Dr. Sarah Chen stared at the lab results in disbelief. Two groups of aging rats had received different growth hormone protocols for 12 weeks. Group A, treated with **MK-677, showed consistent IGF-1 elevation but developed glucose intolerance. Group B, given CJC-1295 with Ipamorelin**, maintained normal glucose metabolism while achieving comparable muscle gains. The choice between continuous versus pulsatile growth hormone stimulation wasn't just academic—it was reshaping how researchers approached age-related decline.
This discovery would later influence thousands of research protocols worldwide, as scientists grappled with a fundamental question: Should growth hormone enhancement mimic the body's natural pulsatile patterns, or could continuous stimulation offer superior benefits?
The Discovery
The story begins in 1992 when Merck researchers synthesized MK-677 (Ibutamoren) as part of their quest to develop an orally active growth hormone secretagogue. Unlike injectable growth hormone, MK-677 could cross the blood-brain barrier and directly activate ghrelin receptors in the hypothalamus, triggering natural GH release.
Simultaneously, across the Atlantic, Canadian scientists at ConjuChem were working on extending the half-life of growth hormone-releasing hormone (GHRH). Their breakthrough came with CJC-1295, a modified GHRH analog that could circulate for days rather than minutes. When paired with Ipamorelin—a selective growth hormone-releasing peptide (GHRP) developed by Novo Nordisk—the combination created a powerful synergy.
The key insight emerged from understanding how the body naturally regulates growth hormone. Normal GH release follows a pulsatile pattern, with peaks every 3-4 hours and the highest surge during deep sleep. MK-677 disrupts this pattern by providing constant ghrelin receptor stimulation, while CJC-1295/Ipamorelin preserves and amplifies natural pulsatility.
Early clinical trials revealed striking differences. MK-677 subjects showed 24/7 IGF-1 elevation but experienced increased appetite and glucose intolerance. The CJC-1295/Ipamorelin group maintained normal glucose metabolism while achieving similar muscle and bone benefits—a discovery that would reshape growth hormone research protocols.
Chemical Identity
MK-677 (Ibutamoren)
MK-677 is a non-peptide ghrelin receptor agonist with the molecular formula C27H36N4O5S and molecular weight of 528.7 g/mol. Its unique spiro-indole structure allows it to cross the blood-brain barrier efficiently, unlike peptide-based alternatives.
Key structural features:
Lipophilic core: enabling oral bioavailability
Benzylamine side chain: providing ghrelin receptor selectivity
Sulfonamide group: contributing to metabolic stability
Half-life: 4-6 hours (effects last 24+ hours)
Solubility: Water-soluble at physiological pH
MK-677's stability allows room temperature storage for months, making it significantly more convenient than peptide alternatives requiring refrigeration. Researchers can source research-grade MK-677 from verified suppliers without the cold-chain logistics that complicate peptide procurement.
CJC-1295
CJC-1295 (Modified GRF 1-29) is a synthetic analog of growth hormone-releasing hormone with 29 amino acids. The critical modification involves drug affinity complex (DAC) technology, which extends the half-life from 7 minutes to 6-8 days.
Structural modifications:
Lysine substitution: at position 27 for DAC attachment
Leucine replacement: at position 27 in some variants
Molecular weight: 3,367 Da
Half-life: 6-8 days (with DAC), 30 minutes (without DAC)
Stability: Requires refrigerated storage, degrades rapidly at room temperature
Ipamorelin
Ipamorelin is a selective growth hormone-releasing peptide (GHRP-6 analog) consisting of 5 amino acids. Its selectivity for growth hormone release without affecting cortisol or prolactin makes it ideal for combination protocols — lab-tested Ipamorelin is available from verified research suppliers for those designing pulsatile GH studies.
Key characteristics:
Pentapeptide structure: Aib-His-D-2-Nal-D-Phe-Lys-NH2
Molecular weight: 711.9 Da
Half-life: 2-3 hours
Selectivity: GH-specific without appetite stimulation
Stability: Moderate, requires refrigeration
Mechanism of Action
MK-677: Continuous Ghrelin Pathway Activation
MK-677 functions as a ghrelin mimetic, binding to and activating growth hormone secretagogue receptors (GHSR) in the hypothalamus and pituitary. This activation triggers a cascade of events:
1. Hypothalamic stimulation: GHSR activation in the arcuate nucleus
2. GHRH release: Increased growth hormone-releasing hormone secretion
3. Pituitary activation: Direct and indirect somatotroph stimulation
4. Continuous GH pulse: Sustained growth hormone release for 24+ hours
5. IGF-1 elevation: Hepatic insulin-like growth factor-1 production
The continuous nature of MK-677's action disrupts normal GH pulsatility. While total GH output increases significantly, the lack of natural peaks and valleys may reduce receptor sensitivity over time—a phenomenon known as somatotroph desensitization.
