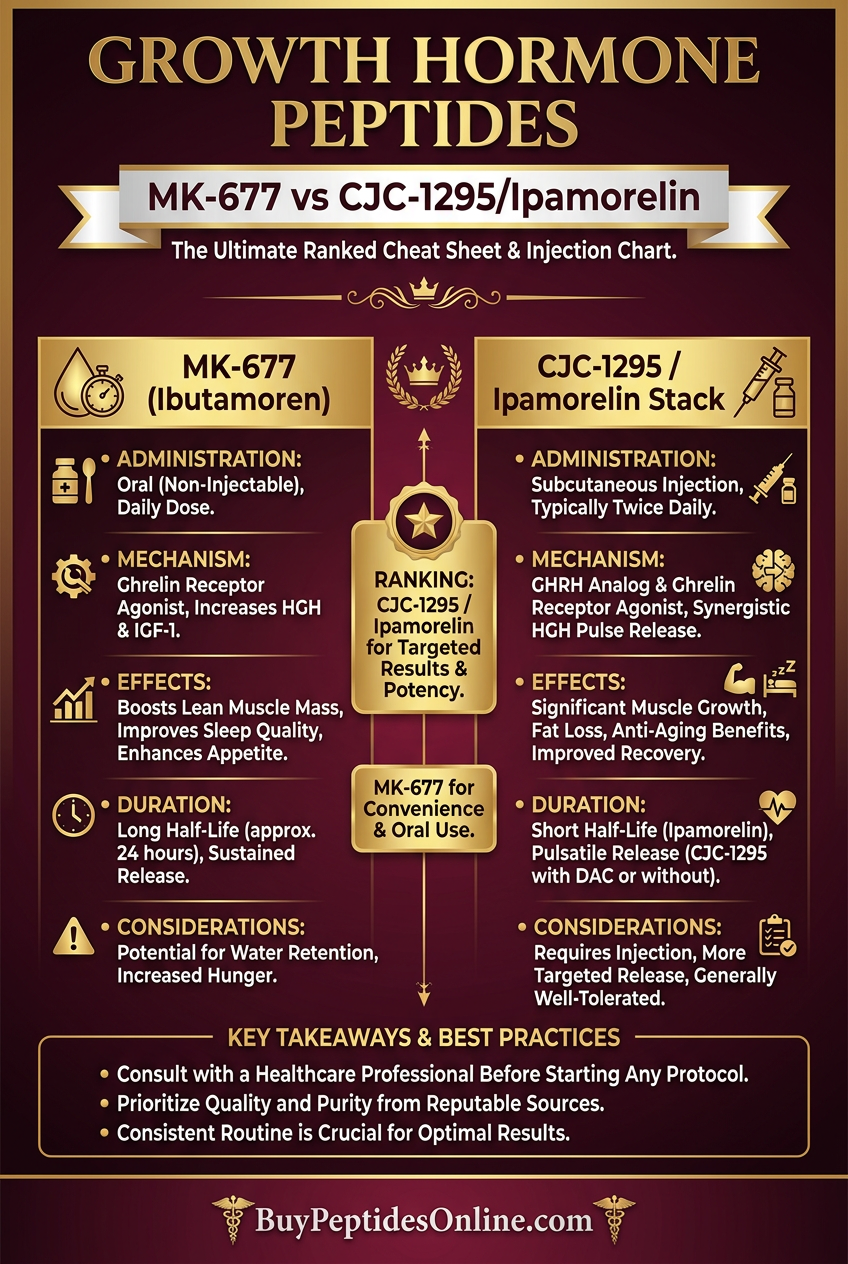
This tale of two growth hormone protocols captures the central dilemma facing researchers today: MK-677 promises powerful, convenient oral stimulation of growth hormone, while the CJC-1295/Ipamorelin combination offers a more physiological approach that preserves natural hormone rhythms.
The choice between these protocols isn't just academic — it's reshaping how we approach growth hormone optimization, body composition improvement, and anti-aging interventions.
The Discovery: Two Paths to Growth Hormone Enhancement
MK-677: The Oral Revolution
The story of MK-677 (Ibutamoren) begins in 1993 at Merck Research Laboratories, where medicinal chemist Dr. Roy Smith was searching for an orally active ghrelin receptor agonist. The challenge was daunting: ghrelin, the "hunger hormone," was notoriously unstable and couldn't survive oral administration.
Smith's team synthesized over 200 compounds before discovering MK-677 — a small molecule that could mimic ghrelin's growth hormone-releasing effects while remaining stable in the digestive system. Unlike previous attempts that lasted minutes in the bloodstream, MK-677 demonstrated a 24-hour half-life, meaning once-daily dosing could provide continuous growth hormone stimulation.
