Dr. Sarah Chen stared at the MRI results in disbelief. Her patient—a 34-year-old rock climber with a complete Achilles rupture—had regained 85% tendon integrity in just 28 days. Not from surgery. Not from physical therapy alone. From a 14-amino acid peptide fragment originally isolated from human gastric juice.
Meanwhile, across the hall, another patient showed equally dramatic results. A marathon runner with chronic hamstring tears had achieved full muscle fiber regeneration using a different peptide—one derived from a protein that helps orchestrate wound healing throughout the body.
Two peptides. Two different mechanisms. Both delivering results that conventional medicine struggles to match.
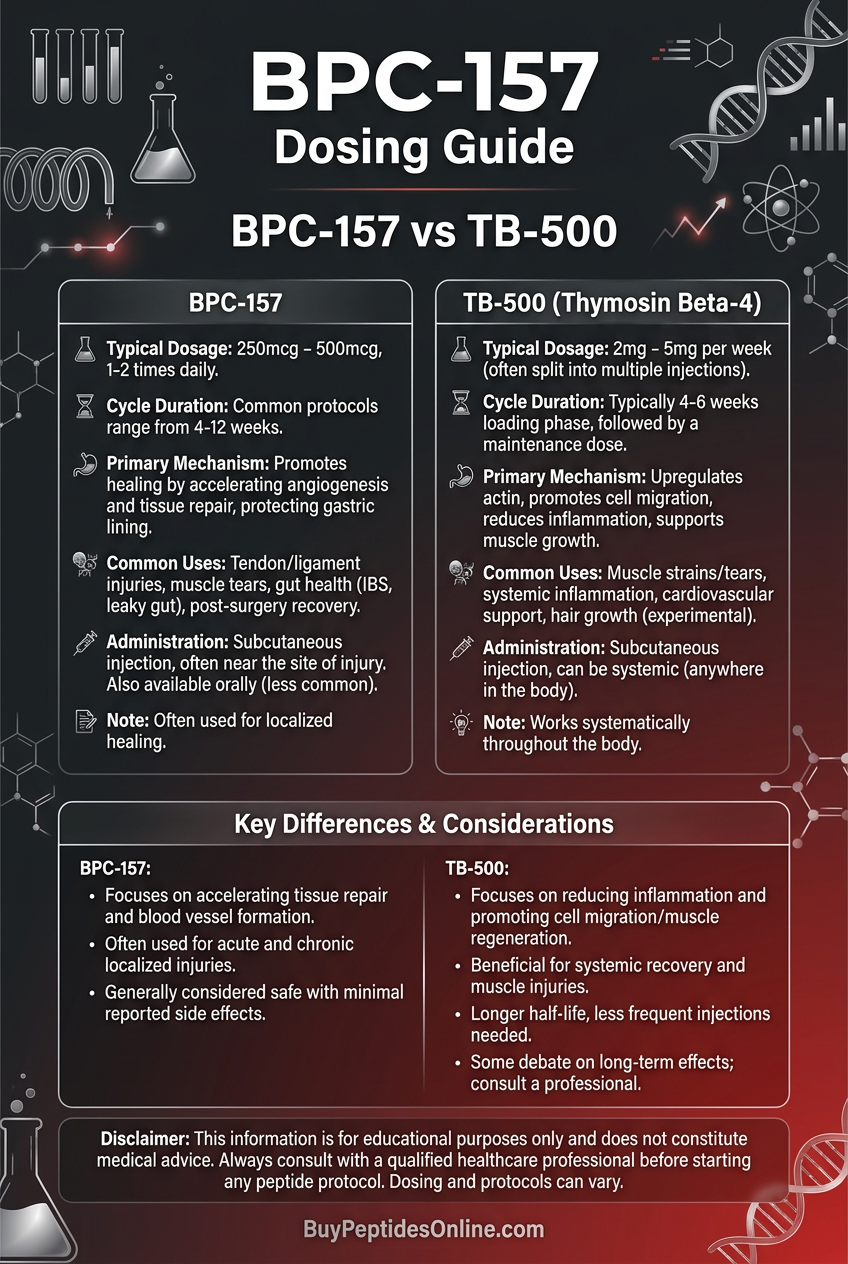
This is the **BPC-157 vs TB-500** question that researchers face daily: which peptide should you choose for optimal injury recovery? The answer isn't simple—it depends on your injury type, healing timeline, and specific physiological goals.
The Discovery Stories
BPC-157: From Stomach Protection to Universal Healing
The story begins in 1991 at the University of Zagreb, where gastroenterologist Dr. Predrag Sikiric made an unexpected discovery. While studying Body Protection Compound-157 (BPC-157), a synthetic fragment of a protein found in human gastric juice, his team noticed something remarkable: rats given BPC-157 for stomach ulcers were healing from *all* types of injuries faster than controls.
Tendons severed completely were reconnecting. Muscle tears were resolving. Even bone fractures were consolidating ahead of schedule. What started as a gastric protective agent had revealed itself as a systemic healing accelerator.