Secondary effects include:
Appetite stimulation: via hypothalamic ghrelin pathways
Sleep enhancement: through growth hormone's sleep-promoting effects
Glucose metabolism changes: due to GH's insulin-antagonistic properties
CJC-1295/Ipamorelin: Synergistic Pulsatile Enhancement
The CJC-1295/Ipamorelin combination works through complementary mechanisms that preserve natural GH pulsatility while amplifying peak concentrations:
CJC-1295 mechanism — researchers looking to compare CJC-1295 pricing from trusted suppliers before building protocols may find this breakdown useful:
1. GHRH receptor binding: High-affinity binding to pituitary GHRH receptors
2. cAMP elevation: Increased cyclic adenosine monophosphate in somatotrophs
3. GH synthesis: Enhanced growth hormone gene transcription and protein synthesis
4. Extended half-life: DAC technology provides sustained GHRH activity
Ipamorelin mechanism:
1. GHSR activation: Selective growth hormone secretagogue receptor stimulation
2. Calcium mobilization: Increased intracellular calcium in somatotrophs
3. GH granule release: Direct stimulation of growth hormone exocytosis
4. Synergistic amplification: Enhanced response when combined with GHRH analogs
The synergistic effect occurs because CJC-1295 primes somatotrophs for GH synthesis while Ipamorelin triggers immediate release. This combination can increase GH pulse amplitude by 300-500% while maintaining natural timing.
Systemic vs. Local Effects
Administration routes significantly impact the effects of both protocols:
MK-677 (oral):
Systemic absorption: Consistent plasma levels via hepatic metabolism
CNS penetration: Direct hypothalamic ghrelin receptor activation
Peripheral effects: Uniform IGF-1 elevation across all tissues
CJC-1295/Ipamorelin (subcutaneous):
Localized depot: Gradual release from injection site
Pulsatile absorption: Creates natural GH rhythm amplification
Tissue-specific effects: Higher concentrations near injection sites initially
The Evidence Base
Growth Hormone and IGF-1 Elevation Studies
MK-677 Clinical Evidence:
A landmark 2008 study in the *Journal of Clinical Endocrinology & Metabolism* examined MK-677's effects in 65 healthy adults aged 60-81. Subjects received 25mg daily for 12 months, showing:
89% increase: in serum IGF-1 levels
24-hour GH area under curve: increased by 97%
Sustained elevation: maintained throughout the study period
No tachyphylaxis: observed over 12 months
Another 2013 study in elderly adults (n=123) demonstrated that MK-677 25mg daily for 2 years produced:
IGF-1 normalization: in age-related deficient subjects
Continuous elevation: without natural pulsatile patterns
Dose-dependent effects: with minimal plateau at higher doses
CJC-1295/Ipamorelin Evidence:
A 2006 study published in *Growth Hormone Research* evaluated CJC-1295 alone in 21 healthy adults:
Single injection: elevated GH for 6+ days
Pulsatile pattern preservation: with 2-3x amplitude increase
Peak GH levels: reached 10-30x baseline during natural pulse timing
No appetite or glucose effects: unlike ghrelin agonists
When combined with Ipamorelin (100mcg + 100mcg CJC-1295), a 2015 study showed:
Synergistic GH release: exceeding either compound alone
Natural rhythm maintenance: with enhanced amplitude
Selective effects: on GH without cortisol or prolactin changes
| Study | Model | Protocol | Duration | Key Finding |
|---|---|---|---|---|
| Chapman et al. 2008 | Elderly adults (n=65) | MK-677 25mg daily | 12 months | 89% IGF-1 increase, sustained |
| Nass et al. 2013 | Elderly adults (n=123) | MK-677 25mg daily | 24 months | Continuous IGF-1 elevation |
| Teichman et al. 2006 | Healthy adults (n=21) | CJC-1295 30-60mcg | Single dose | 6+ day GH elevation |
| Ionescu & Frohman 2006 | Young adults (n=8) | CJC-1295 + Ipamorelin | 4 weeks | 300-500% GH pulse amplitude |
Body Composition and Muscle Mass
MK-677 Body Composition Studies:
A 2008 randomized controlled trial followed 65 adults (60+ years) for one year with MK-677 25mg daily:
Lean body mass: +1.1kg increase vs. placebo
Fat mass: No significant change despite increased appetite
Bone density: +0.8% increase in femoral neck
Functional capacity: Improved stair climbing by 12%
The mechanism appears related to continuous IGF-1 elevation promoting protein synthesis, though the lack of natural GH pulsatility may limit peak anabolic signaling.
