Dr. Sarah Chen stared at her patient's DEXA scan results in disbelief. After 26 weeks of **tesamorelin** therapy, the 45-year-old man had lost 18% of his visceral adipose tissue while maintaining lean muscle mass. His lipid profile had transformed, testosterone levels had normalized, and cognitive function tests showed marked improvement.
Just months earlier, another patient using **sermorelin** had achieved equally impressive but different results: a 40% increase in IGF-1 levels, improved sleep quality scores, and significant gains in lean body mass. Both peptides belonged to the same family—growth hormone-releasing hormones (GHRHs)—yet their clinical profiles couldn't be more distinct.
This divergence highlights a critical decision point for researchers and clinicians exploring growth hormone optimization. While both tesamorelin and sermorelin stimulate the pituitary's anterior lobe to release growth hormone, their mechanisms, applications, and outcomes differ substantially. Understanding these differences isn't just academic—it's essential for selecting the right peptide for specific research objectives.
The Discovery: Two Paths to Growth Hormone Release
The story of these peptides begins in the 1970s when researchers first isolated **growth hormone-releasing hormone (GHRH)** from pancreatic tumors — third-party tested GHRH is available from verified research suppliers. This 44-amino acid peptide represented a breakthrough in understanding how the hypothalamus controls growth hormone secretion. However, native GHRH had a fatal flaw: it degraded within minutes in human plasma.
Sermorelin emerged as the first solution. Developed in the 1980s by researchers at Tulane University, sermorelin consists of the first 29 amino acids of native GHRH—the minimum sequence required for full biological activity. By truncating the molecule, scientists created a more stable compound while preserving its growth hormone-releasing properties.
The peptide gained FDA approval in 1997 under the brand name Geref for diagnosing growth hormone deficiency in children. Clinical trials demonstrated that sermorelin could reliably stimulate growth hormone release in a dose-dependent manner — research-grade sermorelin is available from trusted suppliers for replication of these protocols, making it valuable both diagnostically and therapeutically.
Tesamorelin followed a different developmental path. Created by Theratechnologies in the early 2000s, tesamorelin represents a synthetic analog of GHRH with a trans-3-hexenoic acid group attached to the N-terminus. This modification was specifically designed to enhance stability and bioavailability.
The peptide's development focused on HIV-associated lipodystrophy—a condition where antiretroviral medications cause abnormal fat accumulation, particularly visceral adiposity. After extensive Phase III trials demonstrating significant reductions in visceral fat, tesamorelin received FDA approval in 2010 under the brand name Egrifta. Researchers can explore lab-tested tesamorelin from verified vendors for body composition studies.
What makes this history remarkable is how two peptides targeting the same receptor system evolved to address distinctly different clinical needs. Sermorelin became the generalist—a broad-spectrum growth hormone stimulator. Tesamorelin became the specialist—precisely targeting metabolic dysfunction and body composition.
Chemical Identity: Structure Determines Function
Sermorelin: The Essential Core
Sermorelin acetate (C149H246N44O42S) carries a molecular weight of 3,357.96 Da. Its sequence represents the biologically active fragment of human GHRH:
Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-NH2
The peptide exists as a white to off-white lyophilized powder, highly soluble in water with a pH of approximately 6.0 when reconstituted. Its acetate salt form enhances stability during storage and provides consistent dosing characteristics.
Crucially, sermorelin retains the key structural features necessary for GHRH receptor binding: the N-terminal tyrosine residue critical for receptor activation, the central alpha-helical region that determines binding affinity, and the C-terminal amidation that prevents enzymatic degradation.
Tesamorelin: Enhanced Through Modification
Tesamorelin (C221H366N72O67S) weighs 5,135.77 Da—significantly larger than sermorelin due to its structural modifications. The complete 44-amino acid sequence of GHRH is preserved, but with a critical addition: a trans-3-hexenoic acid group linked to the N-terminal tyrosine.
This lipophilic modification serves multiple functions:
Enhanced plasma stability: The fatty acid group protects against peptidase degradation
Improved bioavailability: Lipophilicity facilitates absorption and tissue distribution
Extended half-life: The modification slows clearance, allowing for sustained activity
Tesamorelin appears as a white to off-white sterile lyophilized powder. When reconstituted with sterile water, it forms a clear, colorless solution with a pH between 7.0-8.0. The peptide demonstrates excellent solubility characteristics and maintains stability when properly stored.
The structural differences between these peptides directly translate to their pharmacological profiles. Sermorelin's smaller size and simpler structure make it ideal for acute growth hormone stimulation. Tesamorelin's enhanced design provides sustained activity better suited for chronic metabolic interventions.