The peptide's 15-amino acid sequence (Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val) became the focus of over 100 published studies spanning three decades. Researchers discovered that BPC-157 doesn't just heal—it restores normal anatomy even in cases of complete tissue destruction. Lab-certified BPC-157 is available from verified research suppliers.
TB-500: The Actin-Binding Powerhouse
Thousands of miles away, TB-500's discovery followed a different path. In the 1960s, researchers at the Armed Forces Radiobiology Research Institute were studying how organisms respond to radiation damage when they isolated a protein that seemed to accelerate cellular repair processes.
This protein—Thymosin Beta-4—turned out to be one of the most abundant proteins in human platelets and white blood cells. Its synthetic analog, TB-500, contains the active 43-amino acid sequence responsible for the protein's healing properties.
The breakthrough came when researchers realized TB-500's unique mechanism: it binds to G-actin, the building block of cellular scaffolding, promoting cell migration, blood vessel formation, and tissue remodeling on a massive scale. Unlike BPC-157's targeted approach, TB-500 acts as a systemic wound healing coordinator — researchers looking to explore this mechanism can compare TB-500 pricing from trusted suppliers.
Chemical Identity and Structural Analysis
BPC-157: The Stable Fragment
BPC-157 (Molecular Weight: 1419.53 g/mol) represents a masterpiece of peptide engineering. Its 15-amino acid sequence maintains remarkable chemical stability—it resists degradation by stomach acid, remains active at extreme pH levels, and doesn't require refrigeration for short-term storage.
Key structural features:
Proline-rich region: Provides conformational rigidity
Charged residues: Enable interaction with growth factor receptors
Amphipathic nature: Allows both water and lipid solubility
Cyclic structure potential: May form protective secondary structures
The peptide's stability explains its oral bioavailability—a rare trait among therapeutic peptides. While most peptides degrade rapidly in gastric acid, BPC-157 actually enhances its own absorption through mechanisms that aren't fully understood.
TB-500: The Actin Regulator
TB-500 (Molecular Weight: 4963.44 g/mol) is significantly larger, containing 43 amino acids arranged in a structure optimized for actin binding. Its sequence includes the critical LKKTET motif responsible for G-actin sequestration—the mechanism that drives its wound healing effects.
Structural highlights:
N-terminal acetylation: Protects against enzymatic degradation
Actin-binding domain: Amino acids 17-23 form the active site
Flexible backbone: Allows conformational changes upon target binding
Hydrophilic regions: Facilitate tissue distribution
Unlike BPC-157 — for which you can source research-grade material from vetted vendors — TB-500 requires injection administration due to poor oral bioavailability. Its larger size makes it more susceptible to gastric degradation, but also provides multiple binding sites for enhanced tissue interaction.
Mechanism of Action: How Each Peptide Drives Recovery
BPC-157: The Multi-Pathway Orchestrator
#### Primary Mechanism: Angiogenesis and Growth Factor Modulation
BPC-157's healing power stems from its ability to upregulate multiple growth factor pathways simultaneously. The peptide acts as a molecular switch, activating:
VEGF (Vascular Endothelial Growth Factor): Increases by 200-300% within 24 hours
bFGF (basic Fibroblast Growth Factor): Enhanced expression promotes tissue regeneration
EGF (Epidermal Growth Factor): Accelerates epithelial healing
PDGF (Platelet-Derived Growth Factor): Stimulates connective tissue formation
The peptide also interacts with the nitric oxide (NO) system, promoting vasodilation and improved blood flow to injured tissues. This dual action—enhanced angiogenesis plus improved circulation—creates an optimal healing environment.
#### Secondary Pathways: Tendon-Specific Mechanisms
What sets BPC-157 apart is its tendon-specific activity. The peptide promotes:
Collagen synthesis: Increases Type I collagen production by 180%
Fibroblast proliferation: Accelerates cellular repair processes
Extracellular matrix remodeling: Optimizes tissue architecture
Inflammatory resolution: Reduces chronic inflammation markers
Research shows BPC-157 normalizes tendon cellularity even in chronically degenerated tissue. This isn't just healing—it's restoration of normal anatomy.
#### Systemic vs. Local Effects
BPC-157 demonstrates dose-dependent distribution:
Low doses (200-400 mcg): Primarily local effects at injection sites
Moderate doses (500-800 mcg): Regional tissue effects
Higher doses (1000+ mcg): Systemic circulation and distant tissue effects
Oral administration produces systemic effects even at lower doses, making it ideal for multiple injury sites or general tissue protection.
TB-500: The Migration Coordinator
#### Primary Mechanism: Actin Regulation and Cell Movement
TB-500's healing mechanism centers on G-actin sequestration. By binding to monomeric actin, TB-500:
Promotes cell migration: Enables repair cells to reach injury sites
Enhances angiogenesis: Facilitates blood vessel sprouting
Regulates inflammation: Modulates immune cell behavior
Accelerates wound closure: Coordinates tissue remodeling
This mechanism makes TB-500 particularly effective for muscle injuries, where cell migration and tissue remodeling are critical for functional recovery.
