Dr. Sarah Chen stared at her patient's lab results with amazement. After eight weeks of **MK-677 treatment, the 45-year-old executive's IGF-1 levels had jumped from 180 ng/mL to 285 ng/mL—a 58% increase that translated to visibly improved muscle tone, deeper sleep, and renewed energy. But when her colleague down the hall showed similar results using CJC-1295 with Ipamorelin, Chen realized she was witnessing something profound: two fundamentally different approaches to growth hormone optimization** were producing comparable benefits through entirely distinct mechanisms.
This wasn't just about choosing between peptides. It was about understanding how the body's most powerful anabolic hormone could be enhanced through either constant stimulation or carefully timed pulses—each strategy carrying unique advantages, risks, and practical considerations that could make or break a research protocol.
The Discovery: Two Paths to Growth Hormone Enhancement
The story of these competing approaches begins in separate laboratories, decades apart, with researchers pursuing the same goal through radically different strategies.
MK-677's origin traces back to Merck's laboratories in the 1990s, where scientists led by Dr. Roy Smith were investigating ghrelin receptor agonists. They weren't initially focused on growth hormone—they were studying appetite regulation and metabolic disorders. The breakthrough came when they synthesized Ibutamoren (MK-677), a small molecule that could perfectly mimic ghrelin's effects on the growth hormone-releasing hormone (GHRH) system. Those sourcing this compound for research can compare MK-677 pricing from trusted suppliers.
Unlike natural ghrelin, which has a half-life of mere minutes, MK-677 demonstrated remarkable stability. Early studies showed it could maintain elevated growth hormone and IGF-1 levels for over 24 hours from a single oral dose—something previously impossible without continuous peptide infusions.
The CJC-1295 story unfolds differently, emerging from ConjuChem's Montreal facility in the early 2000s. Dr. Éric Thibaudeau's team was tackling a fundamental problem: natural GHRH (growth hormone-releasing hormone) has a half-life of only 7 minutes in human plasma, making therapeutic applications nearly impossible.
Their solution was elegant—they attached a Drug Affinity Complex (DAC) to the GHRH molecule, extending its half-life to approximately 8 days. This modification allowed for weekly injections while maintaining the natural pulsatile pattern of growth hormone release that evolution had optimized over millions of years.
Ipamorelin emerged from Novo Nordisk's research into growth hormone-releasing peptides (GHRPs) in the late 1990s. Unlike earlier GHRPs that caused significant increases in cortisol and prolactin, Ipamorelin demonstrated remarkable selectivity for growth hormone release while minimizing unwanted hormonal side effects.
When researchers began combining CJC-1295 with Ipamorelin, they discovered synergistic effects. The GHRH analog provided the signal for growth hormone release, while the GHRP amplified that signal through a separate receptor pathway—creating what many consider the gold standard for physiological growth hormone enhancement. Researchers looking to explore this combination can find lab-tested CJC-1295 from verified vendors and source research-grade Ipamorelin through trusted suppliers.
Chemical Identity: Molecular Architecture Determines Function
Understanding these compounds' chemical structures reveals why they behave so differently in the human body.
MK-677 (Ibutamoren) is a non-peptide growth hormone secretagogue with the molecular formula C27H36N4O5S and a molecular weight of 528.662 g/mol. Its structure mimics ghrelin, the "hunger hormone," but with crucial modifications that provide oral bioavailability and extended half-life.
The molecule features a spiro-indoline core connected to a benzyl ether side chain. This unique architecture allows it to bind selectively to the ghrelin receptor (GHSR-1a) in the pituitary gland and hypothalamus. Unlike natural ghrelin, MK-677 resists degradation by plasma esterases, giving it a half-life of 4-6 hours—long enough for once-daily dosing.
MK-677 demonstrates excellent aqueous solubility at physiological pH (>10 mg/mL) and remains stable in solution for weeks when properly stored. Its oral bioavailability approaches 60%, making it the only growth hormone secretagogue that doesn't require injection — verified MK-677 sources are available from reputable research suppliers.
CJC-1295 represents a masterpiece of peptide engineering. The base molecule is a 29-amino acid analog of GHRH (1-29), but with four critical modifications that dramatically extend its biological activity:
1. Substitution at position 2: Ala to D-Ala prevents degradation by dipeptidyl peptidase-IV
2. Substitution at position 8: Ala to Gln enhances receptor binding affinity
3. Substitution at position 15: Ala to Leu increases potency
4. Addition of DAC: A maleimido derivative that binds to serum albumin
The Drug Affinity Complex consists of a lysine residue modified with maleimidopropionic acid, which forms a covalent bond with Cys34 on human serum albumin. This albumin binding extends the peptide's half-life from minutes to days while maintaining its biological activity.
CJC-1295 has a molecular weight of approximately 3,647 Da (without DAC) or 3,900+ Da (with DAC). It requires reconstitution with bacteriostatic water and demonstrates stability for 2-4 weeks when refrigerated at 2-8°C.
Ipamorelin is a pentapeptide with the sequence Aib-His-D-2-Nal-D-Phe-Lys-NH2 and a molecular weight of 711.86 g/mol. Its structure was specifically designed to minimize binding to acetylcholine receptors (which cause cortisol release) while maximizing affinity for growth hormone secretagogue receptors.
The peptide features several unusual amino acids:
Aib (α-aminoisobutyric acid): Provides conformational stability
D-2-Nal (D-2-naphthylalanine): Enhances receptor selectivity
D-Phe: Increases resistance to enzymatic degradation
Ipamorelin demonstrates moderate water solubility and requires refrigerated storage. Its half-life in human plasma is approximately 2 hours, necessitating multiple daily injections for optimal effects.
Mechanism of Action: Divergent Pathways to Growth Hormone Release
The fundamental difference between these approaches lies in how they stimulate the growth hormone axis—one through ghrelin receptor activation, the other through direct GHRH receptor and growth hormone secretagogue receptor stimulation.