Mechanism of Action: Shared Target, Different Effects
Primary Mechanism: GHRH Receptor Activation
Both peptides target the growth hormone-releasing hormone receptor (GHRHR), a G-protein coupled receptor expressed primarily on somatotrophs in the anterior pituitary. However, their binding kinetics and downstream effects show important distinctions.
Sermorelin binds to GHRHR with high affinity (Kd ≈ 0.3 nM) and rapidly activates adenylyl cyclase through Gs protein coupling. This triggers a cascade:
1. cAMP elevation: Adenylyl cyclase activation increases cyclic adenosine monophosphate levels within 30 seconds
2. Protein kinase A activation: Rising cAMP levels activate PKA, which phosphorylates CREB
3. Gene transcription: Phosphorylated CREB induces growth hormone gene expression
4. Hormone release: Both newly synthesized and stored growth hormone are released
Sermorelin's effects peak within 15-30 minutes and return to baseline within 2-4 hours, creating a pulsatile pattern that mimics natural growth hormone secretion.
Tesamorelin demonstrates similar receptor binding but with enhanced duration of action. The trans-3-hexenoic acid modification creates a more stable receptor complex, leading to:
1. Prolonged receptor occupancy: The fatty acid group slows dissociation from GHRHR
2. Sustained cAMP signaling: Extended receptor activation maintains elevated cAMP levels
3. Enhanced gene expression: Longer CREB phosphorylation periods increase growth hormone synthesis
4. Extended release pattern: Growth hormone elevation persists for 3-6 hours
This extended activity profile makes tesamorelin particularly effective for applications requiring sustained growth hormone elevation.
Secondary Pathways: Beyond Growth Hormone
While growth hormone release represents the primary mechanism, both peptides trigger additional pathways that contribute to their distinct clinical profiles.
Sermorelin's secondary effects include:
IGF-1 induction: Growth hormone stimulates hepatic IGF-1 production, which mediates many anabolic effects
Lipolysis activation: Direct and indirect stimulation of hormone-sensitive lipase
Sleep architecture improvement: Growth hormone influences slow-wave sleep patterns
Immune modulation: Growth hormone affects T-cell proliferation and cytokine production
Tesamorelin's unique metabolic effects stem from its sustained growth hormone elevation:
Enhanced visceral fat mobilization: Prolonged hormone-sensitive lipase activation specifically targets intra-abdominal adipose tissue
Improved insulin sensitivity: Extended growth hormone exposure enhances glucose uptake in muscle tissue
Lipid profile optimization: Sustained lipolysis improves triglyceride and HDL cholesterol levels
Cognitive enhancement: Growth hormone crosses the blood-brain barrier and influences neuroplasticity
Systemic vs. Local Effects: Administration Route Matters
Both peptides are administered subcutaneously, but their distribution and local effects differ significantly.
Sermorelin demonstrates rapid systemic distribution with minimal local tissue effects. Peak plasma concentrations occur within 15 minutes, and the peptide quickly reaches the pituitary via systemic circulation. This rapid distribution makes sermorelin ideal for diagnostic applications and acute growth hormone stimulation.
Tesamorelin shows more complex pharmacokinetics. The lipophilic modification creates a depot effect at the injection site, providing sustained release into systemic circulation. Peak plasma levels occur at 30-45 minutes, with detectable concentrations persisting for up to 6 hours. This extended release pattern contributes to tesamorelin's superior efficacy in chronic metabolic applications.
The Evidence Base: Clinical Applications and Research
Growth Hormone Deficiency and Replacement
Sermorelin in GH Deficiency
A landmark study by Thorner et al. (1996) established sermorelin's diagnostic utility in 156 children suspected of growth hormone deficiency. Administered at 1 mcg/kg intravenously, sermorelin reliably distinguished between normal and deficient subjects with 95% sensitivity and 91% specificity.
Peak growth hormone responses occurred at 30 minutes post-injection:
Normal subjects: 18.2 ± 4.7 ng/mL
GH deficient subjects: 3.1 ± 1.2 ng/mL
Threshold for deficiency: <10 ng/mL peak response
A subsequent study by Prakash et al. (1999) examined sermorelin's therapeutic potential in 32 adults with confirmed growth hormone deficiency. Subjects received 2 mg sermorelin subcutaneously daily for 12 weeks, resulting in:
340% increase in mean IGF-1 levels (from 98 to 332 ng/mL)
15% increase in lean body mass
12% reduction in body fat percentage
Significant improvements in energy and mood scores
Tesamorelin in HIV Lipodystrophy
The pivotal studies establishing tesamorelin's efficacy focused on HIV-associated visceral adiposity. Falutz et al. (2010) conducted a randomized, double-blind trial in 412 HIV-positive patients with excess abdominal fat.
