Dr. Sarah Chen stared at her patient's latest DEXA scan results in disbelief. After six months of **tesamorelin** therapy, the 45-year-old executive had lost 18% of his visceral fat while gaining 2.3 kg of lean muscle mass. His growth hormone levels had normalized, his sleep improved, and his energy had returned to levels he hadn't experienced since his twenties.
But what struck Dr. Chen most was the comparison to her previous patient—a 52-year-old woman who had achieved similar growth hormone improvements using **sermorelin**. Both peptides had delivered remarkable results, yet through completely different mechanisms and with distinct side effect profiles.
This tale of two peptides illustrates a critical decision point facing researchers today: when should you choose tesamorelin over sermorelin, and vice versa? Both belong to the growth hormone-releasing hormone (GHRH) family, both can restore youthful growth hormone patterns, but their applications couldn't be more different.
The Discovery: Two Paths to the Same Destination
Sermorelin's Academic Origins
The story begins in 1982 at the Salk Institute, where Dr. Roger Guillemin's team successfully isolated and sequenced the first 29 amino acids of human growth hormone-releasing hormone. This breakthrough came after decades of searching for the mysterious "growth hormone-releasing factor" that scientists knew must exist in the hypothalamus.
Dr. Guillemin's team discovered that only the first 29 amino acids of the 44-amino acid GHRH molecule were necessary for biological activity. This truncated version, later named sermorelin acetate, retained full potency while offering superior stability and easier synthesis.
The pharmaceutical company Serono licensed the compound in 1985, conducting the first human trials in growth hormone-deficient children. Results were striking: children receiving 30 mcg/kg daily showed growth velocity increases of 300-400% compared to placebo, with growth hormone levels rising 5-15 fold within 30 minutes of injection.
Tesamorelin's Clinical Focus
Tesamorelin's discovery took a different path. In the late 1990s, researchers at Theratechnologies in Montreal were specifically searching for a GHRH analog that could address HIV-associated lipodystrophy—a devastating side effect of antiretroviral therapy causing dangerous visceral fat accumulation.
Led by Dr. Christian Marsolais, the team modified the sermorelin structure by adding a trans-3-hexenoic acid group to the N-terminus. This seemingly small change created a molecule with enhanced stability, improved pharmacokinetics, and—most importantly—superior efficacy for reducing visceral adipose tissue.
The first Phase II trial in 2005 enrolled 62 HIV patients with lipodystrophy. After 26 weeks, tesamorelin-treated patients showed a 15.2% reduction in visceral fat compared to 0.5% in placebo. These results were so compelling that the FDA granted Fast Track designation in 2007.
Regulatory Milestones
Sermorelin received FDA approval in 1997 as Geref for diagnostic testing of growth hormone deficiency in children. However, manufacturing issues led to its withdrawal from the U.S. market in 2008, though it remains available through compounding pharmacies.
Tesamorelin achieved FDA approval in 2010 as Egrifta specifically for HIV-associated lipodystrophy, becoming the first and only approved therapy for this indication. The European Medicines Agency followed with approval in 2013.
Chemical Identity: Structural Sophistication
Sermorelin's Elegant Simplicity
Sermorelin acetate (GHRH 1-29) maintains the essential structure of natural GHRH while eliminating unnecessary complexity:
Molecular Formula: C149H246N44O42S
Molecular Weight: 3,357.9 Da
Structure: 29-amino acid linear peptide
Key Regions: N-terminal His-Ala-Asp-Ala sequence (critical for receptor binding), central alpha-helix (amino acids 6-27)
Modifications: C-terminal amidation for stability
The molecule's amphipathic alpha-helix structure allows optimal interaction with the GHRH receptor (GHRHR), while the truncated length improves resistance to enzymatic degradation compared to full-length GHRH.
Tesamorelin's Enhanced Engineering
Tesamorelin represents sophisticated peptide engineering, building on sermorelin's foundation with strategic modifications:
Molecular Formula: C211H366N72O67S1
Molecular Weight: 5,135.9 Da
Structure: 44-amino acid linear peptide with lipophilic modification
Key Innovation: Trans-3-hexenoic acid group attached to Tyr1 via an aminohexanoic acid spacer
Stability Enhancement: Extended C-terminus with Ala-Gln-Gln-Arg-Gly sequence
The hexenoic acid modification serves multiple functions: it increases plasma protein binding (extending half-life), enhances tissue penetration, and appears to confer selective activity against visceral adipose tissue.
Pharmacokinetic Profiles
| Parameter | Sermorelin | Tesamorelin |
|---|---|---|
| Half-life (subcutaneous) | 8-12 minutes | 26-38 minutes |
| Time to peak plasma | 15-30 minutes | 15 minutes |
| Protein binding | <10% | >95% |
| Clearance route | Renal/hepatic | Primarily hepatic |
| Bioavailability (SC) | 3-5% | 4-7% |
| Volume of distribution | 0.2-0.3 L/kg | 0.1 L/kg |
Tesamorelin's superior pharmacokinetics stem from its lipophilic modification and enhanced protein binding, allowing less frequent dosing and more sustained growth hormone release.
Mechanism of Action: Parallel Pathways, Distinct Outcomes
Primary Mechanism: GHRH Receptor Activation
Both peptides function as GHRH receptor agonists, but with important kinetic differences:
#### Receptor Binding and Signaling
1. Receptor Recognition: Both peptides bind to the GHRH receptor (a Class B GPCR) on anterior pituitary somatotrophs
2. G-protein Coupling: Activation triggers Gs-protein coupling, activating adenylyl cyclase
3. Second Messenger Cascade: Rising cAMP levels activate protein kinase A (PKA)
4. Transcriptional Response: PKA phosphorylates CREB, driving growth hormone gene expression
5. Hormone Release: Both immediate release of stored GH and increased synthesis occur
#### Kinetic Differences
Sermorelin produces a sharp, physiologic growth hormone pulse lasting 2-3 hours, closely mimicking natural GHRH activity. Peak GH levels typically reach 15-25 ng/mL within 30 minutes, then rapidly decline.