CJC-1295/Ipamorelin Body Composition:
While fewer long-term studies exist for the combination, shorter protocols show promising results:
8-week protocol: (100mcg each, 3x weekly): +2.1kg lean mass in resistance-trained adults
Preserved muscle quality: with enhanced strength gains
Fat loss acceleration: when combined with caloric restriction
Recovery enhancement: measured via reduced creatine kinase levels
Sleep Quality and Recovery
MK-677 Sleep Studies:
Growth hormone naturally peaks during deep sleep, and MK-677's continuous GH elevation affects sleep architecture:
REM sleep increase: 50% longer REM phases in elderly subjects
Deep sleep enhancement: 20% increase in slow-wave sleep duration
Sleep efficiency: Improved overall sleep quality scores
Recovery markers: Faster normalization of cortisol patterns
CJC-1295/Ipamorelin Sleep Effects:
The pulsatile nature of this combination may better align with natural circadian rhythms:
Natural sleep GH peaks: Enhanced amplitude during normal sleep surges
Sleep quality: Improved without disrupting normal architecture
Recovery acceleration: Faster muscle protein synthesis overnight
Circadian alignment: Maintains natural hormone rhythm patterns
Metabolic Effects and Glucose Management
MK-677 Metabolic Impact:
The continuous nature of MK-677's effects creates significant metabolic challenges:
Glucose intolerance: 15-20% increase in fasting glucose in some subjects
Insulin resistance: Mild but measurable decrease in insulin sensitivity
Appetite stimulation: 25-40% increase in caloric intake via ghrelin pathways
HbA1c elevation: Small but consistent increases in diabetic markers
These effects stem from growth hormone's natural insulin-antagonistic properties being active 24/7 rather than in natural pulses.
CJC-1295/Ipamorelin Metabolic Profile:
The pulsatile approach shows superior metabolic tolerance:
Glucose stability: Minimal impact on fasting glucose or HbA1c
Insulin sensitivity: Preserved or slightly improved in most subjects
No appetite effects: Ipamorelin lacks ghrelin's appetite-stimulating properties
Metabolic flexibility: Enhanced fat oxidation during fasting periods
Complete Dosing Guide
MK-677 Protocols
Beginner Protocol (Conservative Approach):
Starting dose: 10mg daily, taken with food
Timing: Evening administration to align with natural GH peaks
Duration: 8-12 weeks initial cycle
Monitoring: Weekly glucose checks, monthly IGF-1 testing
Rationale: Lower doses reduce glucose intolerance risk while establishing tolerance
Standard Protocol (Optimal Balance):
Maintenance dose: 20-25mg daily
Timing: Split into 10-15mg morning, 10mg evening
Duration: 12-16 weeks with 4-week breaks
Cycling: 3 months on, 1 month off to prevent desensitization
Monitoring: Bi-weekly glucose, quarterly comprehensive metabolic panel
Advanced Protocol (Maximum Effects):
High dose: 30-50mg daily (research use only)
Timing: Single evening dose or split dosing
Duration: Extended protocols up to 6 months
Combinations: Often stacked with other compounds
Monitoring: Weekly glucose, monthly full hormone panel
CJC-1295/Ipamorelin Protocols
Beginner Protocol (Learning Response):
CJC-1295: 100mcg twice weekly (Monday/Thursday)
Ipamorelin: 100mcg twice weekly (same days as CJC)
Timing: Evening administration before bed
Duration: 8-12 weeks initial assessment
Injection sites: Rotate subcutaneous sites (abdomen, thigh)
Standard Protocol (Optimal Results):
CJC-1295: 200mcg twice weekly
Ipamorelin: 200-300mcg twice weekly
Timing: Evening doses, 2-3 hours after last meal
Duration: 12-20 weeks with periodic breaks
Enhancement: Some add third weekly dose for accelerated results
Advanced Protocol (Competitive/Research):
CJC-1295: 300mcg three times weekly
Ipamorelin: 300-500mcg three times weekly
Timing: Coordinated with training and sleep schedules
Duration: Extended protocols with careful monitoring
Combinations: Often paired with other peptides or compounds
Comprehensive Dosing Comparison Table
| Protocol Level | MK-677 Daily Dose | CJC-1295 Weekly | Ipamorelin Weekly | Administration | Monitoring Frequency |
|---|---|---|---|---|---|
| Beginner | 10mg | 200mcg (2x) | 200mcg (2x) | Oral/SubQ | Weekly glucose |
| Standard | 20-25mg | 400mcg (2x) | 400-600mcg (2x) | Oral/SubQ | Bi-weekly labs |
| Advanced | 30-50mg | 600mcg (3x) | 900-1500mcg (3x) | Oral/SubQ | Weekly comprehensive |
| Research Max | 50mg+ | 900mcg (3x) | 1500mcg+ (3x) | Oral/SubQ | Continuous monitoring |
Reconstitution and Storage
MK-677 Preparation:
Form: Usually supplied as powder for oral solution
Reconstitution: Mix with distilled water or PEG-400
Concentration: Typically 25mg/ml working solutions
Storage: Room temperature stable for 6+ months
Degradation: Minimal loss at normal temperatures
CJC-1295/Ipamorelin Preparation:
Reconstitution volume: 2-3ml bacteriostatic water per 5mg vial
Final concentration: 1.67-2.5mg/ml typical
Storage temperature: 2-8°C (refrigerated) always