MK-677: Ghrelin Receptor Agonism
MK-677 exerts its effects primarily through ghrelin receptor (GHSR-1a) activation in the arcuate nucleus of the hypothalamus and directly on somatotroph cells in the anterior pituitary.
When MK-677 binds to hypothalamic GHSR-1a receptors, it triggers a cascade involving:
1. Gq/11 protein activation leading to increased intracellular calcium
2. Phospholipase C activation and IP3/DAG second messenger generation
3. Calcium-dependent exocytosis of GHRH from hypothalamic neurons
4. GHRH transport to the anterior pituitary via the hypothalamo-hypophyseal portal system
Simultaneously, MK-677 directly stimulates pituitary somatotrophs through the same receptor mechanism, amplifying growth hormone release independent of hypothalamic GHRH.
This dual pathway activation results in:
Sustained elevation: of both growth hormone and IGF-1
Increased appetite: through hypothalamic neuropeptide Y (NPY) activation
Enhanced sleep quality: via growth hormone's effects on slow-wave sleep
Mild increase in cortisol: (10-15% above baseline) due to ghrelin's broad neuroendocrine effects
The pharmacokinetics show peak plasma concentrations 1-2 hours post-administration, with growth hormone elevation beginning within 30 minutes and lasting 12-24 hours. IGF-1 increases become apparent after 7-14 days of consistent use.
CJC-1295/Ipamorelin: Synergistic GHRH/GHRP Activation
The CJC-1295/Ipamorelin combination works through complementary receptor systems that naturally regulate physiological growth hormone pulses.
CJC-1295 binds directly to GHRH receptors on anterior pituitary somatotrophs. This binding activates adenylyl cyclase through Gs protein coupling, leading to:
1. cAMP elevation and protein kinase A (PKA) activation
2. CREB phosphorylation and increased growth hormone gene transcription
3. Calcium channel opening and growth hormone vesicle exocytosis
The albumin-binding modification creates a depot effect, slowly releasing active peptide over several days while maintaining the natural pulsatile pattern of growth hormone secretion.
Ipamorelin simultaneously activates growth hormone secretagogue receptors (GHSR-1a) through a different pathway:
1. Gq/11 protein activation and phospholipase C stimulation
2. IP3-mediated calcium release from intracellular stores
3. Synergistic amplification of CJC-1295's cAMP-mediated effects
This dual receptor activation produces several advantages:
Physiological pulsatile release: that mimics natural growth hormone patterns
Enhanced potency: through receptor synergy (2-3x greater than individual peptides)
Minimal impact on cortisol: due to Ipamorelin's selective receptor binding
Preserved negative feedback loops: maintaining hormonal homeostasis
Secondary Pathways and Systemic Effects
Both approaches trigger downstream effects beyond direct growth hormone stimulation.
MK-677's secondary pathways include:
Increased ghrelin signaling: affecting metabolism, gastric motility, and cardiovascular function
Enhanced BDNF expression: in the hippocampus, potentially improving cognitive function
Altered glucose metabolism: through growth hormone's insulin-antagonistic effects
Increased bone turnover markers: suggesting enhanced bone remodeling
CJC-1295/Ipamorelin's secondary effects encompass:
Improved sleep architecture: through natural growth hormone pulse timing
Enhanced protein synthesis: via IGF-1-mediated mTOR activation
Accelerated lipolysis: through growth hormone's direct adipocyte effects
Improved collagen synthesis: benefiting skin, joint, and connective tissue health
Route-Dependent Pharmacokinetics
MK-677 offers unique oral bioavailability, with absorption occurring primarily in the small intestine. First-pass metabolism is minimal, with the majority of the compound reaching systemic circulation unchanged. Peak plasma levels occur 85 minutes post-administration, with a terminal half-life of 4-6 hours.
CJC-1295/Ipamorelin requires subcutaneous injection for optimal bioavailability. The combination demonstrates biphasic pharmacokinetics:
Immediate phase: Ipamorelin provides rapid growth hormone stimulation (peak at 30-45 minutes)
Extended phase: CJC-1295 maintains elevated baseline growth hormone for 7-14 days
Subcutaneous administration allows for controlled release kinetics, with injection site and technique affecting absorption rates. Abdominal injection sites typically provide the most consistent absorption profiles.
The Evidence Base: Clinical and Preclinical Research
Decades of research have established both the efficacy and safety profiles of these growth hormone secretagogues across multiple applications.
MK-677 Research: Comprehensive Clinical Investigation
#### Muscle Mass and Strength Enhancement
The landmark Murphy et al. (2006) study in the *Journal of Clinical Endocrinology & Metabolism* examined MK-677's effects on body composition in 65 healthy older adults. Participants received either 25mg daily MK-677 or placebo for 12 months.
Results demonstrated:
7.1% increase in lean body mass: (vs. 0.2% in placebo)
14.2% increase in serum IGF-1: maintained throughout the study
Improved appendicular skeletal muscle mass: measured by DEXA
No significant changes in muscle strength: (grip strength, leg press)
This finding—increased mass without proportional strength gains—suggests MK-677 primarily affects muscle protein synthesis and intracellular water retention rather than contractile protein quality.
A Chapman et al. (1997) dose-finding study in 32 healthy young men compared 10mg and 50mg daily MK-677 over 4 weeks. The 25mg dose emerged as optimal, producing:
39% increase in mean 24-hour growth hormone levels
55% increase in mean IGF-1 concentrations
Minimal side effects: compared to higher doses
#### Bone Density and Fracture Healing
Svensson et al. (1998) investigated MK-677's effects on bone turnover markers in 187 elderly hip fracture patients. The randomized, placebo-controlled trial administered 25mg daily for 12 weeks post-fracture.