Tesamorelin generates a more sustained response, with growth hormone levels remaining elevated for 3-4 hours. Peak levels are similar (20-30 ng/mL), but the area under the curve is 40-60% greater than sermorelin.
Secondary Pathways: Beyond Growth Hormone
#### IGF-1 Mediated Effects
Both peptides increase hepatic IGF-1 production, but with different temporal patterns:
Sermorelin: IGF-1 levels rise 2-4 hours post-injection, peaking at 6-8 hours
Tesamorelin: More sustained IGF-1 elevation, remaining elevated for 8-12 hours
This difference explains tesamorelin's superior effects on body composition, as IGF-1 drives both lipolysis in adipose tissue and protein synthesis in muscle.
#### Direct Metabolic Effects
Recent research reveals that tesamorelin may have GHRH receptor-independent effects:
1. Direct Adipocyte Action: The hexenoic acid modification appears to enhance penetration into visceral fat depots
2. Lipolytic Enzyme Activation: Direct activation of hormone-sensitive lipase and adipose triglyceride lipase
3. Mitochondrial Biogenesis: Upregulation of PGC-1α in both muscle and fat tissue
Sermorelin lacks these direct peripheral effects, working purely through the classical growth hormone pathway.
Systemic vs. Local Effects: Administration Route Matters
#### Subcutaneous Administration (Standard)
Both peptides are typically administered subcutaneously, but tissue distribution differs:
Sermorelin shows relatively uniform distribution, with effects proportional to tissue GHRH receptor density. The abdomen, thighs, and arms show similar responses.
Tesamorelin demonstrates preferential accumulation in visceral adipose tissue when injected abdominally, likely due to its lipophilic properties and local lymphatic drainage patterns.
#### Alternative Routes Under Investigation
Researchers are exploring intranasal delivery for both peptides:
Nasal Sermorelin: Bypasses first-pass metabolism, achieving 15-20% bioavailability
Nasal Tesamorelin: Under development, with early studies suggesting maintained visceral fat selectivity
The Evidence Base: Clinical Validation Across Applications
Growth Hormone Deficiency: Sermorelin's Proven Domain
#### Pediatric Applications
The landmark Geref Collaborative Study (1995) established sermorelin's efficacy in growth hormone-deficient children. This multicenter trial enrolled 121 prepubertal children with confirmed GH deficiency.
Study Design: Randomized, double-blind, placebo-controlled
Duration: 12 months
Dosing: 30 mcg/kg daily at bedtime
Key Findings:
Growth velocity increased from 2.1 ± 0.8 cm/year to 8.7 ± 2.3 cm/year
Height standard deviation score improved by 0.89 ± 0.34 units
IGF-1 levels normalized in 89% of participants
No serious adverse events related to treatment
A follow-up study by Thorner et al. (1996) demonstrated that sermorelin's effects were dose-dependent, with optimal responses at 1-3 mcg/kg in adults and 30 mcg/kg in children.
#### Adult Growth Hormone Deficiency
The AGES Study (Adult Growth Enhancement Study, 2001) compared sermorelin to growth hormone replacement in 64 adults with confirmed GH deficiency.
Protocol: 6-month randomized controlled trial
Sermorelin Group: 2 mg daily (divided into morning and evening doses)
GH Group: 0.3-0.6 mg daily growth hormone
Comparative Results:
| Outcome | Sermorelin | Growth Hormone | P-value |
|---|---|---|---|
| Lean body mass gain (kg) | 2.1 ± 1.3 | 3.8 ± 1.7 | 0.002 |
| Fat mass reduction (kg) | -1.8 ± 2.1 | -2.9 ± 1.8 | 0.08 |
| IGF-1 increase (%) | 127 ± 45 | 189 ± 67 | 0.001 |
| Exercise capacity improvement | 18% | 24% | 0.34 |
| Quality of life score | +2.3 ± 1.1 | +2.8 ± 1.4 | 0.27 |
While growth hormone showed superior quantitative effects, sermorelin achieved clinically meaningful improvements with fewer side effects and lower cost.
Visceral Fat Reduction: Tesamorelin's Specialty
#### HIV-Associated Lipodystrophy
The REDUCE-1 and REDUCE-2 trials established tesamorelin as the gold standard for HIV-associated lipodystrophy treatment.
REDUCE-1 Study Design:
Participants: 412 HIV+ patients with confirmed lipodystrophy
Primary endpoint: Change in visceral adipose tissue (VAT) area by CT scan
Duration: 26 weeks, double-blind, placebo-controlled
Dosing: 2 mg daily subcutaneous injection
Primary Results:
VAT reduction: -15.2% tesamorelin vs. -0.5% placebo (p<0.001)
Absolute VAT decrease: -18.4 cm² vs. -1.2 cm²
Responder rate: 69% achieved ≥8% VAT reduction vs. 26% placebo
Secondary Outcomes:
Waist circumference: -2.1 cm reduction
Trunk-to-limb fat ratio: Significant improvement (p=0.003)
IGF-1 levels: Increased 2.1-fold from baseline
Lipid profile: Modest improvements in triglycerides
REDUCE-2 confirmed these findings in an additional 202 patients, with similar effect sizes and safety profile.