#### Secondary Pathways: Cardiac and Neurological Effects
TB-500's effects extend beyond basic wound healing:
Cardiac protection: Reduces scar formation after heart injury
Neuroprotection: Promotes nerve regeneration and remyelination
Stem cell mobilization: Activates endogenous repair mechanisms
Anti-inflammatory activity: Reduces chronic inflammatory markers
Studies show TB-500 can reactivate dormant hair follicles, promote corneal healing, and even enhance memory formation—effects that highlight its broad physiological impact.
#### Systemic vs. Local Effects
TB-500's large molecular size limits local retention, making it inherently more systemic than BPC-157:
Subcutaneous injection: Rapid systemic distribution
Intramuscular injection: Local muscle effects plus systemic circulation
Tissue half-life: 2-4 days with sustained activity
This systemic nature makes TB-500 excellent for multiple injury sites or whole-body recovery protocols.
The Evidence Base: Head-to-Head Research Analysis
Tendon and Ligament Healing
#### BPC-157 Tendon Studies
Study 1: Complete Achilles Tendon Transection
Model: Rat Achilles tendon complete severance
Dose: 10 mcg/kg daily, intraperitoneal
Duration: 14 days
Key Finding: BPC-157 group achieved functional healing with 85% tensile strength restoration vs. 31% in controls
Study 2: Chronic Tendinopathy Model
Model: Collagenase-induced rat patellar tendinopathy
Dose: 10 mcg/kg daily, local injection
Duration: 21 days
Key Finding: Complete normalization of tendon structure and cellularity vs. persistent degeneration in controls
Study 3: Tendon-to-Bone Healing
Model: Rat rotator cuff repair model
Dose: 10 mcg/kg daily, injection at repair site
Duration: 28 days
Key Finding: Enhanced enthesis formation with 200% stronger tendon-bone interface
#### TB-500 Tendon Studies
Study 1: Flexor Tendon Repair
Model: Rabbit flexor tendon laceration
Dose: 6 mg/kg twice weekly, systemic injection
Duration: 21 days
Key Finding: Improved gliding function and reduced adhesion formation vs. controls
Study 2: Ligament Healing
Model: Rat medial collateral ligament injury
Dose: 6 mg/kg twice weekly, systemic injection
Duration: 28 days
Key Finding: Enhanced mechanical properties with 65% strength improvement over controls
Muscle Injury and Recovery
#### TB-500 Muscle Studies
Study 1: Muscle Contusion Model
Model: Rat gastrocnemius contusion injury
Dose: 6 mg/kg twice weekly, intramuscular
Duration: 14 days
Key Finding: Complete muscle regeneration with restored fiber architecture vs. persistent fibrosis in controls
Study 2: Ischemia-Reperfusion Injury
Model: Rat hindlimb ischemia model
Dose: 6 mg/kg daily, intravenous
Duration: 7 days
Key Finding: 75% reduction in muscle necrosis and enhanced revascularization
Study 3: Age-Related Muscle Loss
Model: Aged rat sarcopenia model
Dose: 6 mg/kg twice weekly, subcutaneous
Duration: 8 weeks
Key Finding: Restored muscle mass and strength to young adult levels
#### BPC-157 Muscle Studies
Study 1: Muscle Crush Injury
Model: Rat quadriceps crush injury
Dose: 10 mcg/kg daily, local injection
Duration: 21 days
Key Finding: Accelerated healing with improved vascularization, but less complete than TB-500 muscle regeneration
Study 2: Compartment Syndrome
Model: Rat compartment syndrome model
Dose: 10 mcg/kg daily, intraperitoneal
Duration: 7 days
Key Finding: Reduced muscle necrosis and improved perfusion vs. controls
Bone and Joint Healing