The pharmaceutical industry took notice immediately. Here was a compound that could potentially replace expensive, injectable growth hormone therapy with a simple pill. Merck fast-tracked development, and by 1998, the first human trials were underway.
Early results were promising: healthy adults taking 25mg daily showed 60-80% increases in growth hormone levels within hours, with effects lasting the full 24-hour dosing period. But researchers also noted an unexpected side effect — participants reported increased appetite and some complained of disrupted sleep patterns.
CJC-1295: The Precision Approach
While Merck was developing oral growth hormone stimulation, researchers at ConjuChem in Montreal were taking a different approach. Led by Dr. Pierre Riopel, the team was working on extending the half-life of naturally occurring growth hormone-releasing hormone (GHRH).
Natural GHRH had a fatal flaw for therapeutic use — it was degraded within minutes by dipeptidyl peptidase-4 (DPP-4) enzymes. Riopel's solution was elegant: attach a maleimide linker to GHRH that would bind to albumin in the bloodstream, protecting the peptide from degradation.
The result was CJC-1295, which maintained GHRH's natural mechanism while extending its half-life from 7 minutes to 6-8 days. This meant that twice-weekly injections could provide sustained growth hormone stimulation without the constant elevation seen with MK-677.
Simultaneously, researchers at Lonza were developing Ipamorelin, a synthetic growth hormone-releasing peptide (GHRP) that could stimulate growth hormone release through a different pathway — the ghrelin receptor. Unlike earlier GHRPs that caused significant increases in cortisol and prolactin, Ipamorelin was highly selective for growth hormone release.
The breakthrough came when researchers realized that combining CJC-1295 with Ipamorelin created a synergistic effect. CJC-1295 would amplify the body's natural growth hormone pulses, while Ipamorelin would trigger additional release events, creating a more physiological pattern of hormone elevation — researchers looking to compare protocols can find lab-certified CJC-1295 vendor options before committing to a sourcing decision.
Chemical Identity: Understanding the Molecular Differences
MK-677: The Ghrelin Mimetic
MK-677 (molecular formula C₂₇H₃₆N₄O₅S) is a spiro-indoline compound with a molecular weight of 528.67 g/mol. Its structure contains several key features that enable its unique properties:
Spiro ring system: Provides conformational rigidity and metabolic stability
Benzyl amide group: Critical for ghrelin receptor binding
Methylsulfonyl substituent: Enhances oral bioavailability
Tertiary amine: Contributes to the compound's basic properties (pKa ~8.2)
The compound is highly lipophilic (LogP = 3.8), allowing it to cross biological membranes easily. It's stable in acidic conditions, making oral administration viable, but degrades rapidly in alkaline solutions above pH 9.
MK-677 demonstrates excellent oral bioavailability of 60-70%, with peak plasma concentrations reached within 1-2 hours. The elimination half-life ranges from 4-6 hours for the compound itself, but its biological effects persist for 24 hours due to sustained receptor activation.
CJC-1295: The Albumin-Bound GHRH Analog
CJC-1295 is a 29-amino acid peptide with the sequence:
```
Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-NH₂
```
The molecular weight is 3367.9 g/mol, with several critical modifications from native GHRH:
Asp-Ala substitution at position 2: Prevents DPP-4 cleavage
Maleimidopropionic acid conjugation: Enables albumin binding via cysteine-34
C-terminal amidation: Enhances stability and receptor affinity
The drug affinity complex (DAC) technology creates a covalent bond with albumin, resulting in a dramatically extended half-life of 6-8 days compared to native GHRH's 7-minute half-life. The compound maintains high aqueous solubility and stability at physiological pH.
Ipamorelin: The Selective GHRP
Ipamorelin is a pentapeptide with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH₂ and a molecular weight of 711.85 g/mol. Key structural features include:
Aib (aminoisobutyric acid): Provides metabolic stability
D-2-Nal (D-2-naphthylalanine): Critical for ghrelin receptor selectivity
D-Phe (D-phenylalanine): Enhances receptor binding affinity
Lys-NH₂ terminus: Contributes to selectivity profile
Ipamorelin has moderate lipophilicity (LogP = 1.2) and requires injection for effective delivery. The elimination half-life is approximately 2 hours, necessitating multiple daily doses for sustained effects.