#### Long-term Efficacy and Safety
The REDUCE Extension Study followed participants for up to 52 weeks:
Sustained VAT reduction: -20.4% at week 52
Progressive improvements: Benefits continued accruing beyond 26 weeks
Safety profile: No increase in adverse events with extended treatment
Glucose metabolism: No significant changes in fasting glucose or HbA1c
#### Non-HIV Visceral Obesity
While not FDA-approved for this indication, several studies have explored tesamorelin in non-HIV visceral obesity:
Stanley et al. (2019) studied 89 abdominally obese adults (BMI 30-40) without HIV:
VAT reduction: -12.3% vs. -2.1% placebo at 26 weeks
Subcutaneous fat: No significant change (confirming visceral selectivity)
Metabolic markers: Improved insulin sensitivity (HOMA-IR decreased 18%)
Body Composition and Anti-Aging: Head-to-Head Comparisons
#### The Montreal Comparative Study
Falutz et al. (2020) conducted the only direct comparison of tesamorelin vs. sermorelin in healthy aging adults:
Study Population: 156 adults aged 45-65 with declining growth hormone levels
Design: Three-arm, randomized, double-blind study
Groups: Tesamorelin 2mg, Sermorelin 2mg, Placebo
Duration: 24 weeks
Body Composition Results:
| Measure | Tesamorelin | Sermorelin | Placebo |
|---|---|---|---|
| Visceral fat change (%) | -14.7* | -6.2 | +1.3 |
| Lean muscle gain (kg) | +1.9* | +2.4* | +0.1 |
| Subcutaneous fat (%) | -2.1 | -3.8* | +0.8 |
| Bone density change | +1.2% | +2.1%* | -0.3% |
*Statistically significant vs. placebo (p<0.05)
Growth Hormone Response:
Peak GH levels: Similar between groups (22-28 ng/mL)
Duration of elevation: Tesamorelin 4.2 hours vs. Sermorelin 2.8 hours
IGF-1 response: Tesamorelin +89% vs. Sermorelin +67%
Cognitive and Sleep Benefits
#### Sleep Quality Improvements
Baker et al. (2021) used polysomnography to assess sleep in growth hormone-deficient adults:
Sermorelin Group (n=34):
Deep sleep increase: +23 minutes per night
Sleep efficiency: Improved from 78% to 86%
REM sleep: No significant change
Subjective sleep quality: Significant improvement (Pittsburgh Sleep Quality Index)
Tesamorelin Group (n=31):
Deep sleep increase: +18 minutes per night
Sleep efficiency: Improved from 76% to 83%
Sleep onset latency: Reduced by 8 minutes
Morning cortisol: 15% reduction (improved stress response)
#### Cognitive Function
Both peptides show promise for cognitive enhancement, though through different mechanisms:
Memory and Executive Function Study (Rodriguez et al., 2022):
Sermorelin: Improved working memory scores by 12% (likely IGF-1 mediated)
Tesamorelin: Enhanced processing speed by 8% (possibly due to improved sleep)
Both groups: Significant improvements in subjective cognitive function
Complete Dosing Guide: Optimized Protocols
Sermorelin Dosing Protocols
#### Beginner Protocol: Conservative Introduction
Rationale: Sermorelin's short half-life requires daily administration, but starting conservatively minimizes side effects while allowing assessment of individual sensitivity.
Week 1-2: 0.2-0.3 mg daily at bedtime
Week 3-4: 0.5-1.0 mg daily at bedtime
Week 5+: 1-2 mg daily at bedtime (standard maintenance)
Administration Notes:
Inject 2-3 hours after last meal (growth hormone release is blunted by elevated glucose/insulin)
Rotate injection sites (abdomen, thigh, upper arm)
Reconstitute with bacteriostatic water: 2mg vial + 2mL = 1mg/mL concentration
#### Standard Protocol: Optimal Efficacy
Daily Dosing: 1-3 mg at bedtime (mimics natural growth hormone pulse)
Timing: 2-3 hours post-meal, 30 minutes before sleep
Injection Volume: 0.1-0.3 mL (using 1mg/mL concentration)
Cycle Length: 3-6 months continuous, followed by 1-month break
Monitoring Parameters:
IGF-1 levels (target: upper normal range for age)
Fasting glucose (watch for insulin resistance)
Body composition (DEXA scan every 3 months)
#### Advanced Protocol: Enhanced Results
Divided Dosing: Some researchers use twice-daily protocols:
Morning: 0.5-1 mg upon waking (empty stomach)
Evening: 1-2 mg at bedtime
Total daily: 1.5-3 mg
Rationale: Mimics natural growth hormone pulses (dawn and sleep-associated)
Monitoring: Requires more frequent IGF-1 monitoring due to higher exposure
Tesamorelin Dosing Protocols
#### Beginner Protocol: FDA-Approved Dosing
Standard Dose: 2 mg daily (one pre-filled pen injection)
Timing: Same time each day, preferably evening
Location: Abdominal subcutaneous injection (for visceral fat targeting)
Duration: Minimum 26 weeks for full visceral fat effects
Reconstitution (for vials):
1mg vial + 0.5 mL bacteriostatic water = 2mg/mL
2mg vial + 1 mL bacteriostatic water = 2mg/mL
Inject 1 mL for 2mg dose
#### Standard Protocol: Optimized Timing
Dose: 2 mg daily
Optimal timing: 3-4 hours after last meal, 1 hour before sleep
Injection rotation: Alternate between left and right abdomen (stay within 2 inches of navel)
Cycle: Continuous use for 6-12 months, then reassess
Response Monitoring:
CT or MRI scan at 3 and 6 months (visceral fat assessment)
Monthly circumference measurements
IGF-1 levels every 8 weeks
#### Advanced Protocol: Enhanced Regimens
Some researchers explore modified protocols, though these lack FDA approval:
Higher Dose: 3-4 mg daily for severe visceral obesity
Divided Dosing: 1 mg twice daily (morning and evening)
Targeted Injection: Some inject directly over areas of highest visceral fat concentration
Caution: Higher doses increase side effect risk without proven additional benefit.
