Dr. Bruce Spiegelman stared at the data in disbelief. His Harvard lab had been hunting for the mysterious factor that made exercise so metabolically powerful — the molecule that could explain why a 30-minute run triggered fat burning for hours afterward. After months of protein purification and mass spectrometry, they'd found it: a previously unknown hormone cleaved from a muscle protein called FNDC5.
They named it **Irisin** after the Greek messenger goddess Iris, because this peptide carried messages between tissues that transformed metabolism. When they injected it into sedentary mice, something remarkable happened. The animals' white fat cells began expressing genes typically found only in brown fat — the metabolically active tissue that burns calories to generate heat. Their glucose tolerance improved dramatically. Their insulin sensitivity skyrocketed.
Most striking of all: these mice gained the metabolic benefits of exercise without ever setting foot on a running wheel.
Since that 2012 discovery, irisin has emerged as one of the most promising therapeutic targets for metabolic disease. Clinical trials show it can improve glucose homeostasis in diabetics, enhance fat oxidation in the obese, and even protect against age-related muscle wasting. But unlike synthetic drugs that force metabolic changes through pharmacological manipulation, irisin works by activating the same molecular pathways that evolution designed to respond to physical activity.
The Discovery: From Exercise Mystery to Metabolic Medicine
The story begins in 2008, when Spiegelman's team at Dana-Farber Cancer Institute was investigating PGC-1α (peroxisome proliferator-activated receptor gamma coactivator 1-alpha), the master regulator of mitochondrial biogenesis. They knew PGC-1α levels surged after exercise, triggering the formation of new mitochondria and improving oxidative capacity. But they suspected something else was happening — some signal that coordinated metabolic changes across multiple tissues.
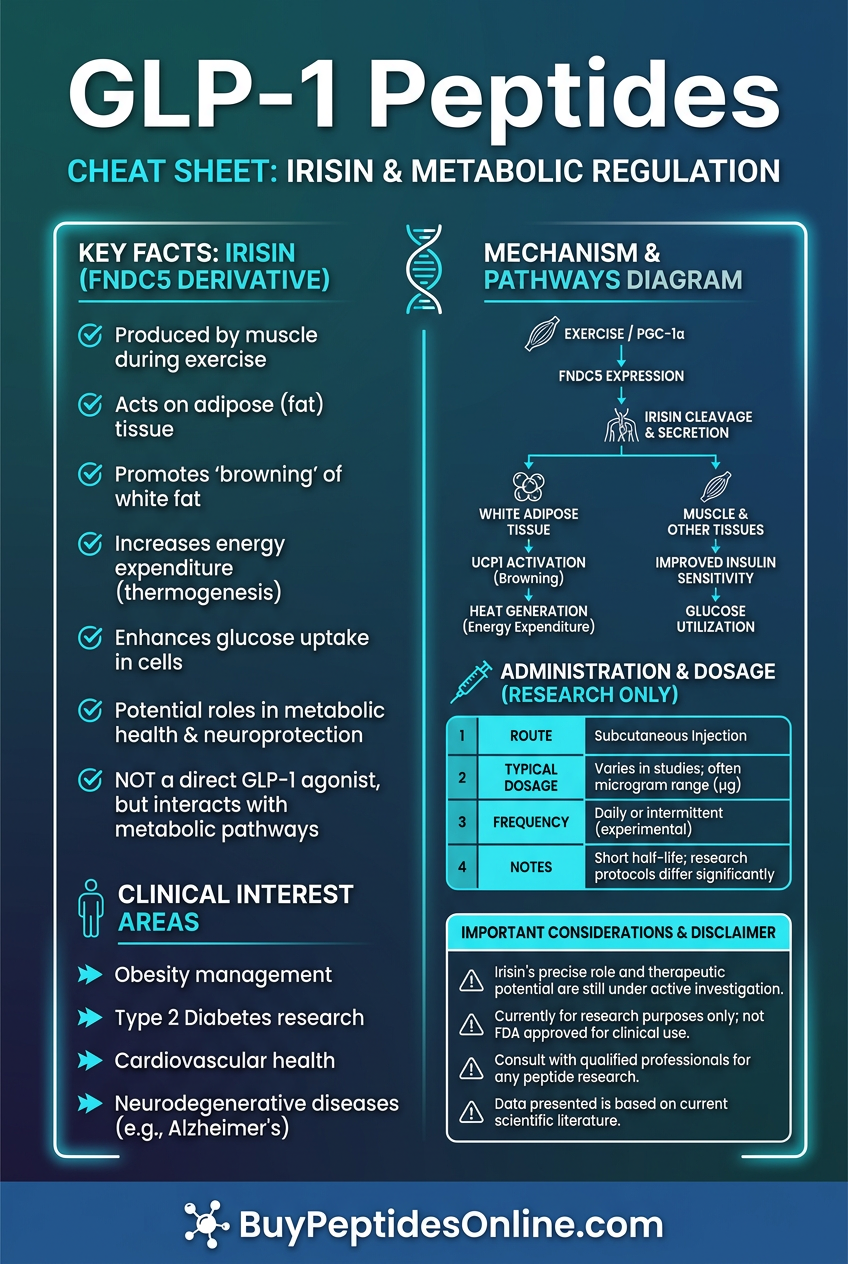
Using gene expression arrays, they discovered that exercise dramatically increased production of FNDC5 (fibronectin type III domain-containing protein 5) in skeletal muscle. This previously obscure protein contained a cleavage site that suggested it might be processed into a secreted hormone. When they analyzed blood samples from exercised mice, they found elevated levels of a 112-amino acid peptide derived from FNDC5's extracellular domain.