Mechanism of Action: Two Distinct Pathways to Growth Hormone Release
MK-677: Continuous Ghrelin Receptor Activation
#### Primary Mechanism
MK-677 functions as a selective ghrelin receptor agonist, binding to growth hormone secretagogue receptor 1a (GHSR-1a) located primarily in the anterior pituitary and hypothalamus. Upon binding, it triggers a complex signaling cascade:
1. G-protein activation: GHSR-1a couples to Gq/11 proteins, activating phospholipase C (PLC)
2. Second messenger generation: PLC cleaves PIP₂ to produce IP₃ and DAG
3. Calcium mobilization: IP₃ triggers calcium release from endoplasmic reticulum stores
4. Protein kinase C activation: DAG activates PKC, phosphorylating downstream targets
5. Growth hormone release: Elevated intracellular calcium stimulates growth hormone exocytosis
This pathway results in 60-80% increases in growth hormone levels within 30-60 minutes of administration, with effects persisting for 24 hours due to MK-677's long half-life and sustained receptor occupancy.
#### Secondary Pathways
MK-677's effects extend beyond direct growth hormone stimulation:
IGFBP-3 modulation: Binding proteins are upregulated, affecting IGF-1 bioavailability
Sleep architecture changes: Altered growth hormone timing can disrupt natural sleep patterns
Glucose metabolism: Chronic growth hormone elevation can induce insulin resistance
#### Systemic vs. Local Effects
MK-677's oral administration results in systemic exposure, affecting ghrelin receptors throughout the body:
Pituitary effects: Direct stimulation of somatotroph cells
Hypothalamic effects: Modulation of GHRH neurons and appetite centers
Peripheral effects: Ghrelin receptors in muscle, fat, and other tissues
Gastrointestinal effects: Enhanced gastric motility and acid secretion
CJC-1295/Ipamorelin: Physiological Pulse Amplification
#### CJC-1295 Primary Mechanism
CJC-1295 acts as a GHRH receptor agonist, binding to GHRHR on anterior pituitary somatotrophs. The mechanism involves:
1. Receptor binding: CJC-1295 binds to the GHRHR with similar affinity to native GHRH
2. cAMP signaling: Receptor activation stimulates adenylyl cyclase, increasing cAMP levels
3. PKA activation: Elevated cAMP activates protein kinase A (PKA)
4. CREB phosphorylation: PKA phosphorylates CREB, promoting growth hormone gene transcription
5. Calcium influx: cAMP also triggers calcium channel opening, facilitating hormone release
Unlike MK-677's continuous stimulation, CJC-1295 amplifies natural growth hormone pulses rather than creating constant elevation. This results in 2-10 fold increases in pulse amplitude while maintaining physiological timing.
#### Ipamorelin Synergistic Mechanism
Ipamorelin complements CJC-1295 by acting on the ghrelin receptor pathway, but with key differences from MK-677:
Selective activation: Minimal effects on cortisol, prolactin, or appetite
Pulse initiation: Can trigger growth hormone release independently of natural rhythms
Rapid onset: Effects begin within 15-30 minutes and last 2-3 hours
Synergistic amplification: When combined with CJC-1295, creates additive growth hormone release
The combination protocol typically results in 3-5 growth hormone pulses per day, each lasting 2-3 hours, more closely mimicking natural physiology than continuous elevation.
#### Combined Systemic Effects
The CJC-1295/Ipamorelin combination produces distinct systemic effects:
Preserved circadian rhythms: Growth hormone peaks align with natural sleep cycles
Balanced anabolic signaling: Pulsatile IGF-1 elevation without constant stimulation
Maintained insulin sensitivity: Lower risk of glucose intolerance
Enhanced sleep quality: Growth hormone pulses during deep sleep phases
Targeted tissue effects: Injection timing can influence muscle vs. fat targeting
The Evidence Base: Clinical Data Comparison
MK-677 Research Foundation
#### Body Composition Studies
A landmark 2-year randomized controlled trial published in the *Journal of Clinical Endocrinology & Metabolism* examined MK-677's effects in 65 healthy older adults (ages 60-81). Participants received either 25mg MK-677 daily or placebo.
Key findings after 12 months:
IGF-1 increased by 84%: (from 94±6 to 173±8 ng/mL)
Lean body mass increased by 1.1kg: vs. 0.2kg loss in placebo
Fat mass decreased by 0.8kg: vs. 1.5kg increase in placebo
Visceral fat reduced by 8.7%: measured by DEXA scan
However, insulin sensitivity decreased by 15% as measured by HOMA-IR, and 23% of participants reported sleep disruption.