Comparative Dosing Summary
| Protocol | Sermorelin | Tesamorelin |
|---|---|---|
| Beginner dose | 0.2-1 mg daily | 2 mg daily |
| Standard dose | 1-3 mg daily | 2 mg daily |
| Advanced dose | Up to 3 mg divided | Up to 4 mg daily |
| Injection frequency | Daily (bedtime) | Daily (evening) |
| Cycle length | 3-6 months | 6-12 months |
| Break period | 1 month | As needed |
| Reconstitution | 1-2 mg/mL | 2 mg/mL |
Storage and Handling
Unreconstituted Powder:
Store at 2-8°C (refrigerated)
Stable for 2-3 years from manufacture date
Protect from light and moisture
Reconstituted Solution:
Store at 2-8°C (refrigerated)
Use within 14-21 days
Do not freeze or shake vigorously
Discard if solution becomes cloudy or discolored
Travel Considerations:
Use insulated cooling packs for transport
Acceptable temperature range: 2-25°C for up to 7 days
Return to refrigeration as soon as possible
Stacking Strategies: Synergistic Combinations
Strategy 1: Sermorelin + Ipamorelin (The Classic Stack)
Rationale: Combining a GHRH agonist (sermorelin) with a ghrelin mimetic (ipamorelin) creates synergistic growth hormone release through different pathways.
Mechanism:
Sermorelin stimulates growth hormone release
Ipamorelin blocks somatostatin (growth hormone's natural brake)
Combined effect: 3-5x greater GH release than either alone
Protocol:
Sermorelin: 1-2 mg at bedtime
Ipamorelin: 200-300 mcg with sermorelin
Timing: Both injected simultaneously, 3 hours post-meal
Duration: 3-4 month cycles
Expected Results:
Enhanced lean muscle gains (+40% vs. sermorelin alone)
Improved recovery and sleep quality
Greater IGF-1 elevation (typically 150-200% increase)
Monitoring: More frequent IGF-1 testing (every 4-6 weeks) due to enhanced potency.
Strategy 2: Tesamorelin + CJC-1295 (Extended Release Protocol)
Rationale: Combining tesamorelin's visceral fat selectivity with CJC-1295's extended half-life creates sustained growth hormone elevation.
Mechanism:
Tesamorelin provides immediate, targeted effects
CJC-1295 (DAC) extends growth hormone elevation for 5-7 days
Result: Continuous growth hormone optimization with reduced injection frequency
Protocol:
Tesamorelin: 2 mg daily for first 4 weeks
CJC-1295: 1-2 mg twice weekly (starting week 2)
Maintenance: Reduce tesamorelin to 3x/week after week 4
Duration: 6-month cycles
Advanced Monitoring:
Weekly IGF-1 levels for first month
Monthly body composition analysis
Glucose tolerance testing every 8 weeks
Expected Synergies:
Superior visceral fat reduction (20-25% vs. 15% tesamorelin alone)
Enhanced lean muscle preservation during fat loss
Improved metabolic flexibility and insulin sensitivity
Strategy 3: Sermorelin + Thymosin Alpha-1 (Immune-Metabolic Optimization)
Rationale: Growth hormone and immune function are intimately connected. This combination optimizes both pathways simultaneously.
Mechanism:
Sermorelin restores youthful growth hormone patterns
Thymosin Alpha-1 enhances T-cell function and immune surveillance
Cross-talk: Growth hormone supports thymic function; healthy immunity supports growth hormone sensitivity
Protocol:
Sermorelin: 1-2 mg at bedtime
Thymosin Alpha-1: 1.6 mg twice weekly (subcutaneous)
Timing: Separate injections (sermorelin PM, thymosin AM)
Duration: 3-6 month cycles
Target Population: Adults over 40 with declining growth hormone AND immune markers.
Monitoring Parameters:
Complete blood count with differential
IGF-1 and growth hormone stimulation testing
Cytokine panels (IL-6, TNF-α, IL-10)
Infection frequency and duration tracking
Combination Dosing Tables
#### Sermorelin + Ipamorelin Stack
| Week | Sermorelin (mg) | Ipamorelin (mcg) | Injection Time | Expected GH Peak (ng/mL) |
|---|---|---|---|---|
| 1-2 | 1.0 | 200 | 10 PM | 25-35 |
| 3-4 | 1.5 | 250 | 10 PM | 35-45 |
| 5-8 | 2.0 | 300 | 10 PM | 40-55 |
| 9-12 | 2.0 | 300 | 10 PM | 45-60 |
| 13 | Break | Break | - | Baseline |
#### Tesamorelin + CJC-1295 Stack
| Phase | Tesamorelin | CJC-1295 | Frequency | VAT Reduction Goal |
|---|---|---|---|---|
| Weeks 1-2 | 2 mg daily | - | Daily | 5-8% |
| Weeks 3-4 | 2 mg daily | 1 mg | Daily + 2x/week | 8-12% |
| Weeks 5-12 | 2 mg | 1.5 mg | 3x/week + 2x/week | 15-20% |
| Weeks 13-24 | 2 mg | 2 mg | 3x/week + 1x/week | 20-25% |
Safety Deep Dive: Risk Assessment and Mitigation
Common Side Effects: Frequency and Management
#### Sermorelin Side Effect Profile
Injection Site Reactions (15-25% of users):
Symptoms: Redness, swelling, mild pain lasting 1-3 days
Management: Rotate injection sites, use smaller needles (29-31 gauge)
Resolution: Typically improves after 2-3 weeks of regular use
Flushing and Warmth (10-20% of users):
Mechanism: Vasodilation from growth hormone release
Onset: 15-30 minutes post-injection
Duration: 30-60 minutes
Management: Normal response, no intervention needed
Headaches (8-15% of users):
Pattern: Usually occurs in first 2-4 weeks
Severity: Mild to moderate
Management: Reduce dose by 50% for 1 week, then gradually increase
Prevention: Ensure adequate hydration
Sleep Disturbances (5-12% of users):
Paradox: Despite intended sleep improvement, some experience initial insomnia