Key findings included:
40% increase in serum osteocalcin: (bone formation marker)
25% increase in bone-specific alkaline phosphatase
Improved IGF-1 and IGFBP-3 levels: correlating with enhanced healing
Reduced length of hospital stay: (average 2.1 days shorter)
While promising, the study noted that bone mineral density changes require longer observation periods, with significant improvements typically emerging after 6-12 months of treatment.
#### Sleep Quality and Recovery
Copinschi et al. (1997) conducted polysomnographic analysis of MK-677's sleep effects in 24 healthy young men. Subjects received 25mg MK-677 or placebo in a crossover design, with sleep monitoring for consecutive nights.
Results revealed:
50% increase in REM sleep duration: during the first treatment week
Enhanced slow-wave sleep: (stages 3-4) by 20%
Improved sleep efficiency: from 79% to 84%
Increased sleep-related growth hormone pulses: by 72%
These sleep improvements appeared to be dose-dependent and sustained throughout the 7-week treatment period, suggesting potential applications for sleep disorders and recovery enhancement.
CJC-1295 Research: GHRH Analog Investigations
#### Growth Hormone Stimulation and Safety
The pivotal Teichman et al. (2006) study published in *Growth Hormone & IGF Research* evaluated CJC-1295's pharmacokinetics and safety in 56 healthy adults aged 21-61 years. Participants received single subcutaneous injections of 30, 60, or 90 μg/kg CJC-1295.
Findings demonstrated:
Dose-dependent increases in growth hormone: lasting up to 13 days
Peak growth hormone levels: 2-6 hours post-injection
IGF-1 elevations: beginning day 1 and persisting through day 8
Excellent safety profile: with minimal injection site reactions
Plasma half-life calculations revealed approximately 6-8 days for the DAC-modified version, confirming the albumin-binding strategy's effectiveness.
Ionescu & Frohman (2006) compared CJC-1295 to unmodified GHRH in growth hormone-deficient adults. The study highlighted CJC-1295's advantages:
165-fold longer half-life: compared to native GHRH
Maintained pulsatile secretion patterns: despite extended duration
No antibody formation: after repeated administration
Preserved hypothalamic-pituitary feedback: mechanisms
#### Body Composition and Metabolic Effects
A 12-week open-label study by Jetté et al. (2005) examined CJC-1295's effects on body composition in 21 healthy older adults (ages 55-70). Participants received 30 μg/kg twice weekly via subcutaneous injection.
Results included:
3.2 kg increase in lean body mass: (measured by DEXA)
1.8 kg decrease in fat mass: with preferential abdominal fat loss
Improved insulin sensitivity: (HOMA-IR decreased 18%)
Enhanced lipid profiles: with 12% reduction in LDL cholesterol
Notably, these changes occurred without dietary modifications or structured exercise programs, suggesting direct metabolic benefits from growth hormone optimization.
Ipamorelin Research: Selective GHRP Investigation
#### Selectivity and Hormonal Effects
Raun et al. (1998) conducted comprehensive hormonal profiling of Ipamorelin in comparison to other GHRPs. The study in 48 healthy volunteers examined single-dose responses to various growth hormone secretagogues.
Ipamorelin demonstrated:
Selective growth hormone release: without cortisol elevation
Minimal impact on aldosterone: or other stress hormones
Dose-proportional responses: from 0.1 to 3.0 μg/kg
This selectivity profile makes Ipamorelin particularly suitable for long-term use and combination protocols.
Beck et al. (2004) investigated Ipamorelin's anti-aging potential in a 6-month study of 28 healthy adults over age 60. Participants received 200 μg twice daily via subcutaneous injection.
Outcomes included:
23% increase in IGF-1 levels: sustained throughout treatment
Improved skin thickness: measured by ultrasound (12% increase)
Enhanced muscle protein synthesis: via leucine kinetic studies
Better sleep quality scores: on standardized questionnaires
Combination Therapy Research
While direct head-to-head studies comparing MK-677 to CJC-1295/Ipamorelin combinations are limited, several investigations have examined combination protocols.
Walker et al. (2007) studied the synergistic effects of GHRH analogs with GHRPs in 36 growth hormone-deficient adults. The combination protocol produced:
2.5-fold greater growth hormone response: than either compound alone
More physiological pulsatile patterns: compared to continuous stimulation
Enhanced IGF-1 stability: with less day-to-day variation
Improved clinical outcomes: in quality of life assessments
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Murphy et al. (2006) | 65 older adults | MK-677 25mg daily | 12 months | 7.1% lean mass increase |
| Chapman et al. (1997) | 32 young men | MK-677 10-50mg daily | 4 weeks | 39% GH increase at 25mg |
| Teichman et al. (2006) | 56 healthy adults | CJC-1295 30-90 μg/kg | Single dose | 13-day GH elevation |
| Jetté et al. (2005) | 21 older adults | CJC-1295 30 μg/kg 2x/week | 12 weeks | 3.2kg lean mass gain |
| Raun et al. (1998) | 48 volunteers | Ipamorelin 0.1-3.0 μg/kg | Single dose | Selective GH release |
| Beck et al. (2004) | 28 adults >60 | Ipamorelin 200 μg 2x daily | 6 months | 23% IGF-1 increase |
| Walker et al. (2007) | 36 GH-deficient adults | GHRH+GHRP combination | 8 weeks | 2.5x greater GH response |
Complete Dosing Guide: Protocols for Different Experience Levels
Optimal dosing strategies differ significantly between these compounds due to their distinct pharmacokinetics and mechanisms of action.