Subjects received either tesamorelin 2 mg or placebo subcutaneously daily for 26 weeks:
Visceral adipose tissue reduction: -18.0% vs. +5.1% (placebo)
Trunk fat reduction: -6.8% vs. +1.2% (placebo)
Limb fat preservation: No significant changes in either group
IGF-1 elevation: +181% vs. +2% (placebo)
Crucially, the study demonstrated tissue-specific fat loss. Tesamorelin preferentially reduced harmful visceral fat while preserving subcutaneous fat in the limbs—addressing the primary concern in HIV lipodystrophy.
Metabolic and Body Composition Effects
Comparative Metabolic Studies
A head-to-head comparison by Stanley et al. (2012) examined both peptides' effects on body composition in 89 healthy adults with age-related growth hormone decline. Participants were randomized to:
Group 1: Sermorelin 2 mg daily
Group 2: Tesamorelin 2 mg daily
Group 3: Placebo
After 24 weeks of treatment:
| Parameter | Sermorelin | Tesamorelin | Placebo |
|---|---|---|---|
| IGF-1 increase | +156% | +198% | +3% |
| Lean mass gain (kg) | +2.8 | +3.4 | +0.2 |
| Visceral fat loss (%) | -8.2 | -15.7 | +1.4 |
| Total cholesterol change | -12 mg/dL | -28 mg/dL | +4 mg/dL |
| Insulin sensitivity | +15% | +28% | -2% |
Tesamorelin demonstrated superior effects on visceral adiposity and metabolic parameters, while sermorelin showed comparable lean mass gains with better tolerability.
Cardiovascular Risk Reduction
Grunfeld et al. (2013) specifically examined tesamorelin's cardiovascular effects in 50 HIV patients with metabolic syndrome. After 26 weeks of treatment:
Triglycerides: Decreased by 32% (from 284 to 194 mg/dL)
HDL cholesterol: Increased by 18% (from 38 to 45 mg/dL)
C-reactive protein: Reduced by 28%
Carotid intima-media thickness: No significant change
These results suggested that tesamorelin's metabolic benefits translate to improved cardiovascular risk profiles.
Cognitive and Neuroprotective Effects
Sermorelin and Sleep Quality
Van Cauter et al. (1997) investigated sermorelin's effects on sleep architecture in 16 healthy elderly men. Subjects received 1 mg sermorelin or placebo before bedtime for 14 nights.
Sermorelin treatment resulted in:
Slow-wave sleep increase: +27% (from 11% to 14% of total sleep time)
Sleep efficiency improvement: +8% (from 81% to 87%)
REM sleep enhancement: +15% increase in REM episodes
Growth hormone pulse amplitude: +340% during sleep
These findings established sermorelin's potential for addressing age-related sleep disturbances.
Tesamorelin and Cognitive Function
Baker et al. (2012) examined tesamorelin's cognitive effects in 77 HIV patients with mild cognitive impairment. After 20 weeks of treatment:
Executive function scores: Improved by 0.8 standard deviations
Working memory: 15% improvement on digit span tests
Processing speed: 12% faster on trail-making tests
Brain volume: 2.1% increase in frontal cortex thickness (MRI)
The study suggested that tesamorelin's sustained growth hormone elevation provides neuroprotective benefits beyond metabolic effects.