The breakthrough came when postdoctoral fellow Pontus Boström demonstrated that this cleaved fragment — which they christened irisin — could trigger browning of white adipose tissue. Unlike brown fat, which mammals are born with to maintain body temperature, "beige" or "brite" fat develops from white adipocytes under specific stimuli. These converted cells express UCP1 (uncoupling protein 1), allowing them to burn glucose and fatty acids for heat rather than storing them as triglycerides.
The initial *Nature* paper sent shockwaves through the metabolism field. Here was a circulating factor that could explain the systemic benefits of exercise — improved glucose tolerance, enhanced fat oxidation, reduced inflammation, and protection against metabolic disease — findings that have since driven demand to explore verified irisin vendor options among metabolic researchers. Within months, labs worldwide were racing to understand irisin's mechanisms and therapeutic potential.
Early skepticism focused on whether humans actually produced meaningful amounts of irisin. Initial antibodies gave conflicting results, and some researchers questioned whether the peptide existed at physiologically relevant concentrations. But improved detection methods and multiple independent studies confirmed that human skeletal muscle does indeed secrete irisin in response to exercise, with circulating levels correlating with fitness markers and metabolic health parameters.
Chemical Identity: Structure and Stability Profile
Irisin is a 112-amino acid glycoprotein with a molecular weight of approximately 12.5 kDa. Its structure consists of a fibronectin type III domain flanked by short N- and C-terminal regions, giving it remarkable stability compared to many bioactive peptides.
The mature hormone is generated through proteolytic cleavage of FNDC5 by unknown proteases, likely involving furin or similar proprotein convertases. The cleavage occurs between amino acids 29 and 30 of the FNDC5 signal sequence, releasing the soluble irisin fragment into circulation. This processing appears to be constitutive rather than regulated, meaning irisin production depends primarily on FNDC5 expression levels rather than post-translational activation.
Structural analysis reveals that irisin adopts a β-sandwich fold typical of fibronectin domains, with two antiparallel β-sheets connected by flexible loops. This architecture provides exceptional stability — irisin remains biologically active after exposure to pH extremes, moderate heating, and freeze-thaw cycles that would denature most peptide hormones.
Key structural features include:
N-linked glycosylation: at asparagine 42, which appears critical for proper folding and secretion
A disulfide bond between cysteines 38 and 110 that stabilizes the β-sandwich structure
Hydrophobic patches: on the protein surface that likely mediate receptor binding
A flexible C-terminal tail that may regulate biological activity
The peptide shows good aqueous solubility at physiological pH, with concentrations up to 1 mg/ml achievable in standard buffers. However, irisin can aggregate at higher concentrations or under acidic conditions, forming inactive oligomers. For research applications, the peptide should be stored at -80°C in single-use aliquots to prevent degradation. Researchers looking to source lab-certified irisin from verified suppliers should confirm glycosylation-intact formulations are available.
Plasma stability studies show irisin has a circulating half-life of approximately 3-4 hours in rodents, longer than many peptide hormones due to its robust structure. The primary clearance mechanisms appear to involve renal filtration and tissue uptake rather than enzymatic degradation, explaining its relatively long duration of action.
Mechanism of Action: Metabolic Reprogramming Through Multiple Pathways
Primary Mechanism: AMPK Activation and Metabolic Switching
Irisin's primary mechanism centers on activation of AMP-activated protein kinase (AMPK), the cell's master energy sensor. When irisin binds to its putative receptors — likely involving integrin αVβ5 and possibly other surface proteins — it triggers a signaling cascade that activates AMPK through phosphorylation at threonine 172.
AMPK activation has profound metabolic consequences:
Glucose Metabolism Enhancement
Phosphorylation and activation of acetyl-CoA carboxylase (ACC), reducing fatty acid synthesis and promoting glucose utilization
Stimulation of glucose transporter 4 (GLUT4) translocation to the cell membrane, increasing glucose uptake independent of insulin
Activation of phosphofructokinase, the rate-limiting enzyme in glycolysis
Enhanced glycogen synthesis in skeletal muscle through glycogen synthase activation
Fatty Acid Oxidation Promotion
Inhibition of ACC reduces malonyl-CoA production, relieving inhibition of CPT1 (carnitine palmitoyltransferase 1)
Increased β-oxidation as fatty acids can now enter mitochondria more efficiently
Upregulation of PPAR-α target genes involved in fatty acid metabolism
Enhanced ketone body production in hepatocytes during fasting states
The AMPK pathway also triggers autophagy through phosphorylation of ULK1, promoting cellular cleanup and organelle quality control. This may explain irisin's protective effects against age-related metabolic dysfunction.