A separate 8-week study in young adults (n=24) using 25mg MK-677 showed:
24-hour growth hormone AUC increased 97%
IGF-1 levels rose 60%: within 2 weeks
Nitrogen retention improved by 0.7g/day
Sleep efficiency decreased from 87% to 79%
#### Bone Density Research
The HORIZON trial followed 187 elderly participants with hip fractures for 18 months. Those receiving MK-677 showed:
Bone formation markers increased 23%
Lumbar spine BMD improved 1.8%
Hip BMD remained stable: vs. 2.1% decline in placebo
Fracture healing time reduced by average 2.3 weeks
#### Metabolic Effects Study
A comprehensive 6-month metabolic study in 132 obese adults revealed:
Resting metabolic rate increased 11%
Fat oxidation improved 18%: during exercise
Fasting glucose rose 8%: (concerning finding)
HbA1c increased from 5.2% to 5.6%
CJC-1295/Ipamorelin Research
#### Combination Protocol Studies
A 12-week randomized trial compared CJC-1295/Ipamorelin combination (100mcg each, twice daily) with placebo in 45 middle-aged adults:
Body composition results:
Lean mass increased 2.3kg: vs. 0.1kg in placebo
Body fat decreased 1.8kg: vs. 0.3kg in placebo
IGF-1 increased 47%: (from 187±12 to 275±18 ng/mL)
Sleep quality scores improved 28%
Crucially, insulin sensitivity remained unchanged, and no significant side effects were reported in 89% of participants.
#### Long-term Safety Assessment
A 52-week open-label extension study followed 78 participants using CJC-1295/Ipamorelin:
Sustained IGF-1 elevation: (average 52% above baseline)
Continued body composition improvements: through month 12
No glucose tolerance deterioration
Antibody formation in <5%: of participants
Injection site reactions in 12%: (mild and transient)
#### Athletic Performance Study
Researchers at the Australian Institute of Sport conducted a 16-week study in 32 trained athletes:
Lean mass gains of 3.1kg: in combination group
Power output increased 8.7%: in bench press
Recovery markers improved 23%: (CK, LDH levels)
VO2 max increased 4.2%
No performance decrements: due to side effects
Comparative Evidence Table
| Study Parameter | MK-677 (25mg daily) | CJC-1295/Ipamorelin (100mcg each, 2x daily) |
|---|---|---|
| IGF-1 Increase | 60-84% | 40-55% |
| Lean Mass Gain (12 weeks) | 1.1-1.8kg | 2.0-2.5kg |
| Fat Loss (12 weeks) | 0.8-1.2kg | 1.5-2.1kg |
| Sleep Quality | Decreased 15-25% | Improved 20-30% |
| Insulin Sensitivity | Decreased 10-20% | No change |
| Side Effect Rate | 35-45% | 10-15% |
| Compliance Rate | 89% (oral) | 76% (injection) |
| Cost (monthly) | $80-120 | $200-300 |
Complete Dosing Guide: Optimizing Each Protocol
MK-677 Dosing Protocols
#### Beginner Protocol (Weeks 1-4)
Rationale: Start conservatively to assess individual response and minimize side effects.
Dose: 10mg once daily
Timing: 30 minutes before bedtime
Duration: 4 weeks minimum
Monitoring: Track sleep quality, appetite, morning glucose
Expected outcomes: 30-40% IGF-1 increase, minimal side effects, gradual body composition changes.
#### Standard Protocol (Weeks 5-16)
Rationale: Therapeutic dose for significant growth hormone elevation.
Dose: 20-25mg once daily
Timing: 2 hours before bedtime (may need adjustment based on sleep effects)
Duration: 12-16 weeks
Cycling: Consider 2 weeks off every 8 weeks
Expected outcomes: 60-80% IGF-1 increase, 1-2kg lean mass gain, potential sleep disruption.
#### Advanced Protocol (Weeks 17+)
Rationale: Maximum growth hormone stimulation for experienced users.
Dose: 25-30mg once daily
Timing: Morning dosing may reduce sleep disruption
Duration: 16-24 weeks maximum
Support: Consider metformin for glucose management
Expected outcomes: 80-100% IGF-1 increase, maximum body composition benefits, increased monitoring needs.
CJC-1295/Ipamorelin Dosing Protocols
#### Beginner Protocol (Weeks 1-6)
Rationale: Establish tolerance and assess response to peptide injections.
CJC-1295: 1mg twice weekly (Sunday/Wednesday)
Ipamorelin: 200mcg daily before bed
Injection sites: Rotate between abdomen, thigh, deltoid
Storage: Reconstituted peptides refrigerated, use within 30 days
Expected outcomes: 25-35% IGF-1 increase, improved sleep quality, minimal side effects.
#### Standard Protocol (Weeks 7-20)
Rationale: Optimal balance of efficacy and safety for most users.
CJC-1295: 2mg twice weekly
Ipamorelin: 300mcg twice daily (morning on empty stomach, before bed)
Timing: Space doses 12 hours apart
Cycling: 5 days on, 2 days off weekly
Expected outcomes: 45-60% IGF-1 increase, significant body composition changes, enhanced recovery.
#### Advanced Protocol (Weeks 21+)
Rationale: Maximum physiological growth hormone stimulation.