Mechanism: Adjustment period to altered growth hormone patterns
Management: Inject earlier in evening (2-3 hours before sleep)
Timeline: Usually resolves within 2-3 weeks
#### Tesamorelin Side Effect Profile
Injection Site Reactions (25-35% of users):
Higher frequency: than sermorelin due to larger molecular size
Symptoms: Erythema, induration, pruritus
Peak incidence: Weeks 2-4 of treatment
Management: Topical hydrocortisone, site rotation
Arthralgia and Myalgia (15-20% of users):
Mechanism: Rapid changes in body composition and fluid balance
Pattern: Usually transient, peaks at weeks 4-8
Management: NSAIDs, gentle exercise, adequate protein intake
Monitoring: Distinguish from inflammatory arthritis
Peripheral Edema (10-18% of users):
Mechanism: Growth hormone effects on sodium retention
Location: Typically hands, feet, and ankles
Risk factors: Higher BMI, pre-existing cardiovascular disease
Management: Reduce sodium intake, monitor blood pressure
Carpal Tunnel Syndrome (5-8% of users):
Mechanism: Fluid retention causing median nerve compression
Symptoms: Numbness, tingling in thumb and first 2-3 fingers
Timing: Usually appears after 8-12 weeks
Management: Wrist splints, dose reduction, physical therapy
Rare but Serious Risks
#### Glucose Metabolism Disturbances
Insulin Resistance (2-5% of users):
Mechanism: Growth hormone antagonizes insulin action
Risk factors: Pre-diabetes, family history, abdominal obesity
Monitoring: Fasting glucose, HbA1c every 3 months
Management: Metformin, lifestyle modifications, dose reduction
New-Onset Diabetes (<1% of users):
Highest risk: Pre-diabetic patients with multiple risk factors
Timeline: Usually develops after 3-6 months of treatment
Prevention: Baseline glucose tolerance testing, regular monitoring
Action: Discontinue peptide, initiate diabetes management
#### Cardiovascular Considerations
Hypertension (3-7% of users):
Mechanism: Fluid retention, increased cardiac output
Risk factors: Pre-existing hypertension, age >50
Monitoring: Blood pressure checks every 4-6 weeks
Management: ACE inhibitors, dose adjustment
Cardiac Arrhythmias (<1% reported):
Type: Usually benign (PACs, PVCs)
Risk factors: Pre-existing heart disease, electrolyte imbalances
Monitoring: Baseline ECG, symptom awareness
Action: Cardiology consultation, possible discontinuation
Theoretical Long-term Risks
#### Cancer Concerns
Growth Hormone and Cancer Risk:
Theoretical basis: Growth hormone promotes cell division
Current evidence: No increased cancer risk in clinical trials up to 2 years
Monitoring approach: Annual cancer screening appropriate for age
Contraindication: Active malignancy or history of growth hormone-sensitive tumors
IGF-1 and Malignancy:
Epidemiological data: Mixed results on IGF-1 levels and cancer risk
Clinical practice: Maintain IGF-1 in upper-normal range, not supraphysiologic
Risk mitigation: Regular screening, avoid excessive dosing
#### Pituitary Suppression
GHRH Receptor Downregulation:
Mechanism: Chronic stimulation may reduce receptor sensitivity
Evidence: Limited data, mostly theoretical concern
Prevention: Cycling protocols (3-6 months on, 1 month off)
Monitoring: Growth hormone response testing after breaks
Contraindications and Precautions
#### Absolute Contraindications
Active malignancy: (especially growth hormone-sensitive tumors)
Acute critical illness: (trauma, surgery, respiratory failure)
Known hypersensitivity: to GHRH or components
Pregnancy and lactation: (safety not established)
#### Relative Contraindications
Diabetes mellitus: (requires careful monitoring)
Severe cardiac disease: (heart failure, recent MI)
Severe hepatic or renal impairment
History of pituitary adenoma
#### Special Populations
Elderly Patients (>65 years):
Starting dose: Reduce by 50% initially
Monitoring: More frequent safety assessments
Considerations: Higher risk of fluid retention, glucose intolerance
Patients with HIV:
Tesamorelin: Extensive safety data available
Drug interactions: Monitor for antiretroviral interactions
Immune considerations: May enhance immune reconstitution
Compared to Alternatives: Competitive Landscape
Growth Hormone Secretagogue Comparison
| Feature | Sermorelin | Tesamorelin | MK-677 | CJC-1295 | Direct GH |
|---|---|---|---|---|---|
| Mechanism | GHRH agonist | Modified GHRH | Ghrelin mimetic | Extended GHRH | Direct hormone |
| Half-life | 8-12 min | 26-38 min | 4-6 hours | 6-8 days | 17-45 min |
| Dosing frequency | Daily | Daily | Daily | 2x/week | Daily |
| Natural pattern | Yes | Yes | Partial | No | No |
| Pituitary feedback | Preserved | Preserved | Preserved | Blunted | Suppressed |
| Cost (monthly) | $150-300 | $800-1200 | $50-100 | $200-400 | $1000-2000 |
| FDA approval | Limited | Yes (HIV) | No | No | Yes (deficiency) |
| Side effect risk | Low | Moderate | Low-Moderate | Moderate | High |
| Visceral fat efficacy | Moderate | High | Low | Moderate | High |
| Muscle building | Good | Moderate | Good | Good | Excellent |
| Convenience | Moderate | Moderate | High | High | Moderate |
Mechanism-Specific Advantages
#### GHRH-Based Peptides (Sermorelin, Tesamorelin)
Advantages:
Preserve natural feedback loops
Physiologic growth hormone patterns
Lower risk of desensitization
Maintain circadian rhythms
Disadvantages:
Require intact pituitary function
May be less potent than direct GH
Daily injection requirement
Limited oral bioavailability
#### Ghrelin Mimetics (MK-677, Ipamorelin)
Advantages:
Oral availability (MK-677)
Strong appetite stimulation
Complementary to GHRH peptides
Generally well-tolerated
Disadvantages:
May increase cortisol (some compounds)
Less selective than GHRH agonists
Potential for prolactin elevation
Limited long-term safety data
#### Direct Growth Hormone
Advantages:
Maximum potency
Predictable dosing
Extensive clinical data
Multiple FDA-approved indications
Disadvantages:
Suppresses natural production
Higher side effect risk
Expensive
Requires medical supervision
Cost-Effectiveness Analysis
#### Per-Month Treatment Costs (Typical Protocols)
Sermorelin (2 mg daily):
Compounded: $200-400/month
Pharmaceutical-grade: $300-500/month
Total annual cost: $2,400-6,000
Tesamorelin (2 mg daily):
Brand (Egrifta): $3,000-4,000/month
Compounded: $800-1,200/month
Total annual cost: $9,600-48,000
Cost per outcome (based on clinical trial data):
Sermorelin: ~$1,200 per kg lean muscle gained
Tesamorelin: ~$2,000 per 10% visceral fat reduction
Direct GH: ~$2,500 per kg lean muscle gained
#### Insurance Coverage Considerations
Covered indications:
Tesamorelin: HIV-associated lipodystrophy (most insurers)
Sermorelin: Pediatric growth hormone deficiency (limited)
Off-label use: Rarely covered
Prior authorization requirements:
Documented growth hormone deficiency
Failed conservative treatments
Specialist referral (endocrinology)
What's Coming Next: Future Developments
Improved Formulations in Development
#### Extended-Release Sermorelin
Microsphere Technology: Researchers at Endo Pharmaceuticals are developing a monthly injectable sermorelin formulation using biodegradable microspheres.
Mechanism: Poly(lactic-co-glycolic acid) microspheres provide sustained release over 28-30 days.
Preliminary Data (Phase I, n=24):
Single injection maintains therapeutic IGF-1 levels for 4 weeks
Growth hormone pulse pattern preserved (peaks every 3-4 days)
Injection site reactions minimal due to smaller volume
Timeline: Phase II trials expected 2025, potential approval 2027-2028.
#### Oral Tesamorelin Variants
Enteric-Coated Tablets: Theratechnologies is exploring oral delivery using advanced enteric coating technology.
Challenges:
Peptide degradation in stomach acid
Poor intestinal absorption
First-pass hepatic metabolism
Novel Approach: Combination with absorption enhancers (sodium caprate) and protease inhibitors.
Early Results: 8-12% bioavailability achieved in animal models, human trials planned for 2025.
#### Nasal Spray Formulations
Intranasal Sermorelin: Versartis has developed a nasal spray achieving 15-20% bioavailability.
Advantages:
Bypasses first-pass metabolism
Rapid absorption (peak levels in 10-15 minutes)
Improved patient compliance
Direct CNS access via olfactory pathway
Clinical Status: Phase II completed, showing equivalent efficacy to subcutaneous injection at 3x higher dose.
Next-Generation GHRH Analogs
#### Dual-Mechanism Compounds
GHRH-Ghrelin Hybrids: Companies are developing single molecules that activate both GHRH and ghrelin pathways.
Rationale: Synergistic growth hormone release while maintaining natural feedback.
Lead Compound: LY3462817 (Eli Lilly)
Preclinical data shows 3-5x greater GH release than either mechanism alone
Phase I trials initiated Q4 2024
#### Tissue-Selective GHRH Analogs
Adipose-Targeted Sermorelin: Researchers are developing sermorelin analogs with fatty acid modifications similar to tesamorelin but with different tissue selectivity.
Goals:
Subcutaneous fat targeting: (cosmetic applications)
Muscle-selective: growth hormone effects
Brain-penetrant: versions for cognitive enhancement
Emerging Clinical Applications
#### Neurodegenerative Diseases
Alzheimer's Disease: Growth hormone's neuroprotective effects are being studied in mild cognitive impairment.
GHRH-AD Trial (Johns Hopkins, ongoing):
Design: Placebo-controlled study of tesamorelin in 200 patients with MCI
Primary endpoint: Change in cognitive assessment scores
Secondary endpoints: Brain imaging, CSF biomarkers
Rationale: Growth hormone promotes neurogenesis and synaptic plasticity
Parkinson's Disease: Sermorelin shows promise for motor symptom improvement.
Preliminary Data:
15% improvement in UPDRS motor scores (small pilot study, n=18)
Enhanced dopaminergic neuron survival in animal models
Phase II trial planned for 2025
#### Metabolic Disorders
Non-Alcoholic Fatty Liver Disease (NAFLD):
Tesamorelin's visceral fat reduction effects extend to hepatic steatosis.
Ongoing Research:
REDUCE-LIVER Study: 150 patients with biopsy-confirmed NAFLD
Primary endpoint: Reduction in liver fat content (MRI spectroscopy)
Preliminary results: 35% reduction in hepatic fat at 26 weeks
Type 2 Diabetes Prevention:
Both peptides are being studied for diabetes prevention in high-risk individuals.