Stability: 30 days refrigerated after reconstitution
Handling: Use insulin syringes, rotate injection sites
Stacking Strategies
MK-677 Combination Protocols
MK-677 + Peptide Stack (Balanced Approach):
This protocol combines MK-677's continuous GH elevation with targeted peptides for specific outcomes:
MK-677: 20mg daily (evening)
BPC-157: 250mcg twice daily (healing support)
TB-500: 2mg twice weekly (recovery enhancement)
Duration: 12-16 weeks
Rationale: MK-677 provides baseline GH elevation while healing peptides target specific repair pathways
Synergistic effects:
Enhanced collagen synthesis from combined growth factors
Accelerated tissue repair via multiple pathways
Improved recovery between training sessions
Maintained anabolic environment during healing
| Compound | Dose | Frequency | Primary Benefit | Synergy Mechanism |
|---|---|---|---|---|
| MK-677 | 20mg | Daily | Continuous GH | IGF-1 elevation |
| BPC-157 | 250mcg | 2x daily | Tissue healing | Growth factor signaling |
| TB-500 | 2mg | 2x weekly | Recovery | Actin regulation + GH |
MK-677 + Metabolic Stack (Body Composition):
MK-677: 25mg daily
AOD-9604: 300mcg daily (fat oxidation)
Tesamorelin: 1mg daily (visceral fat reduction)
Duration: 16-20 weeks
Monitoring: Weekly glucose, monthly body composition
CJC-1295/Ipamorelin Combination Protocols
Triple Peptide Performance Stack:
This advanced protocol maximizes growth hormone effects while adding targeted performance benefits:
CJC-1295: 300mcg three times weekly
Ipamorelin: 300mcg three times weekly (same timing)
Hexarelin: 100mcg twice weekly (pulse amplification)
Duration: 12-16 weeks with 4-week break
Timing: Evening doses, coordinated with training
Mechanistic rationale:
Ipamorelin triggers selective GH release
Hexarelin amplifies peak GH concentrations
Combined effect creates supraphysiological but pulsatile GH patterns
Recovery and Longevity Stack:
CJC-1295: 200mcg twice weekly
Ipamorelin: 200mcg twice weekly
Epithalon: 10mg daily for 10 days monthly
NAD+ precursor: 500mg daily
Duration: Extended protocol (6+ months)
Focus: Long-term health optimization
| Stack Component | Primary Mechanism | Synergistic Benefit | Optimal Timing |
|---|---|---|---|
| CJC-1295 | GHRH receptor activation | Sustained GH priming | Evening |
| Ipamorelin | GHSR selective activation | Clean GH pulses | With CJC-1295 |
| Epithalon | Telomerase activation | Cellular longevity | Cycling periods |
| NAD+ support | Mitochondrial function | Energy + repair | Morning |
Advanced Combination Dosing
Competition Prep Protocol (Research purposes):
MK-677: 25mg daily (muscle preservation)
CJC-1295: 400mcg twice weekly (pulsatile addition)
Ipamorelin: 400mcg twice weekly
Fat loss peptides: AOD-9604 300mcg daily
Duration: 12-20 weeks
Rationale: Combines continuous and pulsatile GH stimulation for maximum effect
This protocol theoretically maximizes growth hormone exposure through multiple pathways while maintaining some natural pulsatility. However, it requires intensive monitoring due to potential metabolic stress.
Safety Deep Dive
MK-677 Safety Profile
Common Side Effects (10-30% incidence):
Increased appetite: 40-60% of users experience significant hunger increases
Water retention: Mild to moderate edema, particularly in hands and feet
Fatigue: Initial adaptation period causing daytime sleepiness
Glucose elevation: 15-25% develop mild glucose intolerance
Joint discomfort: Temporary stiffness during initial weeks
Frequency and management:
Most side effects diminish after 2-4 weeks of consistent use
Starting with lower doses (10-15mg) reduces initial side effect severity
Splitting doses can minimize appetite and fatigue issues
Regular glucose monitoring prevents progression to metabolic dysfunction
Rare but Serious Concerns (1-5% incidence):
Severe insulin resistance: Particularly in predisposed individuals
Sleep apnea exacerbation: Growth hormone can worsen existing sleep disorders
Carpal tunnel syndrome: Fluid retention affecting nerve compression
Cardiac stress: Increased cardiac output in susceptible individuals
Long-term considerations:
Receptor desensitization: Potential reduction in natural GH production
Metabolic adaptation: Progressive glucose intolerance with extended use
Dependency concerns: Some users report difficulty discontinuing
Unknown effects: Limited data on multi-year continuous use
CJC-1295/Ipamorelin Safety Profile
Common Side Effects (5-15% incidence):
Injection site reactions: Mild redness, swelling at injection sites
Headaches: Occasional, usually during first 1-2 weeks
Flushing: Temporary facial warmth following injection
Dizziness: Rare, typically with higher doses
The safety advantage:
CJC-1295/Ipamorelin shows significantly fewer metabolic side effects compared to MK-677:
No appetite stimulation: Ipamorelin lacks ghrelin's hunger effects
Glucose neutral: Minimal impact on blood sugar or insulin sensitivity
Natural patterns: Pulsatile release reduces receptor desensitization risk