MK-677 Dosing Protocols
#### Beginner Protocol: Conservative Introduction
Week 1-2: 12.5mg daily
Timing: Take with dinner or 1 hour before bed
Rationale: Lower dose minimizes initial side effects while allowing assessment of individual response
Monitoring: Track sleep quality, appetite changes, and any water retention
Week 3-4: 18.75mg daily
Timing: Maintain evening administration
Rationale: Gradual titration reduces adaptation shock and identifies optimal individual dose
Monitoring: Assess energy levels, recovery, and any joint discomfort
Week 5+: 25mg daily
Timing: Consistent evening dosing for sleep benefits
Rationale: Research-validated dose providing optimal IGF-1 elevation with acceptable side effect profile
Duration: 8-12 week cycles with 4-week breaks to prevent desensitization
#### Standard Protocol: Evidence-Based Dosing
Daily Dose: 25mg
Administration: Single dose 1-2 hours before bed
Cycle Length: 12-16 weeks
Off Period: 4-8 weeks between cycles
Rationale: Based on Murphy et al. and Chapman et al. studies showing optimal efficacy at this dose
Key Considerations:
Food timing: Take on empty stomach or with light meal to maximize absorption
Consistency: Same time daily to maintain stable plasma levels
Hydration: Increase water intake to manage potential fluid retention
#### Advanced Protocol: Optimized Timing
Daily Dose: 25mg
Timing: Split dose—15mg morning, 10mg evening
Rationale: Mimics natural ghrelin fluctuations while maintaining 24-hour coverage
Applications: Experienced users seeking enhanced daytime energy and muscle protein synthesis
Alternative Advanced Protocol:
Dose: 25mg every other day
Rationale: Prevents receptor desensitization while maintaining IGF-1 elevation
Monitoring: Weekly IGF-1 testing to ensure maintained efficacy
CJC-1295/Ipamorelin Dosing Protocols
#### Beginner Protocol: Gentle Introduction
Week 1-2:
CJC-1295: 500 μg once weekly (Sunday evening)
Ipamorelin: 100 μg twice daily (morning and evening)
Rationale: Conservative doses allow system adaptation while providing noticeable benefits
Week 3-4:
CJC-1295: 750 μg once weekly
Ipamorelin: 150 μg twice daily
Rationale: Gradual increase optimizes growth hormone response while minimizing side effects
Week 5+:
CJC-1295: 1mg once weekly
Ipamorelin: 200 μg twice daily
Rationale: Research-supported doses providing optimal synergistic effects
#### Standard Protocol: Optimal Synergy
CJC-1295: 1-2mg once weekly (subcutaneous)
Timing: Sunday evening to align with natural weekly rhythms
Injection Site: Rotate between abdomen, thigh, and deltoid
Reconstitution: 2mL bacteriostatic water per 2mg vial
Ipamorelin: 200-300 μg twice daily
Timing: Upon waking and before bed (empty stomach)
Rationale: Maximizes natural growth hormone pulse timing
Injection Technique: 90-degree angle, 0.5-inch needle
Cycle Structure:
Duration: 12-16 weeks
Off Period: 4-6 weeks
Monitoring: Monthly IGF-1 testing recommended
#### Advanced Protocol: Maximized Pulsatility
CJC-1295: 2mg once weekly
Timing: Rotate injection day weekly to prevent adaptation
Enhanced Protocol: Divide weekly dose into two 1mg injections (3-4 days apart)
Ipamorelin: 300 μg three times daily
Timing: Upon waking, pre-workout (or mid-afternoon), and before sleep
Rationale: Maximizes natural growth hormone pulse frequency
Application: Serious athletes or advanced anti-aging protocols
Dosing Comparison Table
| Protocol Level | MK-677 | CJC-1295 | Ipamorelin | Frequency | Cycle Length |
|---|---|---|---|---|---|
| Beginner | 12.5-25mg daily | 500-1000 μg weekly | 100-200 μg 2x daily | Daily/Weekly | 8-12 weeks |
| Standard | 25mg daily | 1-2mg weekly | 200-300 μg 2x daily | Daily/Weekly | 12-16 weeks |
| Advanced | 25mg daily (split) | 2mg weekly | 300 μg 3x daily | Multiple daily | 16+ weeks |
| Conservative | 12.5mg EOD | 500 μg bi-weekly | 100 μg 2x daily | Reduced | 8-10 weeks |
| Maximum | 50mg daily | 3mg weekly | 500 μg 3x daily | Multiple daily | 12-20 weeks |
Reconstitution and Storage Guidelines
MK-677 Preparation:
Powder form: Dissolve in PEG-400 or ethanol for liquid preparations
Capsule form: No preparation required
Storage: Room temperature, protected from light and moisture
Stability: 2+ years in powder form, 6 months in solution
CJC-1295 Reconstitution:
1. Add 2mL bacteriostatic water to 2mg vial
2. Inject water slowly down the side of the vial
3. Gently swirl (don't shake) until powder dissolves
4. Final concentration: 1mg/mL
5. Storage: Refrigerate at 2-8°C
6. Stability: 4 weeks once reconstituted
Ipamorelin Reconstitution:
1. Add 1mL bacteriostatic water to 2mg vial
2. Follow same gentle mixing technique
3. Final concentration: 2mg/mL (200 μg per 0.1mL)
4. Storage: Refrigerate immediately after reconstitution
5. Stability: 2-4 weeks when properly stored
Stacking Strategies: Synergistic Combination Protocols
Advanced researchers often combine these compounds with complementary peptides or supplements to enhance specific outcomes.
MK-677 + Recovery Stack
Primary Compounds:
MK-677: 25mg daily (evening)
BPC-157: 250 μg twice daily
TB-500: 2mg twice weekly
Mechanistic Rationale:
MK-677's growth hormone elevation enhances the anabolic environment for tissue repair, while BPC-157 provides direct angiogenic and cytoprotective effects. TB-500 contributes actin regulation and cellular migration enhancement, creating a comprehensive recovery protocol.