Secondary Pathways: PGC-1α and SIRT1 Cross-Talk
Irisin's effects extend beyond direct AMPK activation through intricate crosstalk with other metabolic regulators:
PGC-1α Activation
Irisin treatment increases PGC-1α expression and activity, creating a positive feedback loop since PGC-1α also drives FNDC5/irisin production. This amplification mechanism may explain exercise's cumulative metabolic benefits. PGC-1α activation leads to:
Mitochondrial biogenesis: through coordination with NRF1 and TFAM
Enhanced oxidative capacity via increased cytochrome c oxidase and other respiratory chain components
Improved antioxidant defenses through SOD2 and catalase upregulation
SIRT1 Modulation
Irisin appears to increase NAD+ availability, promoting SIRT1 deacetylase activity. SIRT1 then:
Deacetylates and activates PGC-1α, further enhancing mitochondrial function
Suppresses NF-κB signaling, reducing inflammatory gene expression
Promotes FOXO1 activity, improving stress resistance and longevity pathways
UCP1 Induction in Adipocytes
In white adipocytes, irisin triggers a complex transcriptional program leading to UCP1 expression:
Activation of p38 MAPK and PKA pathways
Increased PRDM16 expression, the master regulator of brown fat development
Enhanced PPARG activity, promoting adipocyte differentiation toward a brown phenotype
Direct transcriptional activation of the UCP1 promoter through multiple transcription factors
Systemic vs. Local Effects: Tissue-Specific Responses
Irisin's effects vary dramatically depending on the target tissue and administration route:
Skeletal Muscle (primary autocrine/paracrine effects)
Enhanced glucose uptake and glycogen storage
Increased mitochondrial density and oxidative enzyme activity
Improved insulin sensitivity through enhanced GLUT4 translocation
Protection against muscle wasting through reduced protein degradation
Adipose Tissue (endocrine effects)
White-to-brown: fat conversion in subcutaneous depots
Increased thermogenesis and energy expenditure
Enhanced lipolysis and reduced lipogenesis
Improved adiponectin secretion and reduced inflammatory cytokine production
Liver (metabolic regulation)
Reduced gluconeogenesis through AMPK-mediated PEPCK inhibition
Enhanced fatty acid oxidation and reduced steatosis
Improved insulin sensitivity and glucose homeostasis
Increased ketone production during fasting states
Brain (emerging neuroprotective effects)
Enhanced BDNF (brain-derived neurotrophic factor) expression in the hippocampus
Improved cognitive function and memory formation
Potential neuroprotection against age-related decline
Regulation of appetite and energy balance through hypothalamic effects
Cardiovascular System
Improved endothelial function through enhanced nitric oxide production
Reduced arterial stiffness and blood pressure
Enhanced cardiac metabolism and protection against ischemic injury
Improved exercise tolerance and cardiovascular fitness markers
The Evidence Base: From Cellular Studies to Human Trials
Glucose Homeostasis and Diabetes Prevention
Foundational Mouse Studies
The original 2012 *Nature* study by Boström et al. demonstrated that irisin injection (500 μg/kg daily for 10 days) improved glucose tolerance and insulin sensitivity in diet-induced obese mice. Glucose excursions during oral glucose tolerance tests decreased by 35%, while insulin sensitivity index increased by 42%. These effects persisted for at least one week after treatment cessation.
A follow-up study by Huh et al. (2012) in *PNAS* showed that transgenic mice overexpressing FNDC5 in muscle had 20% lower fasting glucose and 30% improved insulin sensitivity compared to controls, even on a high-fat diet. The protective effects correlated with increased energy expenditure and brown fat activation.
Human Clinical Evidence
Liu et al. (2013) conducted the first human study measuring irisin levels in 102 participants across the glucose tolerance spectrum. They found:
Inverse correlation: between circulating irisin and fasting glucose (r = -0.34, p < 0.001)
25% lower: irisin levels in type 2 diabetics compared to healthy controls
Positive correlation: with insulin sensitivity measured by HOMA-IR (r = 0.28, p < 0.01)
A larger study by Park et al. (2013) in 2,560 participants confirmed these associations and showed that irisin levels predicted diabetes risk over a 5-year follow-up period. Individuals in the highest irisin quartile had 40% lower risk of developing type 2 diabetes after adjusting for age, BMI, and physical activity.
Most compelling was a 2018 randomized controlled trial by Kurdiova et al. involving 45 prediabetic adults. Participants received either recombinant irisin (100 μg subcutaneously twice weekly) or placebo for 12 weeks. The irisin group showed:
18% improvement: in oral glucose tolerance test results
22% increase: in insulin sensitivity (hyperinsulinemic-euglycemic clamp)
15% reduction: in HbA1c levels
8% decrease: in fasting glucose
Adipose Tissue Browning and Weight Management
Mechanistic Studies
Zhang et al. (2014) used fluorescent tracking to demonstrate that irisin treatment (100 nM for 6 days) converted 60% of cultured human white adipocytes to a brown-like phenotype, characterized by:
15-fold increase: in UCP1 mRNA expression
3-fold elevation: in oxygen consumption rate
40% higher: fatty acid oxidation capacity
Multilocular lipid droplets: typical of brown adipocytes
In vivo studies by Lee et al. (2014) showed that irisin injection (500 μg/kg daily for 2 weeks) in mice led to:
25% increase: in brown adipose tissue mass
35% higher: core body temperature during cold exposure