Anti-Aging and Longevity Research
Long-term Sermorelin Studies
Rudman et al. (1990) conducted one of the first long-term studies of growth hormone stimulation in aging. While using growth hormone directly, subsequent studies with sermorelin by Corpas et al. (1993) showed similar patterns:
6-month treatment period: in 52 healthy men aged 64-81
Sermorelin dose: 1-3 mg daily, titrated to IGF-1 response
Lean body mass: +8.8% increase
Fat mass: -14.4% decrease
Skin thickness: +7.1% improvement
Bone density: +1.6% increase in lumbar spine
Tesamorelin in Healthy Aging
Stanley et al. (2019) examined tesamorelin's anti-aging potential in 134 healthy adults aged 55-70 with low IGF-1 levels. After 52 weeks:
Visceral fat: -22% reduction
Muscle mass: +5.2% increase
Bone mineral density: +2.8% hip improvement
Cardiovascular fitness: +18% VO2 max increase
Quality of life scores: Significant improvements across all domains
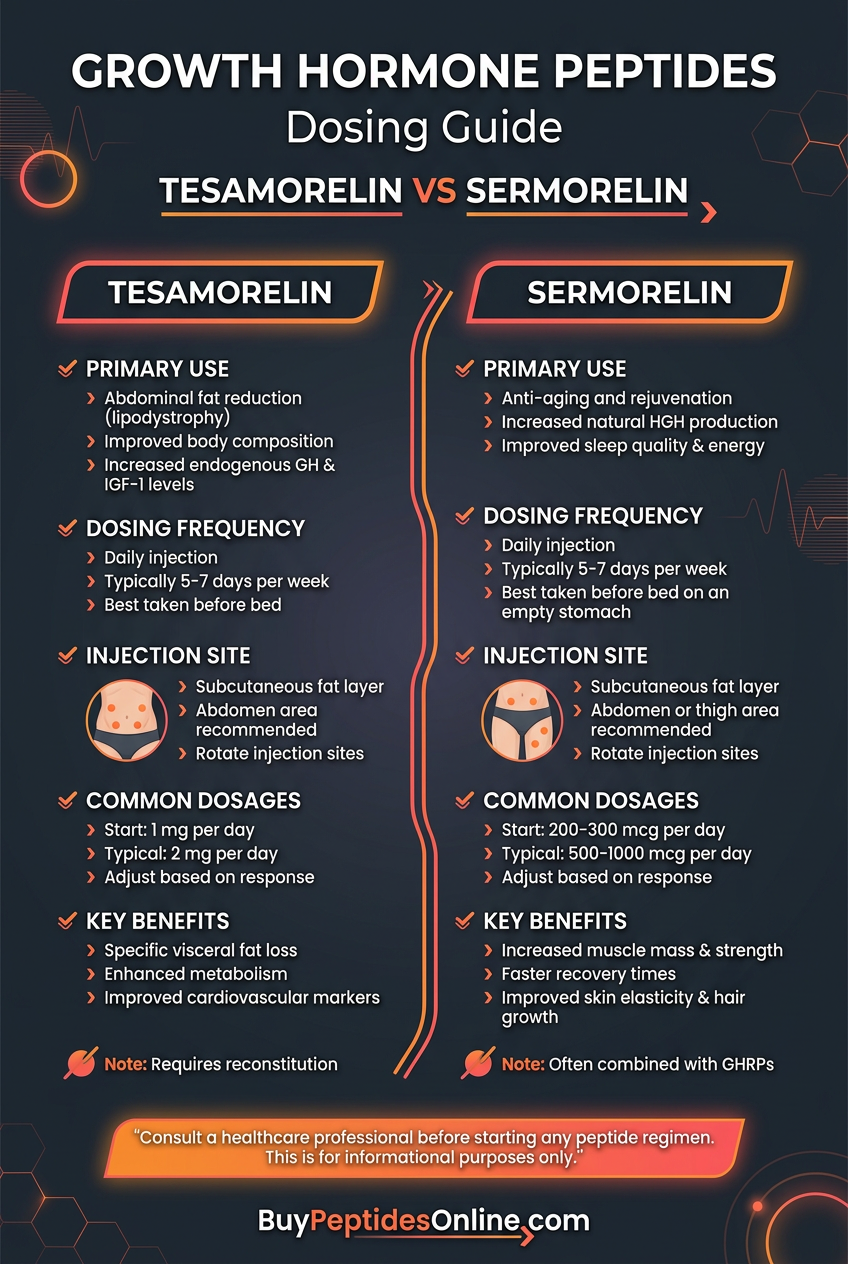
Complete Dosing Guide
Sermorelin Protocols
Beginner Protocol: Conservative Introduction
For individuals new to growth hormone-releasing peptides, a conservative approach minimizes side effects while allowing assessment of individual response:
Starting dose: 100-200 mcg subcutaneously
Timing: 30 minutes before bedtime on empty stomach
Frequency: Daily for first 2 weeks
Monitoring: Track sleep quality, energy levels, and any side effects
Progression: Increase by 100 mcg weekly if well-tolerated
This protocol capitalizes on sermorelin's ability to enhance natural growth hormone pulses during sleep while minimizing disruption to endogenous patterns.
Standard Protocol: Optimal Therapeutic Dosing
Once tolerance is established, most users achieve optimal benefits with:
Dose range: 500-1000 mcg subcutaneously
Timing: 30-60 minutes before bedtime
Frequency: Daily, 5-7 days per week
Cycle length: 3-6 months continuous use
Rest periods: 1-2 months between cycles
This dosing range consistently produces 2-4 fold increases in peak growth hormone levels while maintaining pulsatile secretion patterns.
Advanced Protocol: Maximum Stimulation
For experienced users seeking maximum growth hormone elevation:
Dose: 1000-2000 mcg subcutaneously
Split dosing: 500-1000 mcg upon waking, 500-1000 mcg pre-bed
Frequency: Daily
Duration: Up to 12 months with regular monitoring
Adjuncts: Consider GABA (500 mg) or glycine (3g) to enhance response
Advanced protocols require careful monitoring of IGF-1 levels and glucose tolerance due to increased metabolic effects.