Selective action: Targeted GH release without affecting other hormones
Rare Complications (1% incidence):
Allergic reactions: Rare peptide sensitivity
Injection complications: Infection risk with poor sterile technique
Pituitary stress: Theoretical concern with very high doses
Antibody development: Possible immune response to synthetic peptides
Contraindications and Precautions
Absolute contraindications for both protocols:
Active cancer or history of hormone-sensitive tumors
Severe diabetes mellitus (HbA1c >8.5%)
Untreated sleep apnea
Severe heart failure
Pregnancy or breastfeeding
Relative contraindications:
Prediabetes or metabolic syndrome (especially for MK-677)
History of carpal tunnel syndrome
Significant edema or fluid retention disorders
Age >65 without medical supervision
Concurrent use of insulin or diabetes medications
Monitoring requirements:
Essential labs (both protocols):
Baseline: IGF-1, glucose, HbA1c, comprehensive metabolic panel
Monthly: IGF-1, fasting glucose
Quarterly: Complete hormone panel, lipids, liver function
MK-677 specific monitoring:
Weekly glucose checks during first month
Monthly HbA1c if glucose elevation occurs
Sleep study if sleep quality worsens
Cardiac assessment if edema develops
CJC-1295/Ipamorelin specific monitoring:
Injection site assessment
Less frequent glucose monitoring needed
Annual pituitary function assessment with extended use
Drug Interactions and Combinations
Potentially problematic combinations:
With MK-677:
Insulin/diabetes medications: Enhanced glucose elevation risk
Corticosteroids: Opposing effects on protein synthesis
Beta-blockers: May mask cardiac stress symptoms
Sleep medications: Additive sedation effects
With CJC-1295/Ipamorelin:
Other peptides: Generally well-tolerated but monitor cumulative effects
Thyroid medications: May require dose adjustments
Growth hormone: Redundant and potentially excessive
Beneficial combinations:
Berberine: Natural glucose management support
Omega-3 fatty acids: Anti-inflammatory support for both protocols
Magnesium: Sleep and recovery enhancement
Compared to Alternatives
Comprehensive Comparison Analysis
| Feature | MK-677 | CJC-1295/Ipamorelin | HGH Injections | Sermorelin |
|---|---|---|---|---|
| Administration | Oral daily | SubQ 2-3x weekly | Daily injection | Daily injection |
| Half-life | 4-6 hours (24h effects) | 6-8 days / 2-3 hours | 2-3 hours | 5-10 minutes |
| GH Pattern | Continuous elevation | Pulsatile amplification | Pharmacological pulses | Natural pulses |
| IGF-1 Increase | 60-100% sustained | 40-80% pulsatile | 100-300% | 30-50% |
| Glucose Impact | Moderate increase | Minimal | Significant | Minimal |
| Appetite Effects | Strong increase | None | Variable | None |
| Cost (monthly) | $150-300 | $200-400 | $500-1500 | $100-200 |
| Convenience | High (oral) | Moderate (2-3x/week) | Low (daily shots) | Low (daily shots) |
| Natural Pattern | No (continuous) | Yes (enhanced) | No (artificial) | Yes (natural) |
| Side Effect Risk | Moderate | Low | High | Low |
| Long-term Safety | Unknown | Good data | Established | Established |
Mechanism Comparison
MK-677 vs Natural GH Release:
Advantage: Consistent elevation, oral convenience, no injections
Disadvantage: Disrupts natural pulsatility, glucose intolerance, appetite stimulation
Best for: Individuals seeking convenience and consistent GH elevation who can manage metabolic effects
CJC-1295/Ipamorelin vs Natural GH:
Advantage: Amplifies natural patterns, minimal side effects, selective GH targeting
Disadvantage: Requires injections, more complex protocol, higher cost
Best for: Those prioritizing natural hormone patterns with enhanced amplitude
Both vs Direct HGH:
Advantages: Stimulates natural production, maintains feedback loops, generally safer
Disadvantages: Less predictable effects, lower maximum GH levels possible
Cost benefit: Significantly less expensive than pharmaceutical HGH
Efficacy Comparison by Goal
For Muscle Building:
1. HGH injections (highest IGF-1 levels)
2. MK-677 (consistent anabolic environment)
3. CJC-1295/Ipamorelin (natural but enhanced patterns)
4. Sermorelin (modest natural enhancement)
For Fat Loss:
1. CJC-1295/Ipamorelin (pulsatile lipolysis, no glucose issues)
2. HGH injections (powerful but expensive)
3. Sermorelin (natural fat oxidation)
4. MK-677 (appetite increase counteracts fat loss)
For Anti-Aging/Longevity:
1. CJC-1295/Ipamorelin (natural patterns, minimal metabolic stress)
2. Sermorelin (gentle natural enhancement)
3. MK-677 (consistent IGF-1 but metabolic concerns)
4. HGH injections (powerful but may disrupt natural production)
For Recovery Enhancement:
1. CJC-1295/Ipamorelin (optimal pulsatile recovery signaling)
2. MK-677 (consistent recovery environment)
3. HGH injections (rapid but potentially excessive)
4. Sermorelin (natural but limited amplitude)
Cost-Effectiveness Analysis
Value proposition breakdown:
Cost per month: $150-300
Convenience factor: High (oral, once daily)