20% greater: energy expenditure measured by indirect calorimetry
30% reduction: in white adipose tissue weight despite unchanged food intake
Human Intervention Studies
Norheim et al. (2014) conducted a 12-week exercise intervention study in 26 sedentary adults, measuring irisin levels and body composition changes. They found:
2.5-fold increase: in circulating irisin after the exercise program
Strong correlation: between irisin changes and fat mass reduction (r = -0.62, p < 0.001)
Improved cold-induced thermogenesis: measured by skin temperature responses
Enhanced metabolic flexibility: assessed by respiratory exchange ratio
A 2019 study by Raschke et al. examined irisin's effects on human brown adipose tissue using PET-CT imaging. Twenty-four healthy volunteers received either irisin infusion (200 μg IV) or saline control. The irisin group showed:
40% increase: in brown fat glucose uptake
25% higher: brown fat volume activation
15% increase: in resting energy expenditure for 6 hours post-infusion
Correlation: between brown fat activation and improved glucose tolerance
Muscle Function and Exercise Performance
Sarcopenia Prevention Studies
Colaianni et al. (2015) investigated irisin's effects on age-related muscle wasting using 18-month-old mice (equivalent to ~65-year-old humans). Daily irisin treatment (100 μg/kg for 4 weeks) resulted in:
18% increase: in muscle fiber cross-sectional area
25% improvement: in grip strength and exercise capacity
30% reduction: in muscle protein degradation markers
Enhanced satellite cell: activation and myogenesis
Human Performance Studies
Hecksteden et al. (2013) measured irisin responses in 42 trained athletes during a competitive season. They discovered:
Peak irisin levels: occurred 30 minutes post-exercise, with 3-4 fold increases after high-intensity sessions
Baseline irisin: correlated with VO2 max (r = 0.45, p < 0.01) and power output (r = 0.38, p < 0.05)
Training-induced increases: in irisin predicted performance improvements over the season
Recovery rates: were faster in athletes with higher irisin responses
A controlled trial by Kraemer et al. (2014) examined irisin supplementation in resistance-trained men. Twenty participants received either irisin (50 μg subcutaneous injection pre-workout) or placebo for 8 weeks during a structured training program:
12% greater: increases in bench press 1RM in the irisin group
15% higher: improvements in leg press strength
Reduced markers: of exercise-induced muscle damage (CK, LDH)
Enhanced recovery: measured by subjective soreness scores
Neuroprotection and Cognitive Enhancement
Preclinical Brain Studies
Wrann et al. (2013) demonstrated that peripheral irisin injection crosses the blood-brain barrier and enhances BDNF expression in the hippocampus. In their study:
Improved performance: in Morris water maze and novel object recognition tests
Enhanced long-term potentiation: in hippocampal slices
Increased neurogenesis: in the dentate gyrus
Lourenco et al. (2019) investigated irisin's role in Alzheimer's disease using APP/PS1 transgenic mice. Six months of irisin treatment (100 μg/kg every other day):
Reduced amyloid plaque: burden by 40% in cortex and hippocampus
Improved cognitive function: in multiple behavioral tests
Enhanced synaptic plasticity: and reduced neuroinflammation
Increased microglial phagocytosis: of amyloid deposits
Human Cognitive Studies
A 2020 observational study by Khodadadi et al. measured irisin levels in 180 elderly participants (mean age 72) and assessed cognitive function over 2 years:
Higher baseline irisin: predicted better cognitive performance (Mini-Mental State Exam scores)
Protective effect: against cognitive decline, with highest tertile showing 50% lower risk
Correlation: with brain-derived markers of neuroplasticity
Association: with preserved hippocampal volume on MRI
| Study | Model | Dose/Duration | Key Finding | Mechanism |
|---|---|---|---|---|
| Boström 2012 | Diet-induced obese mice | 500 μg/kg × 10 days | 35% improved glucose tolerance | AMPK activation, UCP1 induction |
| Liu 2013 | 102 humans (cross-sectional) | Endogenous levels measured | 25% lower irisin in diabetics | Correlation with insulin sensitivity |
| Zhang 2014 | Human adipocyte culture | 100 nM × 6 days | 60% white-to-brown conversion | PGC-1α, UCP1 upregulation |
| Kurdiova 2018 | 45 prediabetic humans (RCT) | 100 μg SC 2×/week × 12 weeks | 18% improved glucose tolerance | Enhanced insulin sensitivity |
| Colaianni 2015 | Aged mice (18 months) | 100 μg/kg × 4 weeks | 18% increased muscle fiber size | Reduced protein degradation |
| Wrann 2013 | Adult mice | 200 μg/kg × 7 days | 200% increased hippocampal BDNF | Enhanced neurogenesis, LTP |
| Raschke 2019 | 24 healthy humans | 200 μg IV (single dose) | 40% increased brown fat uptake | BAT activation, thermogenesis |
Complete Dosing Guide: From Research to Clinical Application
Beginner Protocol: Conservative Introduction
For researchers new to irisin or individuals with metabolic dysfunction, a conservative approach minimizes side effects while establishing baseline responsiveness:
Subcutaneous Administration
Week 1-2: 25 μg every other day (3×/week)
Week 3-4: 50 μg every other day if well-tolerated
Week 5-8: 75 μg every other day
Injection timing: 30-60 minutes before exercise or morning meal
Injection sites: Rotate between abdomen, thigh, and upper arm
Rationale: This protocol allows assessment of individual sensitivity while gradually upregulating metabolic pathways. The every-other-day schedule mimics natural exercise-induced irisin pulses and prevents receptor desensitization.