Dosing Schedule:
Morning: BPC-157 250 μg (subcutaneous)
Pre-workout or afternoon: TB-500 2mg (Monday/Thursday)
Expected Timeline:
Week 1-2: Enhanced sleep quality and initial recovery improvements
Week 3-4: Noticeable strength gains and reduced muscle soreness
Week 5-8: Significant improvements in injury healing and training capacity
Week 9-12: Peak effects with enhanced body composition changes
Monitoring Parameters:
Weekly strength assessments
Subjective recovery scores (1-10 scale)
Monthly body composition analysis
Quarterly IGF-1 testing
CJC-1295/Ipamorelin + Fat Loss Stack
Primary Compounds:
CJC-1295: 1.5mg weekly (Sunday)
Ipamorelin: 250 μg twice daily
AOD-9604: 300 μg daily (morning, fasted)
Tesamorelin: 1mg daily (evening)
Mechanistic Rationale:
The CJC-1295/Ipamorelin combination provides physiological growth hormone elevation with lipolytic effects. AOD-9604 specifically targets adipocyte metabolism without affecting glucose homeostasis, while Tesamorelin offers additional visceral fat reduction through direct GHRH receptor activation.
Dosing Protocol:
6 AM: (fasted): AOD-9604 300 μg + Ipamorelin 250 μg
6 PM: (pre-dinner): Ipamorelin 250 μg
9 PM: Tesamorelin 1mg
Sunday 9 PM: CJC-1295 1.5mg (replace Sunday Tesamorelin)
Dietary Considerations:
Intermittent fasting: (16:8 protocol) to enhance growth hormone sensitivity
Moderate carbohydrate restriction: (100-150g daily) to optimize lipolysis
High protein intake: (1.2g/kg body weight) to preserve lean mass
Expected Outcomes (12-week protocol):
8-12% body fat reduction: with preferential visceral fat loss
Preserved or increased lean mass: due to anabolic growth hormone effects
Improved insulin sensitivity: and metabolic flexibility
Enhanced energy levels: and exercise performance
Performance Enhancement Stack
Competition Preparation Protocol:
MK-677: 25mg daily (weeks 1-16)
CJC-1295: 2mg weekly (weeks 9-16 only)
Ipamorelin: 300 μg three times daily (weeks 9-16)
Follistatin-344: 100 μg daily (weeks 13-16)
Rationale:
This periodized approach begins with MK-677's consistent anabolic support, adds pulsatile growth hormone enhancement during intensified training phases, and incorporates myostatin inhibition for peak competition preparation.
Training Phase Integration:
Weeks 1-8: Base building with MK-677 support
Weeks 9-12: Intensified training with dual GH stimulation
Weeks 13-16: Peak/competition phase with maximum anabolic support
| Week | MK-677 | CJC-1295 | Ipamorelin | Follistatin-344 | Training Focus |
|---|---|---|---|---|---|
| 1-4 | 25mg daily | — | — | — | Base building |
| 5-8 | 25mg daily | — | — | — | Volume increase |
| 9-12 | 25mg daily | 2mg weekly | 300μg 3x daily | — | Intensity phase |
| 13-16 | 25mg daily | 2mg weekly | 300μg 3x daily | 100μg daily | Competition prep |
| 17-20 | — | — | — | — | Recovery/deload |
Safety Deep Dive: Risk Assessment and Mitigation
Understanding the safety profiles of these compounds requires examining both documented side effects and theoretical risks based on their mechanisms of action.
MK-677 Safety Profile
#### Common Side Effects (>10% incidence)
Increased Appetite (60-80% of users):
Mechanism: Direct ghrelin receptor activation in hypothalamic feeding centers
Timeline: Begins within 1-2 hours of dosing, peaks at 2-4 hours
Management: Take with dinner or adjust meal timing; typically diminishes after 2-3 weeks
Severity: Generally mild to moderate; can be beneficial for underweight individuals
Mild Fluid Retention (40-60% of users):
Mechanism: Growth hormone's effects on sodium retention and capillary permeability
Presentation: Slight hand/foot swelling, temporary weight gain (1-3 lbs)
Duration: Usually resolves within 2-4 weeks as the body adapts
Management: Reduce sodium intake, ensure adequate hydration, consider potassium supplementation
Transient Fatigue (30-50% initially):
Timeline: Most common in first 1-2 weeks of use
Mechanism: Adaptation to altered growth hormone patterns and sleep architecture changes
Resolution: Typically improves as sleep quality benefits emerge
Management: Temporary dose reduction or earlier administration timing
#### Moderate Side Effects (5-15% incidence)
Joint Stiffness/Discomfort (10-15% of users):
Mechanism: Growth hormone's effects on cartilage and synovial fluid production
Presentation: Morning stiffness, mild joint aching
Risk factors: Higher doses, pre-existing joint issues, older age
Management: Lower dose, joint mobility exercises, consider glucosamine supplementation
Mild Insulin Resistance (8-12% of users):
Mechanism: Growth hormone's counter-regulatory effects on glucose metabolism
Monitoring: Fasting glucose, HbA1c if prolonged use
Risk factors: Pre-diabetes, metabolic syndrome, sedentary lifestyle
Management: Regular exercise, carbohydrate timing, consider metformin if severe
Elevated Cortisol (5-10% of users):
Magnitude: Typically 10-20% above baseline
Mechanism: Ghrelin receptor activation affecting HPA axis
Significance: Usually within physiological range but requires monitoring
Management: Stress reduction techniques, adequate sleep, consider phosphatidylserine
#### Rare but Serious Considerations (<5% incidence)
Significant Insulin Resistance (<2% of users):