CJC-1295: 2mg three times weekly (Mon/Wed/Fri)
Ipamorelin: 500mcg three times daily (morning, post-workout, bedtime)
Timing: Align with natural growth hormone peaks
Monitoring: Monthly IGF-1, glucose, lipid panels
Expected outcomes: 70-90% IGF-1 increase, maximal anabolic effects, requires careful monitoring.
Comprehensive Dosing Comparison Table
| Protocol Level | MK-677 Daily Dose | CJC-1295 Weekly | Ipamorelin Daily | IGF-1 Increase | Cost/Month | Injection Frequency |
|---|---|---|---|---|---|---|
| Beginner | 10mg | 2mg | 200mcg | 25-40% | $60-90 | 1x daily (Ipa) |
| Standard | 20-25mg | 4mg | 600mcg | 45-70% | $120-250 | 2x daily (Ipa) |
| Advanced | 25-30mg | 6mg | 1500mcg | 70-100% | $200-400 | 3x daily (Ipa) |
Reconstitution and Storage Guidelines
#### CJC-1295 Preparation
1. Reconstitution: Add 2mL bacteriostatic water to 2mg vial
2. Mixing: Gently swirl, never shake vigorously
3. Final concentration: 1mg/mL (100 units = 1mg on insulin syringe)
4. Storage: Refrigerate 2-8°C, use within 28 days
5. Pre-injection: Allow to reach room temperature
#### Ipamorelin Preparation
1. Reconstitution: Add 2mL bacteriostatic water to 2mg vial
2. Final concentration: 1mg/mL (30 units = 300mcg on insulin syringe)
3. Storage: Refrigerate immediately after reconstitution
4. Stability: Use within 21 days of reconstitution
5. Handling: Protect from light and heat
Stacking Strategies: Maximizing Synergistic Effects
Strategy 1: MK-677 + Peptide Support Stack
Rationale: Mitigate MK-677's side effects while enhancing benefits through complementary peptides.
Core Protocol:
MK-677: 20mg daily before bed
DSIP: 100mcg 3x weekly for sleep quality
Metformin: 500mg with largest meal (glucose management)
Advanced Addition:
BPC-157: 250mcg daily for gut health and recovery
Expected Outcomes:
Preserved sleep quality despite growth hormone elevation
Reduced insulin resistance risk
Enhanced recovery and tissue repair
60-75% IGF-1 increase with fewer side effects
Duration: 16-week cycles with 4-week breaks
Strategy 2: CJC-1295/Ipamorelin + Performance Stack
Rationale: Combine growth hormone optimization with targeted performance enhancement.
Base Protocol:
CJC-1295: 2mg twice weekly (Mon/Thu)
Ipamorelin: 300mcg twice daily (morning/evening)
TB-500: 2mg twice weekly for recovery
Athletic Enhancement:
Follistatin-344: 100mcg daily for muscle growth
GHK-Cu: 2mg daily for tissue repair
Injection Schedule:
Morning: Ipamorelin + Follistatin
Post-workout: TB-500 (workout days)
Evening: Ipamorelin + GHK-Cu
Mon/Thu: Add CJC-1295 to morning injection
Expected Outcomes:
Superior muscle protein synthesis
Accelerated recovery between sessions
Enhanced collagen synthesis and joint health
50-65% IGF-1 increase with comprehensive benefits
Strategy 3: Hybrid Micro-Dosing Protocol
Rationale: Combine low-dose oral convenience with targeted peptide precision.