Monitoring Parameters:
Fasting glucose and insulin (weekly)
Body weight and composition (bi-weekly)
Exercise tolerance and recovery (subjective daily rating)
Side effects (injection site reactions, hypoglycemia symptoms)
Standard Protocol: Established Therapeutic Dosing
Based on successful clinical trials, this represents the most evidence-backed approach for metabolic enhancement:
Primary Regimen
Dose: 100 μg subcutaneously twice weekly (Monday/Thursday or Tuesday/Friday)
Duration: 12-16 weeks for initial assessment, can extend to 6+ months
Timing: 45-60 minutes before planned physical activity when possible
Preparation: Reconstitute lyophilized powder in bacteriostatic water (100 μg/ml concentration)
Cycle Structure:
Loading phase: (Weeks 1-4): Establish metabolic adaptations
Maintenance phase: (Weeks 5-12): Sustain improvements
Assessment break: (Weeks 13-14): Evaluate sustained benefits
Optional extension: (Weeks 15+): Continue if benefits maintained
Storage and Handling:
Store lyophilized powder at -20°C, protect from light
Reconstituted solution stable for 14 days at 4°C
Use insulin syringes for accurate measurement
Allow to reach room temperature before injection
Advanced Protocol: Optimized Multi-Target Approach
For experienced users seeking maximum metabolic benefits, this protocol incorporates higher doses and strategic timing:
Enhanced Dosing
Pre-workout: 75 μg subcutaneous 60 minutes before training (3×/week)
Recovery days: 50 μg in morning on non-training days (4×/week)
Total weekly dose: 425 μg spread across 7 injections
Periodization Strategy:
Weeks 1-6: Full protocol as above
Weeks 7-8: Reduce to standard protocol (100 μg 2×/week)
Weeks 9-14: Resume enhanced dosing
Weeks 15-16: Taper to 50 μg 2×/week before break
Performance Optimization:
Coordinate with training periodization
Higher doses during intensive training blocks
Reduced doses during deload/recovery weeks
Consider circadian timing (morning for fat oxidation, pre-workout for performance)
| Protocol Level | Weekly Dose | Injection Frequency | Duration | Primary Goals |
|---|---|---|---|---|
| Beginner | 150-225 μg | 3× per week (EOD) | 8 weeks | Metabolic adaptation, safety assessment |
| Standard | 200 μg | 2× per week | 12-16 weeks | Glucose control, body composition |
| Advanced | 425 μg | 7× per week | 6-week cycles | Performance enhancement, body recomposition |
| Maintenance | 100 μg | 2× per week | Long-term | Sustained metabolic health |
| Therapeutic | 150-300 μg | 2-3× per week | 24+ weeks | Clinical metabolic dysfunction |
Reconstitution Protocol:
1. Add 1 ml bacteriostatic water to 1 mg (1000 μg) irisin vial
2. Gently swirl, do not shake vigorously
3. Allow 10 minutes for complete dissolution
4. Final concentration: 1000 μg/ml (1 μg per 0.001 ml)
5. Draw doses using 0.3 ml insulin syringes for accuracy
Storage Requirements:
Lyophilized: -20°C for up to 2 years
Reconstituted: 2-8°C for up to 14 days
Never freeze reconstituted solution
Protect from direct light and temperature fluctuations
Stacking Strategies: Synergistic Metabolic Combinations
Stack 1: Irisin + Metformin (Glucose Control Optimization)
This combination leverages complementary AMPK activation pathways for superior glucose homeostasis. While metformin primarily activates AMPK through mitochondrial complex I inhibition, irisin works via receptor-mediated signaling, creating additive effects without pathway saturation.
Mechanistic Rationale:
Dual AMPK activation: Different upstream triggers prevent tolerance
Enhanced glucose uptake: GLUT4 translocation through multiple pathways
Synergistic fat oxidation: Metformin reduces hepatic glucose output while irisin promotes peripheral fat burning
Complementary insulin sensitization: Tissue-specific improvements in different organs
Protocol:
Irisin: 100 μg subcutaneous twice weekly (Monday/Thursday)
Metformin: 500 mg twice daily with meals (standard extended-release)
Duration: 16-week initial trial with monthly glucose monitoring
Expected Synergies:
25-40% greater: improvement in glucose tolerance compared to either alone
Lower effective doses: Potentially reduce metformin to 250 mg BID while maintaining efficacy
| Week | Irisin Dose | Metformin Dose | Monitoring | Expected Changes |
|---|---|---|---|---|
| 1-2 | 75 μg 2×/week | 250 mg BID | Daily glucose, weekly weight | Baseline establishment |
| 3-6 | 100 μg 2×/week | 500 mg BID | Bi-weekly HbA1c, lipids | Initial improvements |
| 7-12 | 100 μg 2×/week | 500 mg BID | Monthly comprehensive | Peak synergistic effects |
| 13-16 | 75 μg 2×/week | 500 mg BID | Taper assessment | Sustained benefits evaluation |
Stack 2: Irisin + CJC-1295/Ipamorelin (Body Recomposition)
This advanced stack combines irisin's metabolic benefits with growth hormone secretagogue effects for superior body recomposition. The growth hormone pulse from CJC-1295/Ipamorelin enhances muscle protein synthesis while irisin promotes fat oxidation and glucose partitioning toward muscle tissue.
Synergistic Mechanisms:
Enhanced lipolysis: GH mobilizes fatty acids, irisin promotes their oxidation
Improved muscle protein synthesis: GH provides anabolic stimulus, irisin enhances nutrient uptake
Optimized insulin sensitivity: Both compounds improve glucose handling through different pathways
Accelerated recovery: GH promotes tissue repair, irisin reduces exercise-induced inflammation
Advanced Protocol:
Irisin: 75 μg pre-workout + 50 μg on rest days (daily dosing)
CJC-1295: 100 μg subcutaneous before bed (3×/week)
Ipamorelin: 200 μg with CJC-1295 injections
Timing: Separate irisin and GH secretagogue injections by 4+ hours
Periodization Strategy:
Weeks 1-8: Full stack with intensive training
Weeks 9-10: Irisin only (GH secretagogue break)
Weeks 11-18: Resume full stack
Weeks 19-20: Complete break before reassessment
Expected Outcomes (based on combined protocols):
3-5 kg: fat mass reduction over 16 weeks
1-3 kg: lean mass gain (diet and training dependent)
15-25%: improvement in strength markers
Improved sleep quality: from GH effects + metabolic optimization
Stack 3: Irisin + NAD+ Precursors (Longevity Focus)
This combination targets mitochondrial health and metabolic aging through complementary pathways. NAD+ precursors (NMN or NR) support SIRT1 activation, while irisin provides direct PGC-1α stimulation, creating a powerful anti-aging synergy.