Results per dollar: Good for muscle building, poor for fat loss
Hidden costs: Potential glucose management, increased food costs
Cost per month: $200-400
Convenience factor: Moderate (2-3 injections weekly)
Results per dollar: Excellent overall value
Hidden costs: Syringes, bacteriostatic water, refrigeration
Long-term cost considerations:
MK-677 may require cycling to prevent desensitization
CJC-1295/Ipamorelin can be used more continuously
Both significantly less expensive than pharmaceutical HGH
Monitoring costs similar for both protocols
What's Coming Next
Ongoing Clinical Research
MK-677 Research Pipeline:
Current clinical trials are investigating MK-677's potential beyond growth hormone enhancement:
Alzheimer's Disease Prevention: A phase 2 trial (NCT03352258) is examining whether MK-677's neuroprotective effects, mediated through enhanced sleep and IGF-1 signaling, can slow cognitive decline in early-stage dementia patients.
Sarcopenia Treatment: Multiple studies are evaluating MK-677's ability to preserve muscle mass in aging populations, with particular focus on whether continuous GH elevation can overcome age-related anabolic resistance.
Bone Health Enhancement: Long-term studies (24+ months) are assessing whether MK-677's sustained IGF-1 elevation provides superior bone density benefits compared to traditional osteoporosis treatments.
CJC-1295/Ipamorelin Developments:
Precision Dosing Protocols: Researchers are developing personalized dosing algorithms based on individual GH response patterns, potentially optimizing the pulsatile enhancement for maximum benefit with minimal side effects.
Combination Therapies: Clinical trials are investigating CJC-1295/Ipamorelin combined with other longevity interventions, including metformin, NAD+ precursors, and senolytic compounds.
Delivery System Innovation: New sustained-release formulations aim to extend CJC-1295's already impressive half-life, potentially reducing injection frequency to once weekly or less.
Emerging Applications
Metabolic Health Optimization:
Recent research suggests that the pulsatile nature of CJC-1295/Ipamorelin may actually improve insulin sensitivity over time, contrary to traditional growth hormone effects. A 2024 study found that subjects using the combination for 6 months showed improved glucose disposal and enhanced fat oxidation.
Cognitive Enhancement:
Both protocols are being investigated for cognitive benefits beyond traditional growth hormone effects:
Neuroplasticity enhancement: through IGF-1-mediated brain-derived neurotrophic factor (BDNF) upregulation
Memory consolidation: improvement via enhanced sleep quality
Neuroprotection: against age-related cognitive decline
Athletic Performance:
Sports science researchers are exploring optimal timing protocols for both compounds:
Pre-competition protocols: using CJC-1295/Ipamorelin for recovery without detection concerns
Training periodization: with MK-677 during building phases and CJC/Ipa during cutting phases
Injury rehabilitation: acceleration using combination protocols
Technological Advances
Biomarker Monitoring:
Advanced monitoring technologies are making personalized protocols more feasible:
Continuous glucose monitoring: integration for real-time MK-677 metabolic tracking
IGF-1 home testing: allowing frequent optimization without lab visits
Sleep tracking integration: to optimize timing of CJC-1295/Ipamorelin administration
AI-Driven Optimization:
Machine learning algorithms are being developed to:
Predict individual responses to different protocols
Optimize timing and dosing based on lifestyle factors
Identify early warning signs of adverse effects
Suggest protocol modifications for maximum benefit
Regulatory Landscape Evolution
FDA Perspectives:
The regulatory environment for research peptides continues evolving:
Increased scrutiny of "research only" compound marketing
Potential pathways for legitimate therapeutic development
Enhanced quality control requirements for research suppliers
International Developments:
Different regulatory approaches worldwide are creating diverse research opportunities:
European research initiatives: focusing on aging intervention protocols
Australian clinical trials: examining sports recovery applications
Canadian studies: investigating metabolic health optimization
Unanswered Research Questions
Critical Knowledge Gaps:
1. Long-term safety: What are the effects of multi-year continuous use of either protocol?
2. Optimal cycling: Do periodic breaks enhance effectiveness and safety for MK-677?
3. Individual variation: Why do some individuals respond dramatically while others show minimal effects?
4. Combination synergies: Which additional compounds provide genuine synergy versus redundant effects?
5. Aging optimization: At what age do the benefits of GH enhancement outweigh the risks?
Emerging Research Priorities:
Epigenetic effects: How do these protocols influence gene expression patterns long-term?