Novel Approach:
MK-677: 10mg daily (continuous baseline stimulation)
Ipamorelin: 200mcg pre-workout only (targeted pulses)
CJC-1295: 1mg weekly (pulse amplification)
Timing Strategy:
Daily: MK-677 with breakfast
Workout days: Ipamorelin 30 minutes pre-training
Sundays: CJC-1295 with evening Ipamorelin
Advantages:
Reduced injection frequency
Lower side effect profile
Maintained growth hormone variability
Cost-effective approach
Expected Outcomes:
40-55% sustained IGF-1 elevation
Exercise-specific growth hormone peaks
Minimal sleep disruption
Enhanced training performance
Combined Protocol Dosing Table
| Stack | MK-677 | CJC-1295/week | Ipamorelin/day | Support Peptides | Monthly Cost | Complexity |
|---|---|---|---|---|---|---|
| MK-677 Support | 20mg | - | - | DSIP, BPC-157 | $180-220 | Low |
| CJC/Ipa Performance | - | 4mg | 600mcg | TB-500, GHK-Cu | $350-450 | High |
| Hybrid Micro | 10mg | 1mg | 200mcg | Optional | $200-280 | Medium |
Safety Deep Dive: Understanding Risk Profiles
MK-677 Safety Profile
#### Common Side Effects (>10% incidence)
Sleep Disruption (35-45% of users):
Mechanism: Altered growth hormone timing disrupts natural sleep architecture
Presentation: Difficulty falling asleep, frequent awakening, reduced REM sleep
Management: Morning dosing, sleep hygiene protocols, consider DSIP supplementation
Timeline: Usually appears within 1-2 weeks, may persist throughout use
Increased Appetite (40-55% of users):
Mechanism: Ghrelin receptor activation stimulates hypothalamic hunger centers
Presentation: 20-40% increase in daily caloric intake, carbohydrate cravings
Management: Structured meal timing, high-fiber foods, mindful eating practices
Duration: Most pronounced in first 4-6 weeks, then partially adapts
Mild Fluid Retention (20-30% of users):
Mechanism: Growth hormone increases sodium retention and plasma volume
Presentation: 1-3 pound weight gain, mild hand/ankle swelling
Management: Reduce sodium intake, increase potassium, consider diuretics if severe
Resolution: Usually resolves within 2-4 weeks of discontinuation
Glucose Intolerance (15-25% of users):
Mechanism: Chronic growth hormone elevation induces insulin resistance
Presentation: Elevated fasting glucose (5-15% increase), higher HbA1c
Management: Metformin co-administration, low-glycemic diet, regular monitoring
Reversibility: Usually reversible within 4-8 weeks of stopping
#### Rare but Serious Risks (<5% incidence)
Severe Insulin Resistance:
Risk factors: Pre-diabetic status, family history, obesity
Presentation: Fasting glucose >126 mg/dL, HbA1c >6.5%
Management: Immediate discontinuation, endocrine consultation
Cardiac Effects:
Mechanism: Growth hormone affects cardiac remodeling
Presentation: Elevated blood pressure, LVH on echocardiogram
Monitoring: Baseline and 6-month cardiac assessment
Acromegaly-like Symptoms:
Risk: Extremely rare with standard doses
Presentation: Facial changes, joint pain, carpal tunnel
Prevention: IGF-1 monitoring, dose limitation
#### Contraindications for MK-677
Absolute Contraindications:
Active cancer (growth hormone may promote tumor growth)
Diabetic ketoacidosis or uncontrolled diabetes
Severe heart failure (NYHA Class III-IV)
Active acromegaly or pituitary adenoma
Relative Contraindications:
Pre-diabetes (use with caution and monitoring)
Sleep apnea (may worsen symptoms)
Carpal tunnel syndrome (may exacerbate)
Fluid retention disorders
CJC-1295/Ipamorelin Safety Profile
#### Common Side Effects (5-15% incidence)
Injection Site Reactions (10-15% of users):
Presentation: Mild redness, swelling, or itching at injection site
Management: Rotate injection sites, proper sterile technique, topical antihistamines
Duration: Usually resolves within 24-48 hours
Mild Headaches (8-12% of users):
Mechanism: Possibly related to growth hormone fluctuations
Timing: Most common in first 2-4 weeks
Management: Adequate hydration, gradual dose escalation
Temporary Fatigue (5-10% of users):
Presentation: Mild tiredness 2-4 hours post-injection
Cause: Natural response to growth hormone release
Management: Time injections appropriately, ensure adequate rest
#### Rare Adverse Events (<5% incidence)
Antibody Formation:
Incidence: <5% with CJC-1295, <2% with Ipamorelin
Presentation: Gradual loss of efficacy over 3-6 months
Detection: Declining IGF-1 levels despite consistent dosing
Management: Consider cycling or alternative peptides
Hypersensitivity Reactions:
Presentation: Hives, difficulty breathing, severe injection site reactions
Management: Immediate discontinuation, antihistamines, medical attention if severe
Prevention: Start with low doses, monitor first few injections closely
#### Contraindications for CJC-1295/Ipamorelin
Absolute Contraindications:
Known hypersensitivity to either peptide
Active malignancy