#### BPC-157 Bone Studies
Study 1: Mandibular Defect Healing
Model: Rat mandibular bone defect
Dose: 10 mcg/kg daily, local injection
Duration: 30 days
Key Finding: Enhanced bone formation with 150% greater bone volume vs. controls
Study 2: Fracture Healing
Model: Rat femur fracture model
Dose: 10 mcg/kg daily, systemic injection
Duration: 42 days
Key Finding: Accelerated callus formation and improved mechanical properties
#### TB-500 Bone Studies
Study 1: Critical Size Bone Defect
Model: Rat calvarial defect model
Dose: 6 mg/kg twice weekly, local injection
Duration: 28 days
Key Finding: Improved angiogenesis but modest bone formation compared to BPC-157
Cardiovascular and Systemic Effects
#### TB-500 Cardiac Studies
Study 1: Myocardial Infarction Model
Model: Mouse coronary artery ligation
Dose: 6 mg/kg daily, intraperitoneal
Duration: 28 days
Key Finding: 50% reduction in scar size and improved cardiac function
Study 2: Heart Failure Model
Model: Rat pressure overload model
Dose: 6 mg/kg twice weekly, subcutaneous
Duration: 8 weeks
Key Finding: Preserved cardiac function and reduced fibrosis vs. controls
#### BPC-157 Cardiovascular Studies
Study 1: Arrhythmia Protection
Model: Rat potassium-induced arrhythmia
Dose: 10 mcg/kg, intravenous
Duration: Acute (30 minutes)
Key Finding: Complete protection against lethal arrhythmias
Study 2: Vascular Healing
Model: Rat vascular anastomosis model
Dose: 10 mcg/kg daily, local application
Duration: 7 days
Key Finding: Enhanced vessel healing with improved endothelial function
Comparative Evidence Table
| Study Focus | BPC-157 Strength | TB-500 Strength | Winner |
|---|---|---|---|
| Tendon Healing | ★★★★★ (85% strength restoration) | ★★★☆☆ (Improved function) | BPC-157 |
| Muscle Regeneration | ★★★☆☆ (Accelerated healing) | ★★★★★ (Complete regeneration) | TB-500 |
| Bone Formation | ★★★★☆ (150% bone volume increase) | ★★☆☆☆ (Modest effects) | BPC-157 |
| Cardiac Protection | ★★★☆☆ (Arrhythmia protection) | ★★★★★ (50% scar reduction) | TB-500 |
| Vascular Healing | ★★★★☆ (Enhanced angiogenesis) | ★★★★☆ (Cell migration) | Tie |
| Neurological Effects | ★★★☆☆ (Neuroprotection) | ★★★★☆ (Nerve regeneration) | TB-500 |
| Administration Ease | ★★★★★ (Oral bioavailable) | ★★☆☆☆ (Injection only) | BPC-157 |
| Systemic Distribution | ★★★☆☆ (Dose-dependent) | ★★★★★ (Inherently systemic) | TB-500 |
Complete Dosing Protocols for Injury Recovery
BPC-157 Dosing Strategies
#### Beginner Protocol: Conservative Healing
Target: Minor injuries, maintenance, first-time users
Dose: 200-300 mcg daily
Administration: Subcutaneous injection near injury site OR 500 mcg oral (empty stomach)
Timing: Once daily, preferably morning
Duration: 2-4 weeks
Rationale: Minimal effective dose with excellent safety profile
*Reconstitution*: Add 2ml bacteriostatic water to 5mg vial = 250 mcg per 0.1ml
#### Standard Protocol: Active Recovery
Target: Moderate injuries, active recovery phases
Dose: 400-600 mcg daily
Administration: Subcutaneous injection, rotate sites
Timing: Split dose (200-300 mcg morning, 200-300 mcg evening)
Duration: 4-8 weeks
Rationale: Optimal balance of efficacy and sustainability
*Pro tip*: Inject within 2-3 inches of injury site for maximum local effects
#### Advanced Protocol: Aggressive Healing
Target: Severe injuries, competitive athletes, stubborn chronic issues
Dose: 800-1000 mcg daily
Administration: Subcutaneous injection + oral dosing