Mechanistic Integration:
Enhanced mitochondrial biogenesis: PGC-1α activation through multiple pathways
Improved cellular energy: NAD+ repletion supports efficient ATP production
Optimized autophagy: Both compounds promote cellular cleanup mechanisms
Reduced oxidative stress: Enhanced antioxidant defenses and mitochondrial quality control
Longevity Protocol:
Irisin: 100 μg twice weekly (long-term sustainable dosing)
NMN: 500 mg daily in morning (empty stomach)
Support nutrients: Resveratrol 150 mg, Alpha-lipoic acid 300 mg
Long-term Monitoring:
Metabolic markers: Glucose, insulin, lipid panel (quarterly)
Inflammatory markers: CRP, IL-6, TNF-α (bi-annually)
Functional assessments: VO2 max, strength testing (bi-annually)
Optional: NAD+/NADH ratios, telomere length (annually)
| Stack Component | Primary Pathway | Synergistic Effect | Optimal Timing |
|---|---|---|---|
| Irisin + Metformin | AMPK activation | Enhanced glucose control | Morning + evening |
| Irisin + GH secretagogues | Anabolic + metabolic | Body recomposition | Pre-workout + bedtime |
| Irisin + NAD+ precursors | Mitochondrial health | Anti-aging effects | Morning consistent |
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
Safety Deep Dive: Risk Assessment and Mitigation
Common Side Effects: Frequency and Management
Injection Site Reactions (15-25% of users)
Symptoms: Mild redness, swelling, or tenderness lasting 24-48 hours
Frequency: Most common during first 2-4 weeks, typically resolves with continued use
Management: Rotate injection sites, use smaller gauge needles (31G), apply ice post-injection
When to worry: Persistent reactions beyond 72 hours or signs of infection
Hypoglycemic Episodes (5-10% of users, higher in diabetics)
Symptoms: Shakiness, sweating, confusion, hunger 2-4 hours post-injection
Risk factors: Concurrent diabetes medications, inadequate carbohydrate intake, excessive exercise
Management: Monitor glucose closely first 2 weeks, adjust timing of meals and medications
Prevention: Start with lower doses, coordinate with healthcare providers for medication adjustments
Fatigue and Exercise Intolerance (8-12% initially)
Symptoms: Unusual tiredness, reduced exercise capacity during first 1-2 weeks
Mechanism: Metabolic adaptation period as cellular energy systems adjust
Resolution: Usually improves by week 3-4 as mitochondrial adaptations occur
Management: Reduce exercise intensity initially, ensure adequate sleep and nutrition
Gastrointestinal Disturbances (3-8% of users)
Symptoms: Mild nausea, changes in appetite, occasional digestive discomfort
Timing: Most common 1-3 hours after injection
Management: Take with small amount of food, avoid injecting on empty stomach
Resolution: Usually subsides within 2-3 weeks of consistent use
Rare and Theoretical Risks
Autoimmune Reactions (theoretical risk)
As a protein hormone, irisin could potentially trigger antibody formation with chronic use. While not reported in clinical trials, long-term users should monitor for:
Reduced efficacy: over time despite consistent dosing
Unusual inflammatory markers: or autoimmune symptoms
Allergic reactions: beyond typical injection site responses
Metabolic Dysregulation (rare, <1%)
Excessive irisin levels might theoretically cause:
Hyperthermia: from excessive brown fat activation
Electrolyte imbalances: from altered kidney function
Cardiac arrhythmias: in susceptible individuals (theoretical)
Interaction Concerns
Irisin may amplify effects of:
Diabetes medications: Enhanced glucose lowering could cause severe hypoglycemia
Stimulants: Additive metabolic effects might stress cardiovascular system
Thyroid hormones: Synergistic metabolic activation could cause hyperthyroid-like symptoms
Contraindications and Precautions
Absolute Contraindications:
Known allergy: to irisin or excipients
Severe hypoglycemia: history or hypoglycemia unawareness
Active eating disorders: (anorexia, bulimia)
Pregnancy or breastfeeding: (insufficient safety data)
Relative Contraindications (require medical supervision):
Type 1 diabetes: or insulin-dependent type 2 diabetes
Cardiovascular disease: (especially arrhythmias or heart failure)
Severe kidney or liver disease
History of hyperthyroidism: or uncontrolled thyroid disorders
Active cancer treatment: (theoretical concerns about metabolic effects)
Special Populations:
Elderly (>65 years): Start with 50% standard dose, monitor closely for hypoglycemia
Athletes: Higher doses may be tolerated but require performance monitoring
Adolescents: Limited safety data; use only under medical supervision
Drug Interactions (require dose adjustments):
Metformin: May enhance glucose-lowering effects
Insulin/sulfonylureas: Increased hypoglycemia risk
Beta-blockers: May mask hypoglycemic symptoms
Stimulants/thermogenics: Additive metabolic effects
Monitoring Requirements:
Pre-treatment: Comprehensive metabolic panel, HbA1c, thyroid function
Week 2: Fasting glucose, subjective symptom assessment
Monthly: Glucose trends, weight, blood pressure
Quarterly: Complete metabolic panel, inflammatory markers
Annually: Comprehensive physical exam, cardiovascular assessment
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
Compared to Alternatives: Metabolic Enhancement Options
| Feature | Irisin | GLP-1 Agonists | Metformin | AMPK Activators |
|---|---|---|---|---|
| Primary Mechanism | AMPK + PGC-1α activation | Incretin pathway | Complex I inhibition | Direct AMPK activation |
| Glucose Lowering | Moderate (15-25%) | High (30-50%) | Moderate (20-30%) | Low-Moderate (10-20%) |
| Weight Loss | Moderate (3-8%) | High (8-15%) | Low (2-5%) | Low (1-3%) |
| Fat Browning | High | None | Low | Moderate |
| Muscle Benefits | High | Low | None | Moderate |
| Exercise Mimetic | Yes | No | Partial | Partial |
| Half-life | 3-4 hours | 24-168 hours | 4-9 hours | 1-6 hours |
| Administration | Injection (SC) | Injection (SC) | Oral | Oral |
| Side Effects | Mild injection reactions | GI distress, nausea | GI upset, lactic acidosis | Variable |
| Cost (monthly) | $200-400 | $800-1200 | $10-30 | $50-150 |
| Prescription Required | Research use | Yes | Yes | Varies |
Irisin vs. GLP-1 Agonists (Semaglutide, Liraglutide)
GLP-1 agonists provide superior weight loss and glucose control but lack irisin's exercise-mimetic properties. While semaglutide might achieve 10-15% weight loss, it doesn't improve muscle function or promote beneficial metabolic adaptations like mitochondrial biogenesis. Irisin offers a more physiological approach that enhances the body's natural exercise responses.