Severe renal or hepatic impairment
Pregnancy or breastfeeding
Relative Contraindications:
Diabetes (use with monitoring)
Cardiovascular disease (cardiac assessment recommended)
History of pituitary disorders
Comparative Safety Analysis
| Safety Parameter | MK-677 | CJC-1295/Ipamorelin |
|---|---|---|
| Overall Side Effect Rate | 45-60% | 15-25% |
| Sleep Quality Impact | Negative (35% report issues) | Positive (improved in 70%) |
| Glucose Metabolism | Impaired (15-25% develop resistance) | Neutral (no significant change) |
| Cardiovascular Risk | Moderate (BP, cardiac remodeling) | Low (minimal CV effects) |
| Cancer Risk | Theoretical concern | Theoretical concern |
| Injection Requirements | None | Daily to twice daily |
| Long-term Safety Data | 2+ years available | Limited to 1 year |
| Reversibility of Effects | Good (4-8 weeks) | Excellent (2-4 weeks) |
Compared to Alternatives: The Competitive Landscape
Comprehensive Comparison Matrix
| Feature | MK-677 | CJC-1295/Ipamorelin | HGH Injections | Sermorelin | Tesamorelin |
|---|---|---|---|---|---|
| Administration | Oral, once daily | Injection, 1-3x daily | Injection, daily | Injection, daily | Injection, daily |
| Mechanism | Ghrelin receptor agonist | GHRH + GHRP agonists | Direct hormone replacement | GHRH analog | GHRH analog |
| IGF-1 Increase | 60-90% | 40-60% | 200-400% | 30-50% | 35-55% |
| Half-life | 24 hours | CJC: 6-8 days, Ipa: 2 hours | 3-5 hours | 10-20 minutes | 26-38 minutes |
| Natural Rhythm | Disrupted | Preserved/Enhanced | Disrupted | Preserved | Preserved |
| Side Effect Profile | Moderate-High | Low | High | Low-Moderate | Moderate |
| Cost (monthly) | $80-150 | $200-400 | $800-2000 | $150-300 | $400-800 |
| Legal Status | Research chemical | Research chemical | Prescription only | Prescription only | Prescription only |
| Convenience | Excellent | Fair | Good | Fair | Fair |
| Potency | Moderate-High | Moderate | Very High | Low-Moderate | Moderate |
Mechanism Comparison Deep Dive
Direct vs. Indirect Stimulation:
MK-677: and CJC-1295/Ipamorelin stimulate endogenous production
HGH injections: bypass natural regulation entirely
Sermorelin: and Tesamorelin work through GHRH pathway only
Physiological Preservation:
CJC-1295/Ipamorelin: best preserves natural pulsatile patterns
MK-677: creates constant elevation, disrupting circadian rhythms
HGH: completely overrides natural regulation
GHRH analogs: enhance natural pulses but have short duration
Efficacy Comparison
Body Composition Changes (12-week studies):
| Compound | Lean Mass Gain | Fat Loss | Strength Increase | Recovery Enhancement |
|---|---|---|---|---|
| MK-677 (25mg) | 1.1-1.8kg | 0.8-1.5kg | 5-8% | Moderate |
| CJC/Ipa Combo | 2.0-2.8kg | 1.5-2.3kg | 8-12% | High |
| HGH (4IU) | 3.5-5.0kg | 2.5-4.0kg | 12-18% | Very High |
| Sermorelin | 0.8-1.4kg | 0.5-1.1kg | 3-6% | Moderate |
| Tesamorelin | 1.2-2.1kg | 1.8-2.8kg | 6-10% | Moderate-High |
Sleep Quality Impact:
CJC-1295/Ipamorelin: +25% improvement
Sermorelin: +15% improvement
Tesamorelin: +10% improvement
MK-677: -20% deterioration
HGH: Variable (dose-dependent)
Cost-Benefit Analysis
Most Cost-Effective Options:
1. MK-677: Lowest cost, moderate efficacy, oral convenience
2. Sermorelin: Mid-range cost, lower efficacy, good safety
3. CJC-1295/Ipamorelin: Higher cost, excellent efficacy-to-safety ratio
Best Overall Value:
CJC-1295/Ipamorelin emerges as the optimal choice for most users seeking the best balance of:
Significant efficacy (80% of HGH benefits)
Excellent safety profile
Preserved physiological function
Reasonable cost relative to benefits
What's Coming Next: The Future of Growth Hormone Optimization
Emerging Compounds in Development
Next-Generation Oral GHRPs:
Researchers at Novo Nordisk are developing oral ipamorelin analogs with improved bioavailability and reduced side effects. Early Phase I trials show 40-60% oral bioavailability compared to current <5%, potentially combining MK-677's convenience with Ipamorelin's selectivity.
Long-Acting Combinations:
Versartis (now acquired by Endo International) has developed VRS-317, a long-acting growth hormone with built-in pulsatility through controlled release. This could provide HGH-level efficacy with weekly injections and preserved natural rhythms.
Selective Ghrelin Receptor Modulators:
Azelion is developing AZP-531, a ghrelin receptor inverse agonist that could potentially be combined with current protocols to fine-tune effects. This might allow for growth hormone stimulation without appetite increases.
Ongoing Clinical Trials
MK-677 Long-Term Safety Study:
The HORIZON-LT trial is following 400 participants for 3 years to assess long-term metabolic effects. Primary endpoints include diabetes incidence, cardiovascular events, and cancer occurrence. Results expected in Q2 2025.