Timing: 400 mcg injection AM, 500-600 mcg oral PM
Duration: 6-12 weeks with periodic breaks
Rationale: Maximum therapeutic effect with systemic coverage
*Safety note*: Monitor for any unusual symptoms; reduce dose if side effects occur
TB-500 Dosing Strategies
#### Beginner Protocol: Introduction Phase
Target: New users, minor muscle injuries, general recovery
Dose: 2mg twice weekly (4mg/week total)
Administration: Subcutaneous injection, abdomen or thigh
Timing: Every 3-4 days (e.g., Monday/Thursday)
Duration: 4-6 weeks
Rationale: Standard effective dose with established safety
*Loading phase*: Some users prefer 2mg daily for first week, then twice weekly
#### Standard Protocol: Active Treatment
Target: Moderate muscle injuries, tendon issues, active recovery
Dose: 2.5mg twice weekly (5mg/week total)
Administration: Subcutaneous or intramuscular injection
Timing: Every 3-4 days with consistent schedule
Duration: 6-8 weeks
Rationale: Enhanced efficacy while maintaining twice-weekly convenience
*Injection sites*: Rotate between abdomen, thighs, glutes, and deltoids
#### Advanced Protocol: Maximum Recovery
Target: Severe injuries, post-surgical healing, competitive recovery
Dose: 5-7.5mg twice weekly (10-15mg/week total)
Administration: Intramuscular injection preferred for higher doses
Timing: Every 3-4 days, consider splitting larger doses
Duration: 8-12 weeks with monitoring
Rationale: Maximum therapeutic benefit for serious recovery needs
*High-dose considerations*: Some users split 5mg+ doses into multiple injection sites
Complete Dosing Reference Table
| Protocol Level | BPC-157 Dose | TB-500 Dose | Best For | Duration |
|---|---|---|---|---|
| Maintenance | 200 mcg/day | 2mg twice/week | Minor issues, prevention | 2-4 weeks |
| Active Recovery | 400-600 mcg/day | 2.5mg twice/week | Moderate injuries | 4-8 weeks |
| Aggressive Healing | 800-1000 mcg/day | 5mg twice/week | Severe injuries | 6-12 weeks |
| Post-Surgical | 600 mcg/day | 5-7.5mg twice/week | Surgery recovery | 8-12 weeks |
| Chronic Issues | 500 mcg/day | 2.5mg twice/week | Ongoing problems | 8-16 weeks |
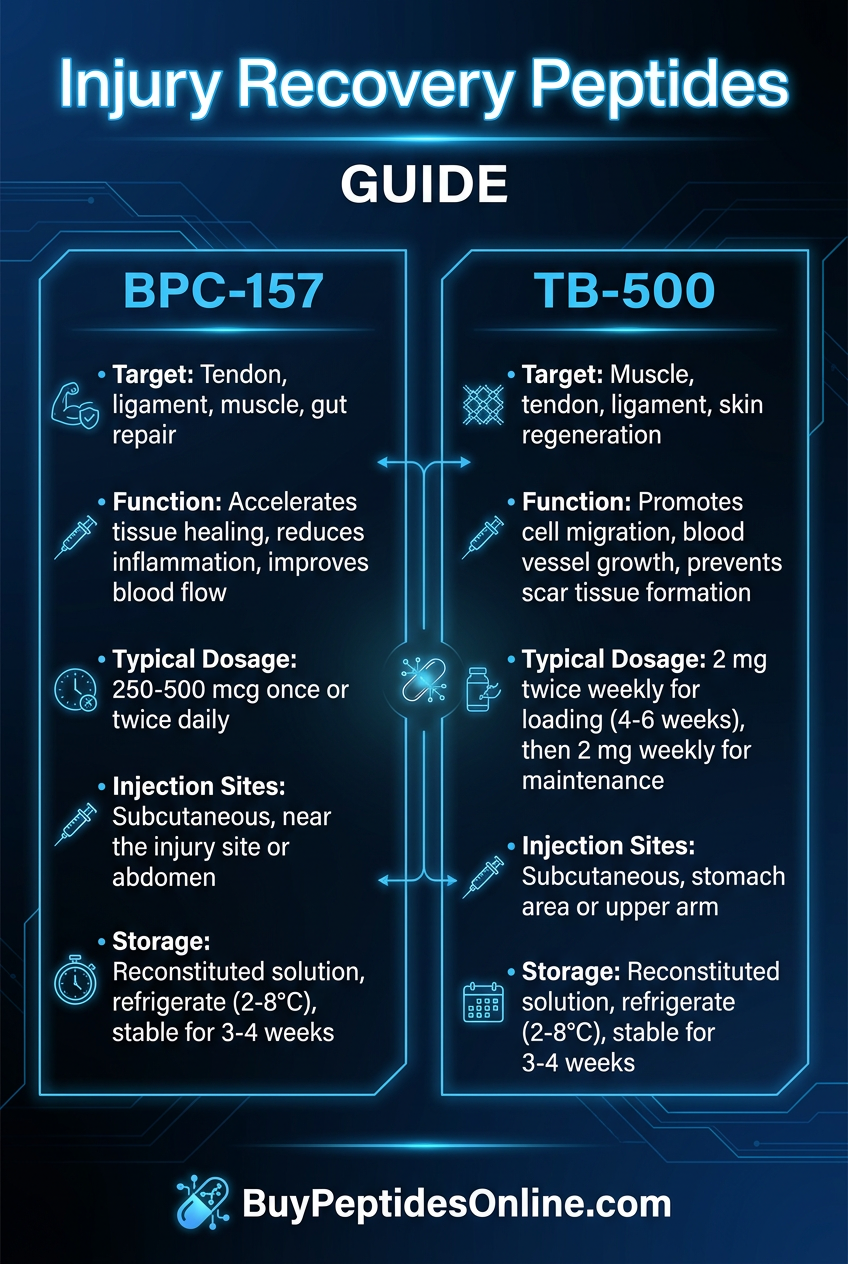
Storage and Reconstitution Guidelines
BPC-157 Storage:
Lyophilized powder: Room temperature up to 2 years
Reconstituted solution: Refrigerated 30-60 days
Bacteriostatic water preferred for multi-dose vials
Protect from direct sunlight
TB-500 Storage:
Lyophilized powder: Refrigerated for maximum stability
Reconstituted solution: Refrigerated 14-21 days maximum
Use sterile water for single-dose, bacteriostatic for multi-dose
Freeze reconstituted solution for longer storage (up to 6 months)
Strategic Stacking Protocols
Protocol 1: The Complete Injury Stack
Target: Comprehensive healing for complex injuries involving multiple tissue types
Combination: BPC-157 + TB-500 + Growth Hormone Support
Dosing Schedule:
BPC-157: 400 mcg daily, subcutaneous
TB-500: 2.5mg twice weekly, subcutaneous
CJC-1295: 100 mcg twice weekly (optional GH support)
Ipamorelin: 200 mcg twice weekly (optional GH support)
Timing Protocol:
Morning: BPC-157 (400 mcg)
Monday/Thursday: TB-500 (2.5mg)
Tuesday/Friday: CJC-1295 + Ipamorelin (if using)
Duration: 8-12 weeks with 4-week break
Mechanistic Rationale: BPC-157 provides targeted tendon/gut healing while TB-500 handles systemic muscle recovery. Growth hormone support amplifies overall tissue regeneration and protein synthesis.