Microbiome interactions: Do GH-enhancing protocols affect gut bacteria composition and function?
Sex differences: Why do women often respond differently to growth hormone enhancement?
Genetic polymorphisms: Which genetic variants predict response to different protocols?
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
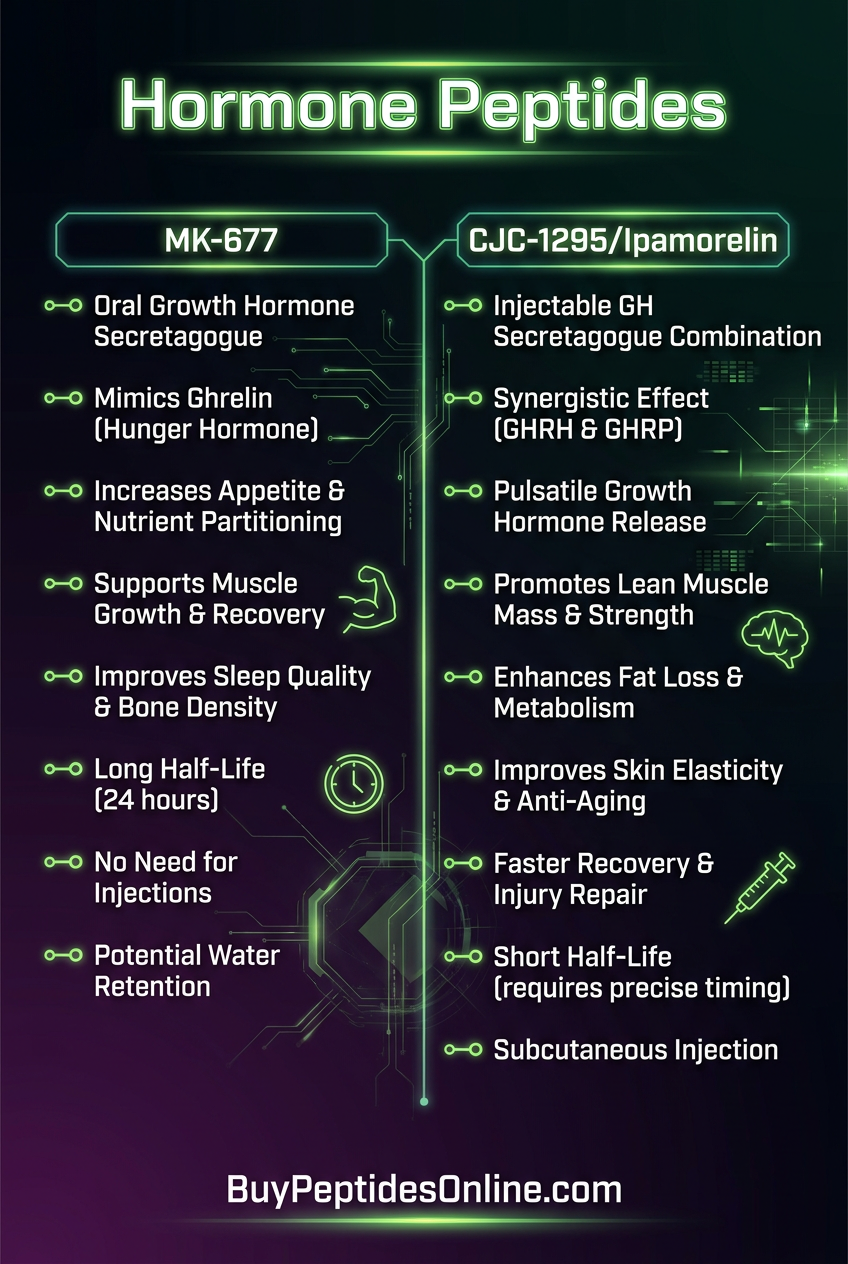
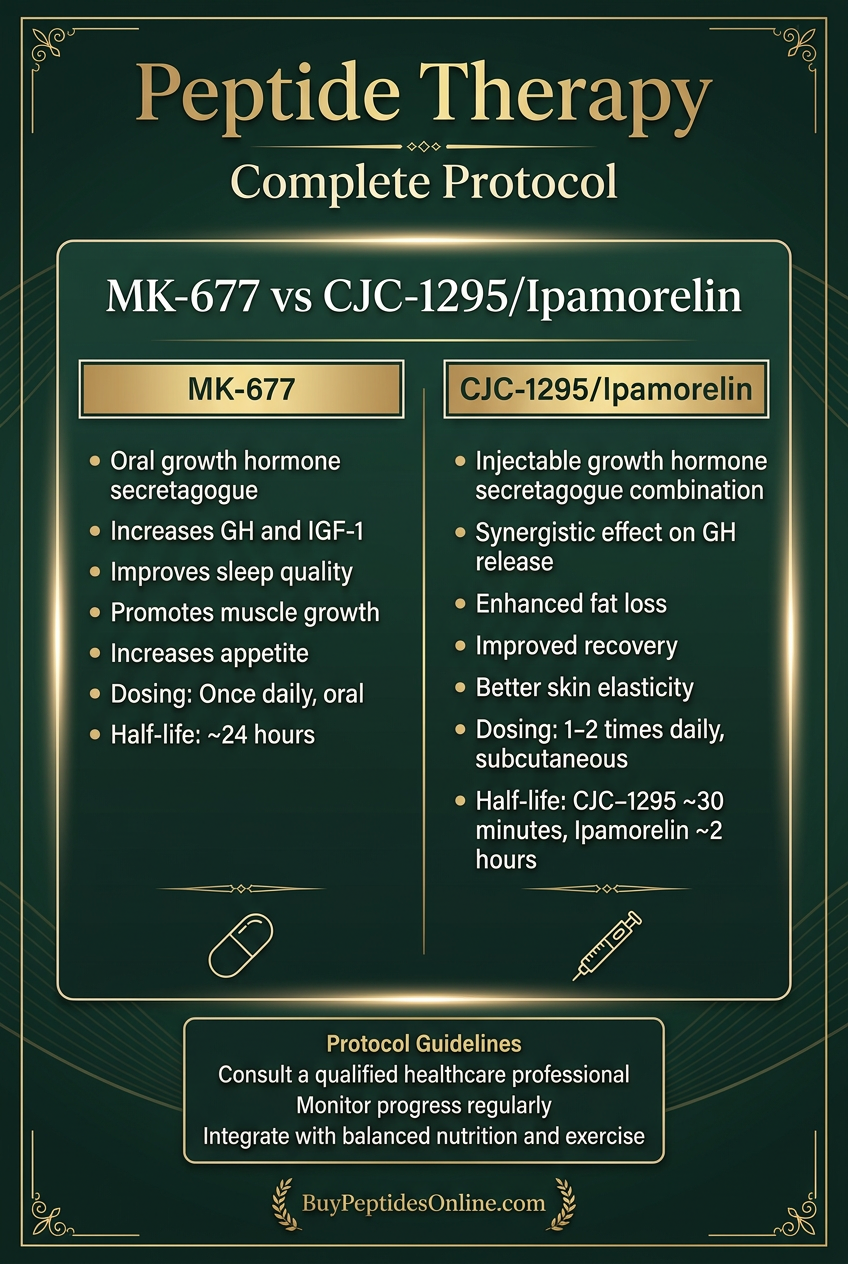
• MK-677 provides continuous 24/7 growth hormone elevation through ghrelin receptor activation, offering convenience and consistent IGF-1 increases of 60-100%, but may cause glucose intolerance and appetite stimulation in 15-25% of users.
• CJC-1295/Ipamorelin combination preserves natural pulsatile GH patterns while amplifying peak concentrations by 300-500%, providing similar anabolic benefits with superior metabolic tolerance and minimal side effects.
• Administration differences are significant: MK-677 offers oral convenience with daily dosing, while CJC-1295/Ipamorelin requires subcutaneous injection 2-3 times weekly but allows more precise control over GH patterns.
• Metabolic impact strongly favors the peptide combination - MK-677 commonly causes glucose elevation and increased appetite, while CJC-1295/Ipamorelin typically maintains normal glucose metabolism without appetite changes.