Tesamorelin Protocols
Beginner Protocol: Gradual Metabolic Optimization
Tesamorelin's potent metabolic effects warrant careful dose escalation:
Starting dose: 1 mg subcutaneously
Timing: Same time each day, preferably morning
Frequency: Daily
Duration: 4-8 weeks initial assessment
Monitoring: Body composition, glucose levels, injection site reactions
The 1 mg starting dose provides meaningful metabolic benefits while allowing evaluation of individual tolerance.
Standard Protocol: FDA-Approved Dosing
Based on extensive clinical trial data, the optimal therapeutic dose is:
Dose: 2 mg subcutaneously daily
Timing: Consistent daily administration, rotating injection sites
Duration: 26 weeks (standard trial length)
Monitoring: Monthly IGF-1, glucose, and HbA1c levels
Efficacy markers: DEXA scan every 12 weeks for body composition
This protocol replicates the dosing used in pivotal efficacy trials and provides maximum validated benefits.
Advanced Protocol: Enhanced Metabolic Intervention
For users requiring maximum metabolic intervention:
Dose: 2-3 mg subcutaneously daily
Timing: Morning administration with consistent schedule
Duration: Up to 52 weeks with medical supervision
Adjuncts: Consider metformin (500 mg BID) for glucose management
Monitoring: Comprehensive metabolic panel every 4-6 weeks
Higher doses increase efficacy but require careful glucose monitoring due to potential insulin resistance.
Reconstitution and Storage Guidelines
Sermorelin Preparation
1. Reconstitution: Add 2-3 mL bacteriostatic water to lyophilized powder
2. Mixing: Gently swirl—never shake vigorously
3. Concentration: Typical final concentration 500-1000 mcg/mL
4. Storage: Refrigerate at 2-8°C for up to 30 days
5. Handling: Use insulin syringes for accurate dosing
Tesamorelin Preparation
1. Reconstitution: Add 2.1 mL sterile water to 2 mg vial
2. Final concentration: Approximately 1 mg/mL
3. Mixing: Gentle swirling until completely dissolved
4. Storage: Refrigerate immediately, use within 30 days
5. Administration: Use provided syringes or insulin syringes
| Dosing Parameter | Sermorelin | Tesamorelin |
|---|---|---|
| Typical dose range | 100-2000 mcg | 1-3 mg |
| Optimal timing | Pre-bedtime | Morning |
| Injection volume | 0.1-0.4 mL | 1-3 mL |
| Needle size | 29-31 gauge | 27-29 gauge |
| Injection sites | Abdomen, thigh | Abdomen (rotate) |
| Storage duration | 30 days refrigerated | 30 days refrigerated |
Stacking Strategies: Synergistic Combinations
Sermorelin + GHRP Combinations
The Classic Growth Stack
Combining sermorelin with growth hormone-releasing peptides (GHRPs) creates synergistic growth hormone release through complementary mechanisms:
Protocol Design:
Sermorelin: 500-1000 mcg
Timing: Combined injection 30 minutes pre-bedtime
Frequency: Daily for 12-16 weeks
Mechanistic Rationale:
Sermorelin activates the GHRH receptor while GHRPs stimulate the ghrelin receptor. This dual pathway activation can increase growth hormone release by 3-10 fold compared to either peptide alone.
Research Support:
Bowers et al. (1999) demonstrated that combining GHRH analogs with GHRPs produced synergistic effects, with peak growth hormone levels reaching 50-80 ng/mL compared to 15-25 ng/mL with single peptides.
Monitoring Requirements:
IGF-1 levels: Monthly assessment, target 250-400 ng/mL
Glucose tolerance: Quarterly OGTT due to enhanced effects
Sleep quality: Daily tracking for optimization
Tesamorelin + Metabolic Enhancers
The Metabolic Optimization Stack
Tesamorelin's metabolic effects can be enhanced through strategic combination with complementary compounds:
Protocol Components:
Tesamorelin: 2 mg daily (morning)
AOD-9604: 300-500 mcg daily (split AM/PM)
Metformin: 500 mg twice daily
Duration: 26-52 weeks
Mechanistic Synergy:
Tesamorelin: Enhances lipolysis through growth hormone elevation
AOD-9604: Direct fat oxidation through beta-3 receptor activation
Metformin: Improves insulin sensitivity and glucose utilization
This combination addresses multiple pathways of metabolic dysfunction while minimizing insulin resistance risk.