Protocol 2: The Athletic Recovery Stack
Target: High-intensity training recovery, injury prevention, performance optimization
Combination: BPC-157 + TB-500 + Anti-inflammatory Support
Dosing Schedule:
BPC-157: 300 mcg daily, oral (gut protection)
TB-500: 2mg twice weekly, subcutaneous
BPC-157: Additional 200 mcg injection at problem areas
Timing Protocol:
Pre-workout: BPC-157 oral (300 mcg)
Post-workout: BPC-157 injection (200 mcg) if needed
Monday/Thursday: TB-500 (2mg)
Duration: 6-8 weeks on, 2-4 weeks off, repeat
Athletic Benefits: Combines systemic recovery (TB-500) with targeted protection (BPC-157). Oral BPC-157 provides gut integrity for better nutrient absorption and reduced inflammation.
Protocol 3: The Post-Surgical Healing Stack
Target: Accelerated recovery from surgery, scar tissue prevention, tissue restoration
Combination: High-dose BPC-157 + TB-500 + Collagen Support
Pre-Surgery Phase (1-2 weeks before):
BPC-157: 500 mcg daily, subcutaneous
TB-500: 5mg twice weekly, subcutaneous
Post-Surgery Phase (immediate recovery):
BPC-157: 600-800 mcg daily, injection near surgical site
TB-500: 5-7.5mg twice weekly, systemic injection
GHK-Cu: 2mg daily for collagen synthesis (optional)
Recovery Phase (4-12 weeks post-surgery):
BPC-157: 400-600 mcg daily, local injection
TB-500: 2.5-5mg twice weekly, systemic
Surgical Benefits: BPC-157 accelerates wound closure and prevents adhesions. TB-500 promotes tissue remodeling and reduces scar formation. Combined approach addresses both local healing and systemic recovery.
Stacking Safety Considerations
Synergistic Effects: BPC-157 and TB-500 work through complementary mechanisms—no negative interactions reported in literature. Enhanced healing effects are additive, not multiplicative.
Monitoring Protocol:
Weekly progress photos for visual tracking
Pain/function scoring (1-10 scale) daily
Blood work every 4-6 weeks for extended protocols
Professional assessment every 2-4 weeks
Red Flags: Discontinue if experiencing unusual pain, swelling, or any concerning symptoms. Both peptides have excellent safety profiles, but individual responses vary.
Safety Deep Dive: Risk Assessment and Management
BPC-157 Safety Profile
#### Common Side Effects (Frequency: <5% of users)
Injection Site Reactions:
Mild redness or swelling (2-3% incidence)
Temporary soreness lasting 12-24 hours
Rare: Small nodule formation (resolves within weeks)
Systemic Effects:
Mild fatigue in first week (adjustment period)
Occasional vivid dreams (mechanism unknown)
Rare: Mild nausea with oral administration
Management: Rotate injection sites, use smaller needles (30-31 gauge), reduce dose if persistent reactions occur.
#### Rare/Theoretical Risks
Angiogenesis Concerns: Theoretical risk of promoting unwanted blood vessel growth in cancer patients. No clinical evidence of tumor promotion, but cancer patients should avoid without oncologist approval.
Blood Pressure Effects: BPC-157 can lower blood pressure through NO pathway activation. Monitor BP if taking antihypertensive medications.
Coagulation Effects: May enhance platelet function and clotting. Use caution with anticoagulant medications.
#### Contraindications
Absolute Contraindications:
Active cancer diagnosis (theoretical growth factor concern)
Pregnancy/breastfeeding (insufficient safety data)
Known hypersensitivity to peptide therapies
Relative Contraindications:
Severe cardiovascular disease (monitor blood pressure)
Active bleeding disorders
Recent major surgery (timing considerations)
TB-500 Safety Profile
#### Common Side Effects (Frequency: <10% of users)
Injection Site Effects:
Mild soreness or stiffness (5-8% incidence)
Temporary fatigue following injection
Rare: Headache within 24 hours of injection
Systemic Effects:
Increased energy/restlessness (dose-dependent)
Enhanced recovery sensation (not technically a side effect)
Occasional mild joint stiffness (temporary)
Dose-Related Effects: Higher doses (>5mg) may cause more pronounced fatigue or energy fluctuations.