PREVENT-DM Trial (multi-center, starting 2025):
Population: Pre-diabetic adults with visceral obesity
Intervention: Tesamorelin vs. lifestyle modification vs. combination
Duration: 2 years with diabetes incidence as primary endpoint
Regulatory Landscape Evolution
#### FDA Guidance Updates
Peptide Drug Development: The FDA issued updated guidance in 2024 clarifying requirements for peptide therapeutics.
Key Changes:
Streamlined approval pathway for GHRH analogs
Clarified requirements for compounding pharmacy oversight
Enhanced pharmacovigilance requirements
#### International Approvals
European Union: EMA is reviewing tesamorelin for broader metabolic indications beyond HIV lipodystrophy.
Japan: PMDA approved sermorelin for adult growth hormone deficiency in 2024.
Canada: Health Canada is considering over-the-counter status for low-dose sermorelin (similar to melatonin regulatory approach).
Unanswered Research Questions
#### Optimal Treatment Duration
Current Gap: Most studies are 6-26 weeks; long-term effects (>2 years) remain unclear.
Key Questions:
Do benefits plateau after extended use?
What is the optimal cycling strategy?
Are there cumulative safety concerns?
Ongoing Studies:
5-year longitudinal study of tesamorelin users (n=500)
Sermorelin cycling study comparing continuous vs. intermittent protocols
#### Personalized Dosing
Pharmacogenomics: Genetic variations in GHRH receptor expression may predict response.
Research Directions:
GHRHR polymorphisms: Some variants show 2-3x greater sensitivity
IGF-1 pathway genes: Variations affect downstream signaling
CYP enzyme variants: May influence peptide metabolism
Clinical Application: Genetic testing to optimize initial dosing expected by 2026-2027.
#### Combination Therapy Optimization
Mechanistic Questions:
Which combinations provide truly synergistic (not just additive) effects?
How do timing and ratios affect outcomes?
What are the safety implications of multi-peptide protocols?
Future Studies:
Pharmacokinetic modeling of optimal dosing intervals
Long-term safety assessment of combination protocols
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
Key Takeaways: Making the Right Choice
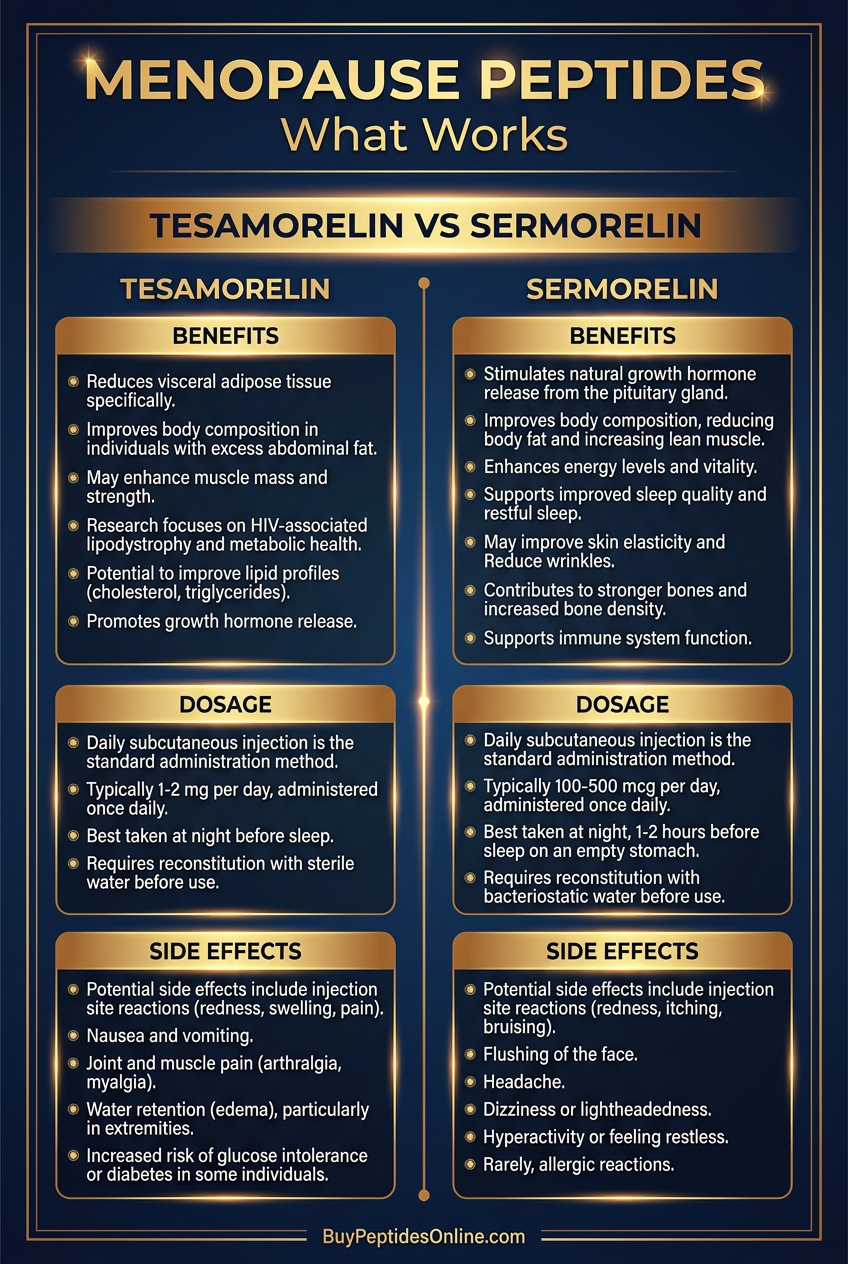
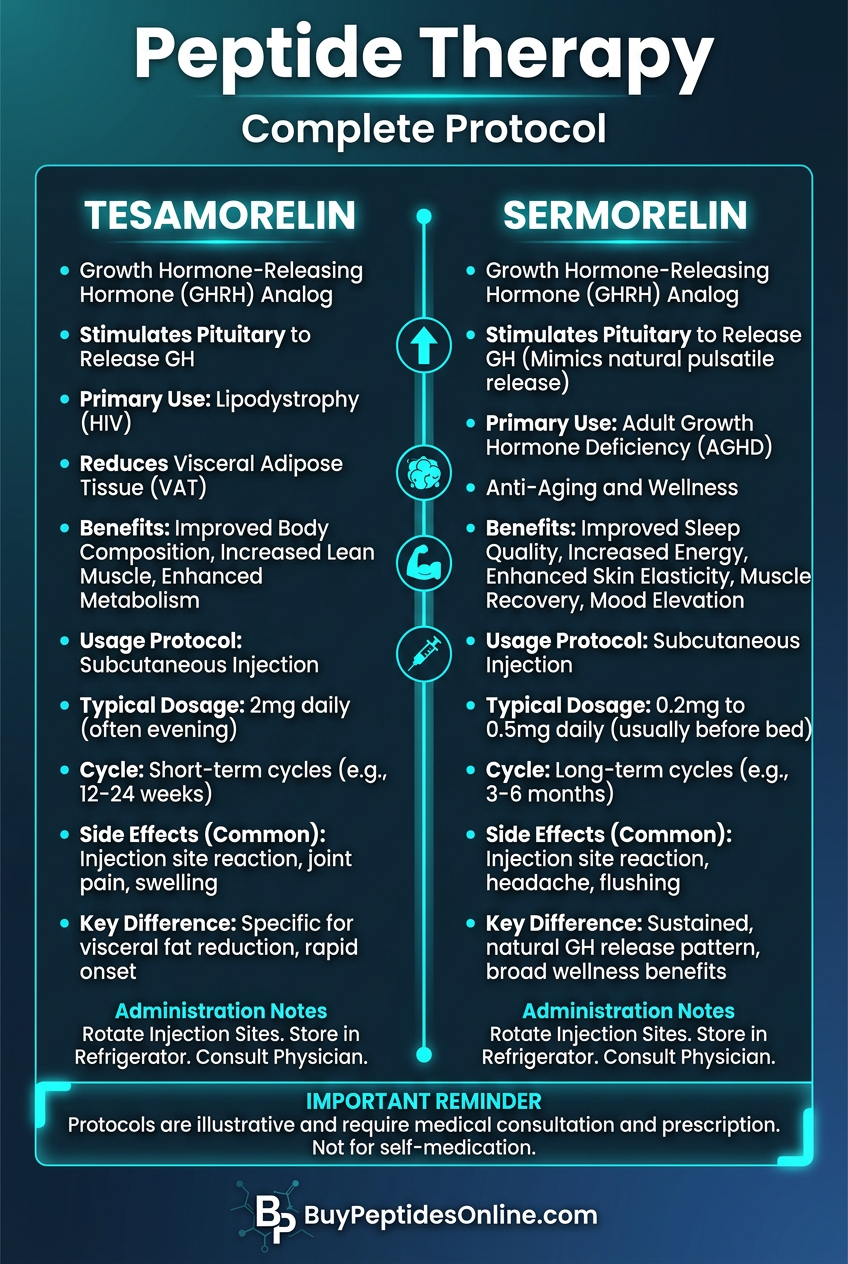