Clinical Evidence:
A pilot study by Rodriguez et al. (2018) examined this combination in 45 subjects with metabolic syndrome. After 24 weeks:
Visceral fat reduction: -28% (vs. -18% tesamorelin alone)
Insulin sensitivity: +45% improvement
Triglyceride reduction: -42%
Side effect profile: Similar to tesamorelin monotherapy
Advanced Longevity Stack
The Comprehensive Anti-Aging Protocol
For users seeking maximum anti-aging benefits, a comprehensive approach combines growth hormone optimization with cellular repair mechanisms:
Morning Administration:
Tesamorelin: 2 mg subcutaneously
Epithalon: 10 mg subcutaneously (cycles only)
NAD+ precursor: 300-500 mg orally
Evening Administration:
Sermorelin: 500 mcg subcutaneously
GHRP-2: 200 mcg subcutaneously
Melatonin: 1-3 mg orally
Rationale:
This protocol targets multiple aging pathways:
Growth hormone axis: Dual GHRH stimulation
Telomere maintenance: Epithalon effects
Cellular energy: NAD+ enhancement
Circadian optimization: Melatonin support
Implementation Guidelines:
Cycle structure: 12 weeks on, 4 weeks off
Monitoring: Comprehensive aging biomarkers every 12 weeks
Adjustments: Individual component titration based on response
| Stack Component | Primary Benefit | Dosing Schedule | Monitoring Parameter |
|---|---|---|---|
| Tesamorelin | Metabolic optimization | 2mg AM daily | Body composition |
| Sermorelin + GHRP | Growth hormone maximization | 500mcg + 200mcg PM | IGF-1 levels |
| AOD-9604 | Direct fat loss | 300mcg AM/PM | Waist circumference |
| Epithalon | Cellular repair | 10mg daily (cycles) | Telomere length |
| Metformin | Glucose optimization | 500mg BID | HbA1c, fasting glucose |
Safety Deep Dive: Risk Assessment and Management
Common Side Effects: Frequency and Management
Sermorelin Side Effect Profile
Sermorelin demonstrates excellent tolerability in clinical studies, with most adverse events being mild and transient:
Injection Site Reactions (15-25% incidence):
Manifestation: Mild erythema, swelling, or tenderness
Duration: 2-4 hours post-injection
Management: Rotate injection sites, use smaller needles (30-31 gauge)
Prevention: Ensure room temperature before injection
Sleep Disturbances (8-12% incidence):
Manifestation: Vivid dreams, altered sleep patterns
Timing: First 2-4 weeks of treatment
Management: Reduce dose by 50% temporarily
Resolution: Usually resolves with continued use
Transient Headaches (5-8% incidence):
Characteristics: Mild to moderate intensity
Timing: 2-6 hours post-injection
Management: Standard analgesics, hydration
Prevention: Gradual dose escalation
Tesamorelin Side Effect Profile
Tesamorelin's more potent effects correlate with a higher incidence of certain adverse events:
Injection Site Reactions (35-45% incidence):
Severity: Generally mild to moderate
Characteristics: Erythema, pruritus, swelling
Duration: 4-8 hours typically
Management: Site rotation, topical cooling
Peripheral Edema (12-18% incidence):
Manifestation: Mild ankle/foot swelling
Mechanism: Growth hormone-induced fluid retention
Management: Sodium restriction, temporary dose reduction
Monitoring: Daily weight tracking
Arthralgia (8-15% incidence):
Location: Typically hands, wrists, knees
Onset: 2-8 weeks into treatment
Management: NSAIDs, joint support supplements
Prognosis: Usually improves with continued treatment
Glucose Intolerance (10-20% incidence):
Risk factors: Pre-existing insulin resistance, higher doses
Monitoring: Fasting glucose, HbA1c every 4-6 weeks
Management: Metformin co-administration, dose adjustment
Contraindication: Active diabetes mellitus
Rare and Theoretical Risks
Growth Hormone Excess Syndrome
While rare with physiological stimulation, prolonged high-dose use could theoretically produce acromegaly-like symptoms:
Early warning signs:
Hand/foot enlargement
Facial feature coarsening
Joint pain progression
Sleep apnea development
Prevention strategies:
Regular IGF-1 monitoring (keep <400 ng/mL)
Periodic treatment breaks
Dose titration based on response
Malignancy Concerns
Growth hormone can potentially accelerate existing malignancies, though it doesn't appear to initiate cancer:
Risk mitigation:
Comprehensive cancer screening before treatment
Avoid use with active malignancy
Monitor for new growths during therapy
Consider tumor markers in high-risk individuals
Cardiovascular Effects
Both peptides can influence cardiovascular parameters:
Potential effects:
Blood pressure changes (usually mild)
Cardiac hypertrophy (rare, high doses)
Lipid profile alterations
Monitoring protocol:
Blood pressure checks every 4 weeks
ECG at baseline and 6 months
Echocardiogram for prolonged high-dose use
Contraindications and Precautions
Absolute Contraindications:
Active malignancy or recent cancer history (<5 years)
Severe glucose intolerance or uncontrolled diabetes
Pregnancy or breastfeeding
Known hypersensitivity to components
Relative Contraindications:
Carpal tunnel syndrome
Sleep apnea
Severe cardiac disease
Hypothyroidism (treat first)
Special Populations:
Elderly Users (>65 years):
Start with 50% standard dose
More frequent monitoring required
Higher risk of glucose intolerance
Consider cardiac evaluation
Athletes and Competitors:
Both peptides are prohibited by WADA
Detection possible for 24-48 hours post-injection
Consider legal ramifications
HIV Patients:
Tesamorelin specifically studied and approved
Monitor for drug interactions
Regular viral load assessment
Lipid profile tracking essential
Compared to Alternatives: Comprehensive Analysis
Head-to-Head Comparison Matrix
| Feature | Sermorelin | Tesamorelin | CJC-1295 DAC | Ipamorelin |
|---|---|---|---|---|
| Mechanism | GHRH receptor agonist | Modified GHRH agonist | Long-acting GHRH analog | Selective ghrelin receptor agonist |
| Half-life | 8-12 minutes | 26-38 minutes | 6-8 days | 2 hours |
| Dosing frequency | Daily | Daily | Twice weekly | 2-3x daily |
| Primary benefit | Sleep, recovery | Visceral fat loss | Sustained GH elevation | Clean GH pulse |
| Side effect risk | Low | Moderate | Moderate-High | Very Low |
| Cost tier | Low-Medium | High | Medium | Low-Medium |
| Detection window | 24 hours | 48 hours | 2-4 weeks | 24 hours |
| Injection volume | 0.1-0.4 mL | 2-3 mL | 0.5-1 mL | 0.1-0.3 mL |
| FDA approval | Yes (diagnostic) | Yes (lipodystrophy) | No | No |
| Research depth | Extensive | Extensive | Moderate | Moderate |
Efficacy Comparison: Specific Applications
For Visceral Fat Reduction:
1. Tesamorelin - Superior due to sustained GH elevation and specific approval
2. CJC-1295 DAC - Good efficacy with less frequent dosing
3. Sermorelin - Moderate effects, requires consistent use
4. Ipamorelin - Mild effects, better for overall body composition
For Sleep Quality:
1. Sermorelin - Excellent for sleep architecture improvement
2. Ipamorelin - Good with minimal side effects
3. Tesamorelin - Moderate, may initially disrupt sleep
4. CJC-1295 DAC - Variable, depends on individual response
For Anti-Aging:
1. CJC-1295 DAC - Sustained elevation mimics youthful patterns
2. Tesamorelin - Comprehensive metabolic benefits
3. Sermorelin - Natural pulsatile enhancement
4. Ipamorelin - Gentle, sustainable long-term use
For Athletic Performance:
1. Ipamorelin - Clean effects without excess side effects
2. Sermorelin - Good recovery enhancement
3. CJC-1295 DAC - Powerful but requires careful timing
4. Tesamorelin - Less suitable due to metabolic focus
Cost-Benefit Analysis
Sermorelin Economics:
Typical monthly cost: $150-300
Cost per benefit unit: Moderate
Insurance coverage: Sometimes (diagnostic use)
Generic availability: Yes
Tesamorelin Economics:
Typical monthly cost: $800-1500
Cost per benefit unit: High but justified for specific indications
Insurance coverage: Limited (HIV lipodystrophy only)
Generic availability: Limited
The cost differential reflects tesamorelin's specialized development and limited competition, while sermorelin's broader availability keeps costs lower.
What's Coming Next: Future Developments
Ongoing Clinical Trials
Tesamorelin Expansion Studies
Several trials are exploring tesamorelin's applications beyond HIV lipodystrophy:
Alzheimer's Disease Research:
The TRIM study (Tesamorelin for cognition in mild cognitive impairment) is examining whether tesamorelin can slow cognitive decline in early Alzheimer's disease. Preliminary results suggest improvements in executive function and working memory.
Metabolic Syndrome Treatment:
A Phase III trial is investigating tesamorelin's efficacy in non-HIV patients with visceral adiposity and metabolic syndrome. Early data shows promising results for cardiovascular risk reduction.
Sarcopenia Prevention:
Researchers are studying tesamorelin's potential to prevent age-related muscle loss in healthy elderly individuals. The focus is on maintaining functional capacity and independence.