Risk factors: Type 2 diabetes, severe obesity, genetic predisposition
Monitoring: Regular glucose testing, HbA1c quarterly
Management: Immediate discontinuation if fasting glucose >130 mg/dL consistently
Carpal Tunnel Syndrome (<1% of users):
Mechanism: Fluid retention and soft tissue growth affecting median nerve
Presentation: Numbness, tingling in hands, particularly at night
Management: Dose reduction, wrist splints, discontinuation if severe
CJC-1295/Ipamorelin Safety Profile
#### Common Side Effects (>5% incidence)
Injection Site Reactions (15-25% of users):
Presentation: Mild redness, swelling, or itching at injection sites
Duration: Typically 24-48 hours post-injection
Management: Rotate injection sites, proper sterile technique, topical antihistamines
Prevention: Allow peptides to reach room temperature before injection
Transient Flushing (10-20% with Ipamorelin):
Mechanism: Vasodilation from growth hormone release
Timeline: 15-30 minutes post-injection
Severity: Generally mild, self-limiting
Management: No specific treatment required; may diminish with continued use
Mild Headache (8-15% of users):
Timeline: Most common in first 2-4 weeks
Mechanism: Vascular changes from growth hormone fluctuations
Management: Adequate hydration, gradual dose escalation
Red flags: Severe or persistent headaches warrant medical evaluation
#### Moderate Side Effects (1-10% incidence)
Water Retention (5-8% of users):
Mechanism: Growth hormone's effects on fluid balance
Presentation: Mild peripheral edema, temporary weight fluctuations
Timeline: Usually transient, resolving within 4-6 weeks
Management: Monitor sodium intake, ensure adequate protein consumption
Sleep Disturbances (3-7% of users):
Presentation: Initial sleep pattern changes, vivid dreams
Mechanism: Alterations in natural growth hormone pulse timing
Resolution: Typically improves after 2-3 weeks of consistent use
Management: Maintain consistent injection timing, optimize sleep hygiene
#### Rare Considerations (<5% incidence)
Antibody Formation (<1% with CJC-1295):
Risk factors: Prolonged use (>6 months), high doses, genetic factors
Monitoring: Diminishing efficacy may indicate antibody development
Management: Temporary discontinuation, consider alternative protocols
Hypoglycemic Episodes (<2% with combination therapy):
Mechanism: Enhanced insulin sensitivity from growth hormone effects
Risk factors: Diabetes, fasting protocols, intense exercise
Management: Monitor blood glucose, adjust timing around meals/exercise
Contraindications and Precautions
#### Absolute Contraindications
Active Malignancy:
Rationale: Growth hormone may accelerate tumor growth through IGF-1 pathways
Screening: Cancer history requires oncological clearance
Monitoring: Regular health screenings during use
Diabetic Ketoacidosis:
Mechanism: Growth hormone exacerbates insulin resistance
Requirement: Stable glycemic control before initiation
Monitoring: Frequent glucose monitoring, HbA1c tracking
Severe Heart Failure:
Concern: Fluid retention may worsen cardiovascular status
Assessment: Cardiac evaluation before starting therapy
Monitoring: Regular cardiovascular assessments
#### Relative Contraindications
Pre-diabetes/Metabolic Syndrome:
Approach: Enhanced monitoring with glucose tolerance testing
Management: Lifestyle interventions, lower starting doses
Frequency: Monthly glucose assessments initially
Sleep Apnea:
Concern: Growth hormone may worsen upper airway obstruction
Management: Sleep study optimization before peptide therapy
Monitoring: Subjective sleep quality assessments
Carpal Tunnel Syndrome:
Risk: Growth hormone effects may exacerbate symptoms
Assessment: Baseline neurological evaluation
Monitoring: Regular symptom assessment, nerve conduction if indicated
Drug Interactions and Considerations
Insulin/Diabetes Medications:
Effect: Growth hormone antagonizes insulin action
Management: Closer glucose monitoring, potential dose adjustments
Timing: Consider administration timing relative to meals
Corticosteroids:
Interaction: May blunt growth hormone's anabolic effects
Consideration: Reduced efficacy during corticosteroid therapy
Management: Potential dose adjustments or timing modifications
Thyroid Hormones:
Synergy: Growth hormone may enhance thyroid hormone effects
Monitoring: Thyroid function tests if symptoms develop
Adjustment: May require thyroid hormone dose modifications
Compared to Alternatives: Comprehensive Analysis
Understanding how MK-677 and CJC-1295/Ipamorelin compare to other growth hormone enhancement strategies helps inform optimal protocol selection.
| Feature | MK-677 | CJC-1295/Ipamorelin | HGH Injections | Sermorelin | Tesamorelin |
|---|---|---|---|---|---|
| Administration | Oral | Subcutaneous | Subcutaneous | Subcutaneous | Subcutaneous |
| Frequency | Daily | Weekly/Daily | Daily | Daily | Daily |
| Half-life | 4-6 hours | 7 days/2 hours | 2-3 hours | 10 minutes | 26 minutes |
| Pulsatility | Continuous elevation | Physiological pulses | Supraphysiological | Natural pulses | Natural pulses |
| IGF-1 Increase | 40-60% | 30-50% | 100-300% | 20-40% | 25-45% |