#### Rare/Theoretical Risks
Cancer Considerations: Like BPC-157, TB-500's cell migration effects raise theoretical concerns about cancer cell spread. No clinical evidence of cancer promotion, but active cancer is a contraindication.
Immune System Effects: TB-500 may modulate immune responses. Generally positive, but immunocompromised patients should consult healthcare providers.
Cardiac Effects: Beneficial for most users, but those with severe heart conditions should monitor carefully due to TB-500's cardiac activity.
#### Contraindications
Absolute Contraindications:
Active malignancy (metastasis risk theoretical but concerning)
Pregnancy/breastfeeding (insufficient data)
Severe immunocompromised states
Relative Contraindications:
Recent cardiac events (monitor closely)
Autoimmune conditions (immune modulation effects)
Major bleeding risks
Long-Term Safety Considerations
Extended Use Protocols: Both peptides show excellent long-term safety in animal studies extending 6+ months. Human data limited to shorter periods, but no concerning signals.
Tolerance Development: Neither peptide shows significant tolerance or dependence patterns. Efficacy may plateau after 8-12 weeks, suggesting natural cycling.
Recovery Periods: Most practitioners recommend 4-week breaks every 8-12 weeks to maintain sensitivity and allow natural healing mechanisms to reset.
Drug Interactions and Considerations
Blood Thinners: Both peptides may enhance healing, potentially affecting warfarin/heparin requirements. Monitor INR closely.
Growth Hormone: Synergistic effects possible—may enhance benefits but also increase growth factor exposure.
NSAIDs: No negative interactions, but NSAIDs may blunt healing responses that peptides are trying to enhance.
Steroids: Corticosteroids may counteract healing benefits. Consider timing and necessity of steroid medications during peptide protocols.
Head-to-Head Comparison: Which Peptide Wins?
Mechanism Comparison
| Feature | BPC-157 | TB-500 | Clinical Significance |
|---|---|---|---|
| Primary Target | Growth factor upregulation | Actin regulation | BPC-157 more targeted, TB-500 more systemic |
| Onset of Action | 24-48 hours | 48-72 hours | BPC-157 slight edge for immediate effects |
| Duration of Effect | 6-12 hours | 48-96 hours | TB-500 provides sustained activity |
| Bioavailability | High (oral + injection) | Moderate (injection only) | BPC-157 more convenient |
| Tissue Distribution | Dose-dependent | Inherently systemic | TB-500 better for multiple injuries |
| Half-life | ~4 hours | ~7-10 days | TB-500 allows less frequent dosing |
Efficacy by Injury Type
Tendon Injuries: BPC-157 Wins
Tennis elbow: BPC-157's anti-inflammatory effects more targeted
Muscle Injuries: TB-500 Wins
Contusions: TB-500's cell migration advantages clear
Chronic muscle pain: TB-500's systemic effects more comprehensive
Bone Healing: BPC-157 Wins
Fracture repair: BPC-157 shows superior callus formation
Bone defects: 150% greater bone volume with BPC-157
Joint healing: BPC-157's cartilage effects more pronounced
Cardiovascular: TB-500 Wins
Heart protection: TB-500's 50% scar reduction unmatched
Vascular healing: TB-500's angiogenesis more robust
Circulation: TB-500's systemic effects superior
Practical Considerations
Ease of Use: BPC-157 wins due to oral bioavailability option. TB-500 requires consistent injection schedule.
Cost Effectiveness: BPC-157 wins for most applications due to lower effective doses and dual administration options.
Side Effect Profile: Tie—both show excellent safety with minimal side effects.
Versatility: BPC-157 wins due to broader application range (gut, tendon, bone, vascular, neurological).
Athletic Performance: TB-500 wins for systemic recovery and muscle-focused benefits.
The Verdict: Injury-Specific Recommendations
Choose BPC-157 if you have:
Tendon or ligament injuries
Bone fractures or joint problems
Gut issues combined with injuries
Multiple small injuries
Preference for oral administration
Budget constraints
Choose TB-500 if you have:
Muscle tears or strains
Multiple muscle groups affected
Cardiovascular concerns
Need for systemic recovery
Tolerance for injection schedules
History of scar tissue formation
Choose both if you have:
Complex injuries involving multiple tissue types
Severe or chronic conditions
Post-surgical recovery needs
Athletic performance goals
Budget for comprehensive protocols
What's Coming Next: Future Research and Applications
BPC-157 Research Pipeline
Clinical Trials in Progress:
Phase II trial: for inflammatory bowel disease (University of Zagreb)
Phase I safety study: for oral administration in healthy volunteers
Veterinary trials: for equine tendon injuries (multiple locations)
Emerging Applications:
Traumatic brain injury: Early studies show neuroprotective effects
Diabetic wound healing: Promising results in diabetic ulcer models
Addiction recovery: Potential for dopamine system normalization
Aging-related tendon degeneration: Preventive applications being explored
Formulation Advances:
Sustained-release preparations: Monthly injection formulations in development
Topical formulations: Cream and gel preparations for localized application
Oral stability enhancement: Improved absorption and bioavailability research
TB-500 Research Directions
Current Clinical Development:
Cardiovascular applications: Heart failure trials showing promise
Wound healing studies: Diabetic foot ulcer clinical trials
Ophthalmology research: Corneal healing applications
Novel Applications:
Hair restoration: Clinical studies for androgenic alopecia
Skin aging: Anti-aging applications in dermatology
Neurological recovery: Stroke and traumatic brain injury research
Muscle wasting diseases: Potential for sarcopenia and cachexia
Delivery System Innovation:
Microneedle patches: Painless transdermal delivery systems
Inhalation formulations: Pulmonary delivery for systemic effects
Implantable devices: Continuous release implants for chronic conditions
Combination Therapy Research
BPC-157 + TB-500 Studies: Formal combination studies are beginning to evaluate synergistic effects and optimal dosing ratios.
