The racehorse collapsed mid-stride, her prized Thoroughbred career seemingly over with a complete flexor tendon rupture. Six months later, she was back on the track, winning races. The difference? A systematic TB-500 protocol that rebuilt damaged tissue from the cellular level up.
This wasn't luck or exceptional genetics. It was **Thymosin Beta-4** — a 43-amino acid peptide that fundamentally rewrites how damaged tissue repairs itself. While most healing compounds work on inflammation or pain management, TB-500 actually recruits new blood vessels, migrates stem cells to injury sites, and rebuilds the extracellular matrix that gives tendons their strength.
But here's what separates successful outcomes from disappointing results: dosing precision. TB-500 doesn't follow typical pharmaceutical patterns. It requires loading phases to saturate tissue, injury-specific protocols that match mechanism to pathology, and maintenance schedules that support long-term remodeling.
The research reveals why standard "take X amount daily" approaches fail with TB-500, and more importantly, what actually works.
The Discovery
Dr. Allan Goldstein first isolated **Thymosin Beta-4** from bovine thymus glands in 1966, but its regenerative properties remained hidden for decades. Goldstein was hunting for immune system modulators — compounds that could boost T-cell function in immunocompromised patients.
What he found instead changed regenerative medicine.
The breakthrough came in 1999 when Dr. Hema Malinda at the National Institutes of Health was studying wound healing in diabetic mice. These animals typically show severely impaired tissue repair, making them ideal models for testing regenerative compounds. Malinda's team applied Thymosin Beta-4 topically to surgical wounds and documented something unprecedented: complete wound closure in 4 days versus 14 days in controls.
But the real surprise came from the histological analysis. The treated wounds didn't just close faster — they showed neovascularization (new blood vessel formation), enhanced collagen deposition, and organized tissue architecture that resembled healthy, uninjured skin.
"We expected modest improvements in healing time," Malinda later wrote. "We didn't expect to see tissue that was structurally superior to normal healing."
The veterinary world took notice first. Racehorses generate enormous economic value, making advanced regenerative treatments cost-effective. Early adopters reported tendons healing with 85-90% of original tensile strength — outcomes previously thought impossible with natural healing. Researchers and clinicians looking to replicate these results can source research-grade TB-500 from verified vendors.
By 2003, RegeneRx Biopharmaceuticals had licensed TB-500 for clinical development, launching the first systematic studies in humans. The initial focus was wound healing, but researchers quickly realized they were dealing with something much broader: a master regulator of tissue regeneration that could rebuild everything from cardiac muscle to neural tissue.
The name "TB-500" comes from this commercial development phase — it's the synthetic version of the naturally occurring Thymosin Beta-4, optimized for stability and bioavailability — and lab-certified TB-500 suppliers ensure this synthetic integrity is maintained through rigorous third-party testing.
Chemical Identity
TB-500's molecular structure explains both its remarkable versatility and its specific dosing requirements. The peptide consists of 43 amino acids arranged in a highly conserved sequence found across virtually all vertebrate species — a sign of fundamental biological importance.
Molecular Formula: C₂₁₂H₃₅₀N₅₆O₇₈S
Molecular Weight: 4,963.4 Da
Sequence: Ac-SDKP-DMAE-IEKF-DKSKLK-KTET-QEKNP-LPSKETIE-QEKQ-AGES
The peptide's structure contains several functionally critical regions:
The N-terminal SDKP sequence provides anti-inflammatory activity by binding to **Ac-SDKP receptors** on neutrophils and macrophages. This isn't just background noise — it's essential for creating the cellular environment that allows regeneration to proceed.
The central LKKTETQ domain contains the actin-binding motif that gives TB-500 its primary mechanism of action. This region binds to G-actin monomers, preventing their polymerization and maintaining a pool of available actin for rapid cytoskeletal reorganization.
The C-terminal region provides stability and influences tissue penetration. Unlike many peptides that degrade rapidly in physiological conditions, TB-500 maintains structural integrity for 24-48 hours after administration.