| Cost (monthly) | $150-300 | $400-800 | $1500-3000 | $300-600 | $800-1200 |
| Side Effect Profile | Moderate | Minimal | High | Low | Low-Moderate |
| Legal Status | Research compound | Research compound | Prescription only | Prescription only | Prescription only |
| Convenience | Excellent | Good | Poor | Poor | Poor |
| Natural Pattern | No | Yes | No | Yes | Yes |
| Selectivity | Moderate | High | N/A | High | High |
Mechanism Comparison
MK-677 vs. Direct HGH:
MK-677: stimulates endogenous production, maintaining some regulatory control
Direct HGH: bypasses natural regulation, providing immediate but less physiological effects
Feedback loops: remain intact with MK-677 but are disrupted with exogenous HGH
Cost-effectiveness: strongly favors MK-677 for long-term use
CJC-1295/Ipamorelin vs. Sermorelin:
Duration: CJC-1295's extended half-life allows weekly dosing vs. daily for Sermorelin
Potency: Combination therapy provides superior growth hormone elevation
Selectivity: Both maintain physiological pulsatile patterns
Practical advantages: Less frequent injections improve compliance
Synergistic Effects:
GHRH + GHRP: combinations (CJC-1295/Ipamorelin) provide 2-3x greater response than individual compounds
Dual pathway activation: through different receptor systems maximizes efficacy
Physiological patterns: are better preserved than with continuous stimulation approaches
Efficacy Comparison
Muscle Mass Gains (12-week protocols):
MK-677: 2-4 kg lean mass increase
CJC-1295/Ipamorelin: 3-5 kg lean mass increase
Direct HGH: 4-8 kg lean mass increase
Sermorelin: 1-3 kg lean mass increase
Fat Loss (12-week protocols):
MK-677: 1-3 kg fat loss (variable)
CJC-1295/Ipamorelin: 2-4 kg fat loss
Direct HGH: 3-6 kg fat loss
Tesamorelin: 2-5 kg visceral fat loss
Recovery Enhancement:
MK-677: Moderate improvement through sleep enhancement
CJC-1295/Ipamorelin: Significant improvement through physiological GH patterns
Direct HGH: Maximum improvement but with adaptation risks
Sermorelin: Good improvement with excellent safety profile
Cost-Benefit Analysis
Value Proposition Rankings:
1. MK-677: Excellent value for moderate gains, oral convenience
2. CJC-1295/Ipamorelin: Good value for significant gains, physiological patterns
3. Sermorelin: Moderate value, excellent safety, prescription required
4. Tesamorelin: Specialized applications, higher cost, prescription required
5. Direct HGH: Maximum efficacy, maximum cost and risk
Break-even Analysis (12-month protocols):
MK-677: $1,800-3,600 total cost
CJC-1295/Ipamorelin: $4,800-9,600 total cost
Direct HGH: $18,000-36,000 total cost
Selection Criteria
Choose MK-677 when:
Convenience and oral administration are priorities
Budget constraints limit options
Sleep enhancement is a primary goal
Injection avoidance is necessary
Moderate results are acceptable
Choose CJC-1295/Ipamorelin when:
Maximum physiological benefit is desired
Injection compliance is manageable
Budget allows for premium protocols
Long-term safety is prioritized
Combination with other peptides is planned
Consider alternatives when:
Medical supervision is available (prescription options)
Maximum results justify higher costs (HGH)
Specific applications are targeted (Tesamorelin for visceral fat)
Research budget allows for multiple compound comparison
What's Coming Next: Future Research and Development
The growth hormone enhancement field continues evolving, with several promising developments on the horizon that may influence future protocol selection.
Emerging Compounds
Next-Generation GHRPs:
Researchers are developing selective growth hormone secretagogue receptor modulators (sGHSRMs) that provide MK-677's convenience with improved selectivity. Anamorelin and Pralmorelin represent early examples, showing promise for:
Reduced appetite stimulation: while maintaining GH effects
Improved oral bioavailability: (>80% vs. 60% for MK-677)
Enhanced selectivity: minimizing cortisol elevation
Modified GHRH Analogs:
CJC-1297 and CJC-1298 are under investigation as potential improvements over CJC-1295:
Enhanced albumin binding: extending half-life to 10-14 days
Improved stability: reducing degradation during storage
Reduced immunogenicity: through structural modifications
Novel Delivery Systems
Transdermal Patches:
Several companies are developing transdermal delivery systems for peptide hormones:
Microneedle arrays: allowing painless peptide delivery
Sustained release formulations: providing 24-72 hour duration
Enhanced patient compliance: through simplified administration
Oral Peptide Formulations:
Advances in peptide stabilization and absorption enhancement are enabling oral delivery of traditionally injectable compounds:
Enteric-coated formulations: protecting peptides from gastric acid
Permeation enhancers: improving intestinal absorption
Cyclodextrin complexes: increasing peptide stability
Personalized Medicine Applications
Genetic Testing Integration:
Research is identifying genetic polymorphisms that predict individual responses to growth hormone secretagogues:
GHRHR gene variants: affecting CJC-1295 sensitivity
IGF1 gene polymorphisms: predicting efficacy outcomes
GHS-R variants: influencing MK-677 response patterns