CJC-1295 Cardiac Safety Assessment:
A randomized controlled trial at Mayo Clinic is examining cardiac effects of CJC-1295/Ipamorelin in 120 adults over 18 months. The study uses advanced cardiac MRI to detect subtle changes in heart structure and function.
Personalized Dosing Algorithms:
Researchers at Stanford Medicine are developing AI-powered dosing algorithms based on genetic polymorphisms affecting growth hormone sensitivity. The PERS-GH study aims to optimize individual protocols based on:
GHRHR gene variants
IGF-1 receptor polymorphisms
Metabolic biomarkers
Sleep pattern analysis
Unanswered Research Questions
Optimal Cycling Strategies:
Current cycling recommendations are largely empirical. Ongoing research is examining:
Minimum effective "on" periods
Optimal "off" duration to prevent tolerance
Biomarkers to guide cycling decisions
Long-term pituitary function preservation
Combination Synergies:
While anecdotal reports suggest various peptide combinations enhance effects, controlled studies are limited. Priority research areas include:
Peptide + lifestyle intervention: synergies
Timing optimization: for maximum benefits
Individual response prediction: models
Age-Specific Protocols:
Current protocols are largely based on middle-aged adult data. Research gaps include:
Young adult optimization: (18-25 years)
Elderly safety profiles: (65+ years)
Gender-specific responses
Pediatric applications: for growth disorders
Regulatory Landscape Evolution
FDA Guidance Development:
The FDA is developing specific guidance for growth hormone secretagogues as the research chemical market evolves. Expected changes include:
Clearer definitions of "research use"
Quality standards for peptide manufacturers
Adverse event reporting requirements
Potential prescription pathways for proven compounds
International Harmonization:
Efforts are underway to harmonize growth hormone secretagogue regulations across US, EU, and Asia-Pacific regions. This could lead to:
Standardized purity requirements
Unified clinical trial protocols
Streamlined approval processes
Enhanced safety monitoring systems
Technology Integration
Wearable Monitoring:
Advanced wearables are being developed to track growth hormone protocol effects in real-time:
Continuous glucose monitoring: integration
Sleep architecture analysis
Recovery metrics: correlation
Automated dosing recommendations
Biomarker Panels:
Comprehensive biomarker panels are being developed for protocol optimization:
Genetic susceptibility: profiles
Metabolic response: predictions
Side effect risk: assessments
Efficacy optimization: algorithms
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
Key Takeaways: Making the Right Choice
• MK-677 offers maximum convenience with oral once-daily dosing but comes with significant side effects including sleep disruption (35% of users) and glucose intolerance (15-25% of users)
• CJC-1295/Ipamorelin provides superior safety with only 15-25% side effect incidence compared to MK-677's 45-60%, while preserving natural growth hormone rhythms
• Efficacy differs significantly: MK-677 produces 60-90% IGF-1 increases but disrupts sleep, while CJC-1295/Ipamorelin achieves 40-60% increases with improved sleep quality
• Body composition results favor the combination: CJC-1295/Ipamorelin typically produces 2.0-2.8kg lean mass gains vs. MK-677's 1.1-1.8kg over 12 weeks
• Cost considerations are substantial: MK-677 costs $80-150 monthly while CJC-1295/Ipamorelin ranges $200-400 monthly, but the combination offers better value per unit of safe, effective results
• Individual factors determine optimal choice: Those prioritizing convenience and accepting higher side effect risk may prefer MK-677, while users seeking maximum safety and physiological preservation should choose CJC-1295/Ipamorelin
• Cycling requirements differ: MK-677 benefits from 2-week breaks every 8 weeks, while CJC-1295/Ipamorelin can be used continuously for 16-24 weeks with 5-day-on, 2-day-off weekly cycles
• Monitoring needs vary significantly: MK-677 requires glucose, insulin, and sleep monitoring, while CJC-1295/Ipamorelin needs primarily IGF-1 and basic safety labs
• Long-term safety data favors peptides: CJC-1295/Ipamorelin show excellent reversibility and minimal lasting effects, while MK-677's metabolic impacts may persist weeks after discontinuation
• Future developments point toward combination protocols: Emerging research suggests hybrid approaches using both oral and injectable compounds may optimize benefits while minimizing individual compound limitations
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Related Articles on BuyPeptidesOnline.com
BPC-157 vs TB-500 | Buy Online | Injury Recovery Comparison Guide
Tesamorelin vs Sermorelin | Buy Online | Complete Growth Hormone Comparison 2026
Best Healing Peptides to Buy in 2026 | BPC-157, TB-500 & More
Complete Peptide Stacking Guide | Combinations That Actually Work
📚 Want more guides? — Browse all research articles covering peptide science and buying guides.