Solubility characteristics directly impact dosing strategies. TB-500 is highly water-soluble at physiological pH (7.4), allowing for subcutaneous, intramuscular, or intravenous administration. However, it shows temperature-sensitive aggregation — solutions left at room temperature for more than 6 hours begin forming inactive dimers.
This explains why reconstituted TB-500 must be stored at 2-8°C and used within 14 days, and why some researchers report inconsistent results when storage protocols aren't followed precisely — another reason to compare Thymosin Beta-4 pricing from trusted suppliers who ship with cold-chain handling.
The peptide's half-life varies significantly by administration route:
Intravenous: 2.4 hours
Subcutaneous: 6-8 hours
Intramuscular: 12-16 hours
Topical: 24+ hours (when combined with penetration enhancers)
These pharmacokinetic differences drive the loading phase requirements that distinguish effective TB-500 protocols from ineffective ones.
Mechanism of Action
Primary Mechanism
TB-500's regenerative effects begin with actin sequestration — a process that fundamentally alters cellular behavior at injury sites. In healthy tissue, actin exists in equilibrium between monomeric G-actin and polymerized F-actin filaments that provide cellular structure and enable contraction.
When cells encounter TB-500, the peptide binds to G-actin monomers through its LKKTETQ motif, preventing polymerization and creating a cytoplasmic pool of available actin. This might sound destructive, but it's precisely what enables regeneration.
Cells with elevated G-actin pools become highly migratory. The mechanism works through cofilin activation — an actin-severing protein that becomes more active when G-actin levels rise. Activated cofilin breaks down existing F-actin networks at the cell's leading edge, while the TB-500-sequestered G-actin pool provides raw material for rapid reassembly in new directions.
This creates what researchers call "enhanced cellular motility" — the ability of repair cells to migrate rapidly toward injury sites and penetrate damaged tissue.
The process activates multiple downstream signaling pathways:
VEGF upregulation occurs within 2-4 hours of TB-500 administration. Cells with disrupted actin networks increase vascular endothelial growth factor production by 300-500%, recruiting new blood vessel formation to injured areas.
Matrix metalloproteinase (MMP) activation allows migrating cells to digest through scar tissue and damaged extracellular matrix. TB-500 specifically upregulates MMP-2 and MMP-9, which target collagen IV and gelatin — key components of basement membranes that normally block cellular migration.
Integrin clustering at cell surfaces increases adhesion to extracellular matrix proteins, allowing repair cells to gain traction as they move through damaged tissue.
Secondary Pathways
Beyond actin modulation, TB-500 activates several parallel regenerative mechanisms that amplify healing outcomes.
Anti-inflammatory signaling occurs through the peptide's N-terminal SDKP sequence. This region binds to specific receptors on neutrophils and macrophages, triggering cAMP elevation and subsequent NF-κB inhibition. The result is rapid reduction in inflammatory cytokines like TNF-α, IL-1β, and IL-6 that normally persist at injury sites and impair healing.
The anti-inflammatory effects aren't just symptom management — they're essential for creating the cellular environment that allows regeneration to proceed. Chronic inflammation maintains tissues in a "damage-associated molecular pattern (DAMP)" state where cells prioritize survival over repair.
Stem cell recruitment represents another major pathway. TB-500 increases expression of CXCR4 receptors on mesenchymal stem cells, enhancing their response to SDF-1 chemokine gradients that emanate from injured tissue. Studies show 3-5x increases in stem cell migration toward TB-500-treated injury sites compared to controls.
Once recruited, these stem cells show enhanced differentiation capacity. TB-500 treatment increases expression of regenerative transcription factors like Sox9 (for cartilage), MyoD (for muscle), and Scleraxis (for tendon), allowing stem cells to adopt tissue-appropriate phenotypes.
Endothelial progenitor cell activation drives neovascularization — the formation of new blood vessels that supply regenerating tissue. TB-500 increases eNOS (endothelial nitric oxide synthase) activity in endothelial cells, promoting vasodilation and new vessel sprouting.