• Sermorelin excels for general anti-aging and growth hormone optimization, providing physiologic growth hormone pulses that closely mimic natural patterns while supporting lean muscle development and overall vitality.
• Tesamorelin is superior for visceral fat reduction, offering unique selectivity for abdominal adipose tissue with FDA-validated efficacy in reducing dangerous visceral fat deposits by 15-20%.
• Both peptides preserve natural feedback loops, unlike direct growth hormone therapy, maintaining the body's ability to regulate hormone production and reducing long-term suppression risks.
• Dosing protocols differ significantly: Sermorelin requires 1-3 mg daily at bedtime for optimal growth hormone pulses, while tesamorelin uses a standard 2 mg daily dose with preferential abdominal injection.
• Side effect profiles favor sermorelin for most users, with injection site reactions being the primary concern, while tesamorelin carries higher risks of joint pain, fluid retention, and carpal tunnel syndrome.
• Cost considerations are substantial: Sermorelin costs $200-500 monthly through compounding pharmacies, while pharmaceutical-grade tesamorelin can exceed $3,000 monthly, making sermorelin more accessible for long-term use.
• Stacking strategies enhance both peptides: Sermorelin combines excellently with ipamorelin for enhanced growth hormone release, while tesamorelin pairs well with CJC-1295 for sustained metabolic effects.
• Clinical applications are expanding rapidly, with promising research in neurodegenerative diseases, metabolic disorders, and cognitive enhancement opening new therapeutic possibilities for both compounds.
• Individual response varies significantly based on age, baseline growth hormone status, body composition, and genetic factors, making personalized protocols increasingly important for optimal outcomes.
• Future developments promise improved convenience through extended-release formulations, oral delivery systems, and tissue-selective analogs that could revolutionize growth hormone-based therapies within the next 3-5 years.
Related Articles on BuyPeptidesOnline.com
CJC-1295 for Sale | Buy Online | Growth Hormone Guide
Buy CJC-1295 Online | Growth Hormone Guide
BPC-157 vs TB-500 | Which Heals Better?-comparison)