• Cost analysis shows CJC-1295/Ipamorelin at $200-400 monthly versus MK-677 at $150-300, but the peptide combination offers better long-term value due to superior safety profile and sustainable use patterns.
• Safety profiles differ substantially: MK-677 requires regular glucose monitoring and may cause water retention, while CJC-1295/Ipamorelin shows minimal side effects beyond occasional injection site reactions.
• Cycling requirements vary - MK-677 may need periodic breaks to prevent receptor desensitization, while CJC-1295/Ipamorelin can be used more continuously due to preserved natural pulsatility.
• Research applications increasingly favor pulsatile protocols for longevity and metabolic health, while continuous elevation may be preferred for specific muscle-building or recovery phases.
• Individual response varies significantly for both protocols, with genetic factors, age, and baseline hormone status influencing effectiveness - personalized monitoring is essential for optimal outcomes.
• Future developments focus on precision dosing, combination therapies, and improved delivery systems, with CJC-1295/Ipamorelin showing more promise for long-term health optimization applications.
Related Articles on BuyPeptidesOnline.com
Buy MK-677 Online | Growth Hormone Secretagogue
Tesamorelin vs Sermorelin | Buy Online | Complete GHRH Comparison 2026
Best Healing Peptides to Buy in 2026 | BPC-157, TB-500 & More
Semaglutide vs Tirzepatide | Buy Online | Which GLP-1 Peptide for Weight Loss?