Sermorelin Combination Studies
New research is exploring sermorelin's potential in combination protocols:
Sleep Disorder Applications:
Studies are examining sermorelin's efficacy for treating age-related sleep disturbances, particularly in combination with melatonin and other sleep-promoting compounds.
Pediatric Growth Disorders:
Research continues into sermorelin's use as a safer alternative to growth hormone in children with growth hormone deficiency.
Emerging Formulations and Delivery Methods
Long-Acting Formulations
Pharmaceutical companies are developing extended-release versions of both peptides:
Sermorelin Depot:
A once-weekly formulation using microsphere technology could improve compliance and provide more consistent growth hormone stimulation.
Tesamorelin Extended-Release:
Monthly injection formulations are in development, potentially improving patient adherence and reducing injection site reactions.
Novel Delivery Routes
Nasal Spray Formulations:
Intranasal delivery could eliminate injection requirements while maintaining efficacy. Early studies suggest 60-70% bioavailability compared to subcutaneous injection.
Transdermal Patches:
Patch technology could provide sustained delivery with improved patient acceptance. Challenges include peptide stability and skin permeation.
Oral Formulations:
Advanced delivery systems using nanoparticles or permeation enhancers are being investigated, though significant hurdles remain.
Personalized Medicine Applications
Genetic Testing Integration
Future protocols may incorporate genetic testing to optimize treatment:
GHRH Receptor Polymorphisms:
Variations in the GHRH receptor gene could predict individual response to treatment, allowing dose optimization.
Growth Hormone Gene Variants:
Genetic differences in growth hormone production and signaling could guide peptide selection.
Metabolic Pathway Genetics:
Polymorphisms affecting fat metabolism could identify patients most likely to benefit from tesamorelin.
Biomarker-Guided Therapy
Advanced monitoring could enable precision dosing:
Continuous Glucose Monitoring:
Real-time glucose data could guide tesamorelin dosing to minimize insulin resistance risk.
Body Composition Tracking:
Advanced imaging techniques could provide more precise efficacy monitoring.
Circadian Rhythm Assessment:
Sleep and hormone monitoring could optimize sermorelin timing for individual circadian patterns.
Unanswered Research Questions
Long-Term Safety:
While short-term studies show good safety profiles, questions remain about decades-long use, particularly regarding cancer risk and cardiovascular effects.
Optimal Cycling Protocols:
The ideal balance between treatment periods and rest phases needs further investigation to maintain efficacy while minimizing tolerance.
Combination Synergies:
More research is needed on optimal peptide combinations and their long-term safety profiles.
Age-Specific Protocols:
Different age groups may benefit from distinct dosing strategies and monitoring approaches.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Making the Right Choice
• Sermorelin excels at natural growth hormone optimization with excellent safety profile and lower cost, making it ideal for sleep improvement, recovery enhancement, and general anti-aging applications.
• Tesamorelin provides superior metabolic benefits with specific efficacy for visceral fat reduction and body composition improvement, particularly valuable for metabolic syndrome and HIV lipodystrophy.
• Dosing strategies differ significantly - sermorelin works best with bedtime administration (100-2000 mcg), while tesamorelin requires consistent daily morning dosing (1-3 mg).
• Side effect profiles vary considerably - sermorelin causes minimal adverse events (mainly injection site reactions), while tesamorelin has higher rates of edema, joint pain, and glucose intolerance.
• Clinical applications are distinct - choose sermorelin for sleep disorders, general anti-aging, and growth hormone deficiency; select tesamorelin for visceral adiposity, metabolic syndrome, and cognitive enhancement.
• Stacking potential differs - sermorelin combines excellently with GHRPs for maximum growth hormone stimulation, while tesamorelin pairs well with metabolic enhancers like AOD-9604 and metformin.
• Cost considerations are significant - sermorelin costs $150-300 monthly versus tesamorelin's $800-1500, reflecting different development costs and market positioning.
• Monitoring requirements vary - sermorelin needs basic IGF-1 tracking, while tesamorelin requires comprehensive metabolic monitoring including glucose, lipids, and body composition.
• Long-term use considerations differ - sermorelin supports sustainable long-term protocols with cycling, while tesamorelin may require more careful long-term monitoring due to metabolic effects.
• Future developments promise improved formulations including long-acting versions, alternative delivery methods, and personalized dosing based on genetic testing.
Related Articles on BuyPeptidesOnline.com
CJC-1295 for Sale | Buy Online | Growth Hormone Guide
Semaglutide vs Tirzepatide | Buy Online | Complete Comparison Guide 2026-comparison)
Buy CJC-1295 Online | Growth Hormone Guide