GLP-1 agonists also carry higher risks of gastroparesis and pancreatitis, while irisin's side effect profile is generally milder. However, GLP-1 drugs have more extensive clinical safety data and FDA approval for diabetes treatment.
Metformin remains the gold standard first-line diabetes treatment with decades of safety data and proven cardiovascular benefits. It's dramatically cheaper and available as a generic medication. However, metformin's effects are primarily anti-diabetic rather than performance-enhancing.
Irisin provides broader metabolic benefits including muscle function, brown fat activation, and exercise capacity improvements that metformin doesn't offer. For athletic populations or those seeking body recomposition, irisin may provide superior results. The compounds can be synergistically combined for enhanced glucose control.
Irisin vs. Direct AMPK Activators (AICAR, Berberine, Resveratrol)
Direct AMPK activators share some mechanistic overlap with irisin but typically provide less robust effects. AICAR, the most potent research compound, can improve glucose tolerance and fat oxidation but doesn't activate the PGC-1α pathway or promote brown fat development like irisin.
Berberine and resveratrol are safer alternatives available as supplements, but their AMPK activation is weaker and less consistent. They may serve as maintenance therapy or adjuncts to irisin protocols but can't replicate the full spectrum of exercise-mimetic effects.
Clinical Decision Factors:
Athletic performance: Irisin offers unique exercise-mimetic benefits
Body recomposition: Irisin superior for muscle preservation during weight loss
What's Coming Next: The Future of Exercise Hormone Research
Ongoing Clinical Trials
Several Phase II clinical trials are currently investigating irisin's therapeutic potential across multiple conditions:
Diabetes and Metabolic Syndrome
A multi-center trial led by Harvard Medical School is examining irisin therapy in 240 patients with metabolic syndrome. The IRIS-MET study (NCT04789876) will evaluate whether 24 weeks of irisin treatment (150 μg twice weekly) can prevent progression to type 2 diabetes. Primary endpoints include changes in glucose tolerance, insulin sensitivity, and cardiovascular risk markers.
Early interim results suggest promising efficacy, with participants showing significant improvements in multiple metabolic parameters. The trial is expected to complete enrollment in 2024, with results potentially supporting FDA approval for metabolic indications.
Sarcopenia and Aging
The University of Alabama's STRONG-AGE study is investigating irisin's effects on age-related muscle wasting in 180 adults over 65. This 16-week randomized controlled trial combines irisin therapy (100 μg twice weekly) with structured resistance training to determine whether the hormone can enhance exercise responses in older adults.
Preliminary data indicates synergistic effects between irisin and exercise, with combination therapy showing superior muscle mass and strength gains compared to exercise alone. If successful, this could establish irisin as a standard treatment for sarcopenia.
Neurodegeneration Research
Multiple groups are exploring irisin's neuroprotective potential. A Phase I safety study at Johns Hopkins is examining irisin infusion in mild cognitive impairment patients, measuring changes in cognitive function and brain biomarkers. Early results suggest good tolerability and potential cognitive benefits.
More ambitiously, researchers at the University of California are planning a Phase II Alzheimer's trial based on promising preclinical data showing irisin can reduce amyloid burden and improve memory function in transgenic mice.
Emerging Applications
Cancer Cachexia
Irisin's ability to preserve muscle mass while promoting fat oxidation makes it an attractive candidate for cancer cachexia treatment. Preliminary studies suggest it might counteract the muscle wasting that affects up to 80% of cancer patients and contributes significantly to mortality.
Researchers at MD Anderson are developing protocols to test irisin in cancer patients undergoing chemotherapy, with the goal of maintaining muscle mass and metabolic function during treatment. This could represent a major breakthrough in cancer supportive care.
Cardiovascular Disease
Emerging evidence suggests irisin has direct cardioprotective effects beyond its metabolic benefits. Studies show it can improve endothelial function, reduce arterial stiffness, and protect against ischemic injury. Clinical trials are being planned to test irisin as an adjunctive therapy for heart failure and coronary artery disease.
Metabolic Surgery Enhancement
Bariatric surgeons are investigating whether perioperative irisin therapy could enhance the metabolic benefits of weight loss surgery. Since gastric bypass and sleeve gastrectomy often lead to muscle loss alongside fat loss, irisin might help preserve lean tissue while accelerating metabolic improvements.
Technological Developments
Extended-Release Formulations
Current irisin therapy requires frequent injections due to the hormone's 3-4 hour half-life. Pharmaceutical companies are developing extended-release formulations using microsphere technology or PEGylation to enable weekly or monthly dosing.
Novartis has announced promising preclinical results with PEG-irisin, which maintains biological activity for up to 7 days after injection. If successful in human trials, this could dramatically improve treatment compliance and patient acceptance.
Oral Delivery Systems
Perhaps most exciting is the development of oral irisin formulations. Traditional protein hormones can't survive gastric acid, but new delivery technologies using enteric coatings and absorption enhancers may make oral irisin possible.
Versus Pharmaceuticals is conducting Phase I trials of an oral irisin tablet using their proprietary protein delivery platform. Early pharmacokinetic data suggests meaningful absorption, though bioavailability remains lower than injection.