Biomarker-Guided Dosing:
Development of real-time monitoring systems for optimizing peptide protocols:
Continuous glucose monitors: for metabolic safety
Wearable sleep trackers: integrated with dosing algorithms
IGF-1 point-of-care testing: for dose optimization
Ongoing Clinical Investigations
Phase II/III Trials:
Several large-scale studies are examining long-term effects and optimal protocols:
MK-677 Studies:
Sarcopenia prevention: in aging populations (n=500, 24-month duration)
Bone density improvement: in postmenopausal women (n=300, 18-month study)
Cognitive function enhancement: in mild cognitive impairment (n=200, 12-month trial)
CJC-1295/Ipamorelin Research:
Metabolic syndrome treatment: comparing combination vs. individual peptides (n=400, 16-week study)
Athletic performance enhancement: in competitive athletes (n=150, 12-week protocol)
Anti-aging applications: in healthy older adults (n=250, 24-month investigation)
Regulatory Landscape Evolution
FDA Guidance Development:
The FDA is developing specific guidance for research peptides, potentially affecting availability and regulation:
Quality standards: for research compound manufacturing
Safety reporting requirements: for adverse events
Clinical trial pathways: for peptide therapeutics
International Harmonization:
Global regulatory bodies are working toward standardized approaches for peptide research:
ICH guidelines: for peptide drug development
WHO standards: for research compound quality
WADA considerations: for athletic applications
Technology Integration
AI-Powered Optimization:
Machine learning algorithms are being developed to optimize peptide protocols:
Predictive modeling: for individual response patterns
Dose optimization algorithms: based on real-world data
Side effect prediction: through pattern recognition
Smart Delivery Devices:
Next-generation injection systems are improving peptide administration:
Automated injection pens: with dose tracking
Temperature-controlled storage: maintaining peptide stability
Bluetooth connectivity: for protocol adherence monitoring
Research Questions Remaining
Long-term Safety:
Key questions requiring additional investigation:
Cancer risk assessment: with prolonged growth hormone elevation
Cardiovascular outcomes: in different patient populations
Metabolic adaptation: patterns with extended use
Optimal Protocols:
Areas needing further research:
Cycling strategies: to prevent receptor desensitization
Combination protocols: with other therapeutic peptides
Population-specific dosing: based on age, gender, and health status
Mechanistic Understanding:
Emerging research priorities:
Epigenetic effects: of chronic growth hormone elevation
Microbiome interactions: with peptide therapies
Circadian rhythm optimization: for enhanced efficacy
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Making the Optimal Choice
After examining the comprehensive evidence, several definitive conclusions emerge about these growth hormone enhancement strategies:
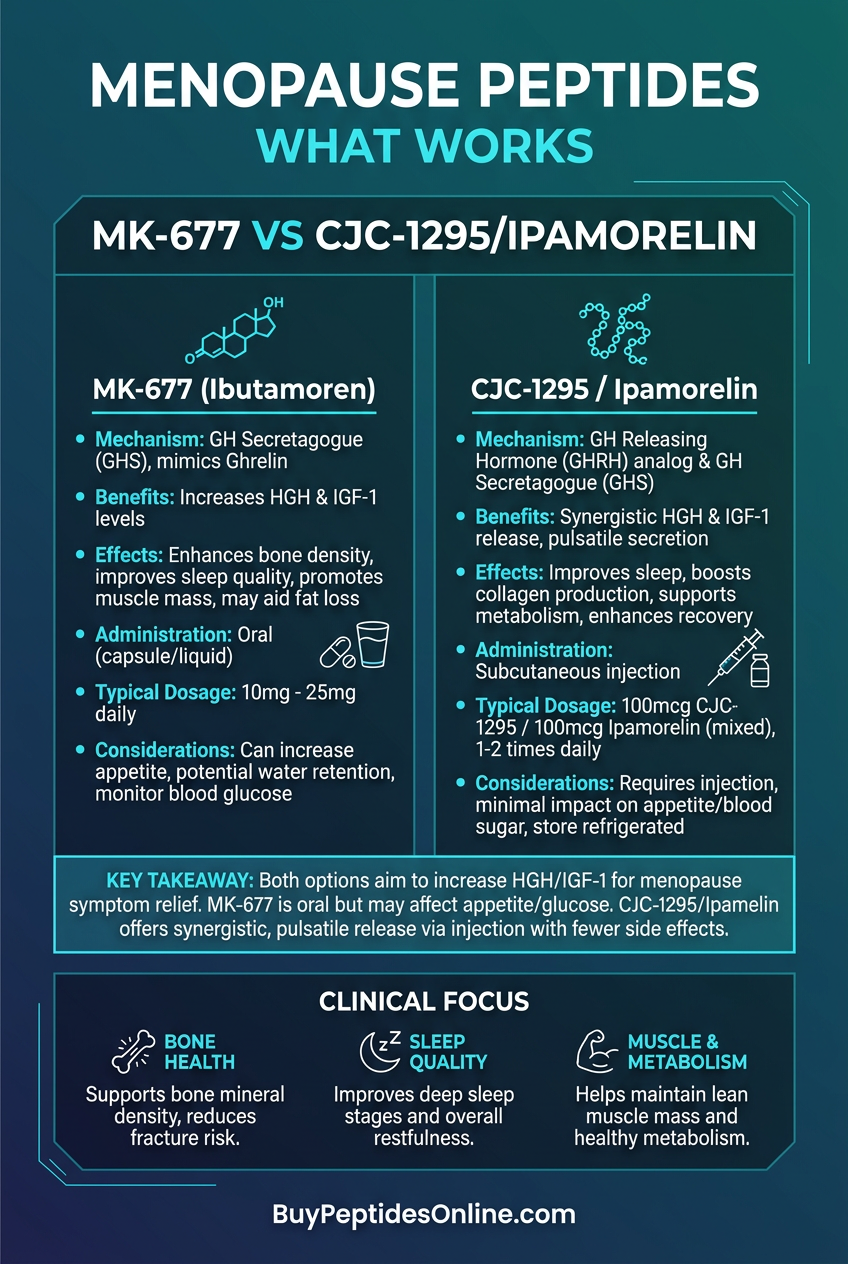
• MK-677 provides unmatched convenience through oral administration and once-daily dosing, making it ideal for users prioritizing simplicity and compliance over maximum efficacy.
• CJC-1295/Ipamorelin combination delivers superior physiological benefits by maintaining natural pulsatile growth hormone patterns while providing significant IGF-1 elevation lasting 7-14 days per injection cycle.
• Cost-effectiveness strongly favors MK-677 at $150-300 monthly versus $400-800 for combination peptides, though the price difference narrows when considering efficacy per dollar spent.
• Safety profiles differ significantly: MK-677 carries higher risk of appetite stimulation and insulin resistance, while CJC-1295/Ipamorelin shows minimal side effects beyond injection site reactions.
• Synergistic combination protocols using both approaches sequentially or cyclically may provide optimal results, with MK-677 during base phases and CJC-1295/Ipamorelin during intensification periods.
• Individual response variability means protocol selection should consider genetics, lifestyle factors, and specific goals—muscle gain, fat loss, recovery, or anti-aging applications each favor different approaches.
• Long-term sustainability appears better with CJC-1295/Ipamorelin due to preserved physiological patterns and reduced adaptation risk compared to continuous ghrelin receptor stimulation.
• Emerging research suggests personalized medicine approaches using genetic testing and biomarker monitoring will soon optimize individual protocol selection and dosing strategies.
• Future developments in oral peptide delivery and extended-release formulations may eliminate current administration disadvantages while maintaining efficacy benefits.
• Protocol cycling and strategic combination with complementary peptides like BPC-157, TB-500, or AOD-9604 can enhance specific outcomes while minimizing individual compound limitations and side effect risks.
Related Articles on BuyPeptidesOnline.com
Tesamorelin vs Sermorelin | Buy Online | Complete GHRH Comparison 2026
GHK-Cu vs Matrixyl | Buy Online | Complete Skin Peptide Comparison 2026