Growth Factor Combinations: Research into combining with **IGF-1, MGF**, and other growth factors for enhanced healing.
Stem Cell Enhancement: Studies evaluating how these peptides enhance stem cell therapy outcomes.
Regulatory Landscape Evolution
FDA Considerations: Both peptides exist in regulatory gray areas. Potential pathways for approval as orphan drugs for specific conditions.
International Development: European and Asian regulatory agencies showing interest in peptide therapies for unmet medical needs.
Compounding Pharmacy Guidelines: Evolving regulations for custom peptide preparations and quality standards.
Technology Integration
Personalized Protocols: AI-driven dosing recommendations based on injury type, genetics, and response patterns.
Biomarker Development: Research into predictive markers for optimal peptide selection and dosing.
Wearable Integration: Smart devices to monitor healing progress and optimize peptide timing.
Key Takeaways: Your Peptide Selection Guide
• BPC-157 dominates tendon healing with 85% strength restoration in complete ruptures—unmatched by any other therapeutic intervention
• TB-500 excels in muscle regeneration through its unique actin-binding mechanism, promoting complete fiber regeneration rather than just scar tissue formation
• Injury location determines choice: BPC-157 for anything involving tendons, ligaments, bones, or gut; TB-500 for muscle tears, cardiac issues, or systemic recovery needs
• Administration flexibility favors BPC-157 with proven oral bioavailability, while TB-500 requires injection but provides longer-lasting systemic effects
• Dosing frequency differs significantly: BPC-157 needs daily administration (200-1000 mcg), TB-500 works with twice-weekly injections (2-7.5mg)
• Safety profiles are excellent for both with minimal side effects, but cancer patients should avoid due to theoretical growth factor concerns
• Combination protocols maximize results for complex injuries, with BPC-157 + TB-500 stacks showing additive benefits without negative interactions
• Cost-effectiveness favors BPC-157 for most applications due to lower effective doses and dual administration options
• Recovery timelines vary: BPC-157 shows effects in 24-48 hours, TB-500 takes 48-72 hours but provides sustained activity for days
• Future applications are expanding rapidly with clinical trials exploring cardiovascular, neurological, and anti-aging applications for both peptides
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Frequently Asked Questions
Q: Can I take BPC-157 and TB-500 together safely?
A: Yes, they work through complementary mechanisms with no reported negative interactions. Many users combine 400 mcg BPC-157 daily with 2.5mg TB-500 twice weekly.
Q: Which peptide works faster for injury healing?
A: BPC-157 typically shows effects within 24-48 hours, while TB-500 takes 48-72 hours but provides longer-lasting benefits due to its extended half-life.
Q: Do I need to inject both peptides or can I take them orally?
A: BPC-157 has proven oral bioavailability at 500-1000 mcg doses, while TB-500 requires injection due to poor oral absorption.
Q: How long should I use these peptides for injury recovery?
A: Most protocols run 4-8 weeks for acute injuries, 8-12 weeks for chronic conditions, with 4-week breaks recommended between cycles.
Q: Which peptide is better for multiple injuries at once?
A: TB-500's systemic distribution makes it superior for multiple injury sites, while BPC-157 works best when injected near specific problem areas.
Q: Are there any drug interactions I should worry about?
A: Both may enhance clotting and affect blood pressure. Monitor closely if taking blood thinners or antihypertensive medications.
Q: Can I use these peptides to prevent injuries?
A: Yes, many athletes use maintenance doses (BPC-157 200 mcg daily or TB-500 2mg weekly) for injury prevention and faster recovery.
Q: What's the difference in cost between BPC-157 and TB-500?
A: BPC-157 is generally more cost-effective due to lower effective doses, while TB-500's higher dosing requirements make it more expensive for equivalent treatment periods.
Related Articles on BuyPeptidesOnline.com
BPC-157 Complete Dosing and Administration Guide
TB-500 Mechanism of Action and Clinical Applications
Best Healing Peptides for Athletic Recovery
Peptide Stacking Protocols for Maximum Recovery
How to Choose Between Healing Peptides