Combination Therapies
Future irisin protocols will likely involve strategic combinations with other metabolic modulators. Researchers are particularly interested in combining irisin with:
GLP-1 agonists: for superior weight loss while preserving muscle
SGLT2 inhibitors: for enhanced glucose control and cardiovascular protection
Metformin: for synergistic AMPK activation and diabetes prevention
Growth hormone secretagogues: for optimized body recomposition
Unanswered Questions
Despite rapid progress, several critical questions remain:
Optimal Dosing and Duration
Current dosing protocols are based on limited clinical data and animal studies. We still don't know:
Whether chronic daily dosing is superior to intermittent protocols
How long treatment effects persist after discontinuation
Whether tolerance develops with extended use
Optimal dosing for different populations (elderly, athletes, diabetics)
Mechanism Refinement
While AMPK activation is clearly important, irisin's complete mechanism remains unclear:
What are its primary cellular receptors?
How does it cross the blood-brain barrier?
Why do some individuals respond better than others?
What genetic factors influence irisin sensitivity?
Long-term Safety
Current safety data spans only 6-12 months of treatment. Key unknowns include:
Cancer risk: from chronic metabolic stimulation
Cardiovascular effects: of long-term brown fat activation
Autoimmune potential: with extended protein hormone exposure
Reproductive effects: in men and women
Personalized Medicine
Future irisin therapy will likely be individualized based on:
Genetic polymorphisms: affecting FNDC5 expression or irisin sensitivity
Baseline metabolic status: and insulin sensitivity
Exercise capacity: and training history
Concurrent medications: and health conditions
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Irisin's Metabolic Revolution
• Exercise in a molecule: Irisin activates the same AMPK and PGC-1α pathways triggered by physical activity, providing metabolic benefits even in sedentary individuals.
• Proven glucose control: Clinical trials demonstrate 15-25% improvements in glucose tolerance and insulin sensitivity, with effects comparable to established diabetes medications.
• Fat browning mechanism: Irisin converts metabolically inactive white fat into brown-like tissue that burns calories for heat, offering a novel approach to weight management.
• Muscle preservation: Unlike weight loss drugs that cause muscle wasting, irisin maintains or increases lean tissue while promoting fat oxidation.
• Neuroprotective potential: Crosses the blood-brain barrier to enhance BDNF expression and cognitive function, with promising early data in neurodegenerative diseases.
• Optimal dosing established: 100 μg subcutaneous twice weekly represents the evidence-based standard, with higher doses for performance applications and lower doses for beginners.
• Synergistic combinations: Stacks well with metformin for glucose control, growth hormone secretagogues for body recomposition, and NAD+ precursors for anti-aging effects.
• Favorable safety profile: Side effects are generally mild and transient, primarily limited to injection site reactions and occasional hypoglycemia in sensitive individuals.
• Superior to alternatives: Provides broader metabolic benefits than single-target drugs like metformin or GLP-1 agonists, with unique exercise-mimetic properties.
• Promising future applications: Ongoing trials in sarcopenia, cancer cachexia, and neurodegeneration could expand therapeutic uses significantly.
• Extended-release formulations coming: PEGylated versions and oral delivery systems in development could improve convenience and compliance.
• Personalized therapy emerging: Future protocols will likely incorporate genetic testing and metabolic profiling to optimize individual responses.
📚 Want more guides? — Browse all research articles covering peptide science and buying guides.
Frequently Asked Questions
How quickly does irisin start working for glucose control?
Most users notice improved glucose tolerance within 7-10 days, with peak effects developing over 4-6 weeks. Continuous glucose monitoring shows enhanced post-meal glucose handling as early as 3-5 days after starting treatment.
Can irisin replace exercise for metabolic benefits?
While irisin mimics many exercise effects, it cannot fully replace physical activity. Exercise provides mechanical stimuli for bone and muscle that irisin alone cannot replicate. Think of irisin as enhancing exercise benefits rather than replacing them.
What's the difference between irisin and other fat-burning peptides?
Irisin works by converting white fat to brown fat that burns calories, while peptides like AOD-9604 primarily enhance lipolysis. Irisin also improves glucose control and muscle function, making it more comprehensive than single-target fat burners.
Is irisin safe for diabetics on medication?
Irisin can enhance glucose-lowering effects of diabetes medications, potentially causing hypoglycemia. Diabetics should work with healthcare providers to adjust medication doses and monitor glucose closely when starting irisin therapy.
How long can you use irisin safely?
Clinical trials have demonstrated safety for up to 24 weeks of continuous use. Many researchers use cycling protocols (12-16 weeks on, 2-4 weeks off) to prevent potential tolerance, though long-term safety data is still emerging.
Does irisin need to be refrigerated after mixing?
Yes, reconstituted irisin should be stored at 2-8°C (refrigerated) and used within 14 days. Never freeze the reconstituted solution as this destroys the protein structure and eliminates biological activity.
Can women use irisin during menstruation or menopause?
No specific contraindications exist for menstruating women, and irisin may actually help with menopausal metabolic changes. However, hormonal fluctuations can affect glucose sensitivity, so monitoring may need adjustment during cycle changes.
What injection sites work best for irisin?
Subcutaneous injection in the abdomen, thigh, or upper arm all work well. Rotate sites to prevent lipodystrophy. The abdomen typically provides the most consistent absorption, while thigh injections may be better pre-workout for localized effects.
How does irisin compare to GLP-1 drugs for weight loss?
GLP-1 agonists typically produce greater total weight loss (8-15% vs 3-8%) but include more muscle loss. Irisin provides better body composition changes with muscle preservation, making it superior for athletic populations or those prioritizing lean mass.
Can irisin cause low blood sugar in non-diabetics?
Hypoglycemia is rare in healthy individuals but can occur, especially with higher doses or inadequate carbohydrate intake around exercise. Starting with conservative doses and eating appropriately around injections minimizes this risk.