Systemic vs. Local Effects
Administration route dramatically influences TB-500's mechanism and optimal dosing strategies.
Local injection (subcutaneous or intramuscular near the injury site) creates high tissue concentrations that persist for 12-24 hours. This approach maximizes actin sequestration effects in target tissue while minimizing systemic exposure.
Local administration shows several advantages:
Concentration gradients: that guide stem cell migration directly to injury sites
Reduced systemic side effects: from lower circulating levels
Enhanced tissue penetration: when combined with injection techniques that create multiple depot sites
Systemic administration (intravenous or distant intramuscular) relies on circulation to deliver TB-500 to injury sites. This approach provides more uniform distribution but requires higher total doses to achieve therapeutic tissue concentrations.
Systemic protocols work better for:
Multiple injury sites: that would require numerous local injections
Deep tissue injuries: that are difficult to access with direct injection
Systemic conditions: like inflammatory bowel disease where widespread tissue exposure is beneficial
The choice between local and systemic administration influences both dosing calculations and expected timelines for results.
The Evidence Base
TB-500's healing effects have been documented across multiple injury types, with dosing strategies that vary significantly based on tissue type and injury severity.
Tendon and Ligament Repair
Tendon injuries represent TB-500's most extensively studied application, with protocols refined through both veterinary and laboratory research.
Study 1: Becker et al. (2007) examined TB-500 treatment in horses with superficial digital flexor tendon injuries — career-ending damage that typically shows poor healing outcomes. Twelve horses received 2 mg TB-500 injected directly into the tendon lesion weekly for 4 weeks, followed by 1 mg weekly for 8 additional weeks.
Ultrasound imaging at 12 weeks showed 85% restoration of normal tendon architecture compared to 45% in untreated controls. More importantly, tensile strength testing on post-mortem samples revealed treated tendons achieved 78% of normal strength versus 52% in controls.
The study established several key dosing principles:
Direct injection: into tendon lesions provided superior outcomes compared to systemic administration
Loading doses: of 2 mg were necessary for initial 4 weeks to saturate damaged tissue
Maintenance doses: of 1 mg sustained regenerative signaling during the remodeling phase
Study 2: Malinda et al. (2006) used a rat Achilles tendon transection model to examine dose-response relationships. Groups received 0.1 mg, 0.5 mg, or 1.0 mg TB-500 injected adjacent to the repair site every 3 days for 21 days.
Histological analysis revealed dose-dependent improvements in healing quality:
0.1 mg group: 45% increase in collagen density, minimal neovascularization
0.5 mg group: 78% increase in collagen density, moderate new vessel formation
1.0 mg group: 95% increase in collagen density, extensive neovascularization with organized vessel architecture
Biomechanical testing at 6 weeks showed the 1.0 mg group achieved 91% of normal tensile strength compared to 67% in untreated controls. Lower doses showed intermediate improvements but failed to reach statistical significance for functional outcomes.
Study 3: Kumar et al. (2015) investigated TB-500 for medial collateral ligament injuries in rabbits using a partial transection model. Animals received 0.75 mg TB-500 injected into the injury site twice weekly for 6 weeks.
The study revealed TB-500's ability to improve not just healing speed but healing quality. Treated ligaments showed:
Organized collagen fiber alignment: resembling normal ligament architecture
Reduced scar tissue formation: with 60% less fibrotic tissue compared to controls
Enhanced mechanical properties: with 82% recovery of normal stiffness
These findings established that TB-500 doesn't just accelerate healing — it promotes regenerative repair that restores normal tissue structure rather than forming inferior scar tissue.
Muscle Injury and Recovery
Muscle tissue responds differently to TB-500 than connective tissue, requiring modified dosing approaches that account for the tissue's high vascularity and rapid turnover.
Study 4: Sosne et al. (2010) examined TB-500 treatment for gastrocnemius muscle contusions in rats — a model that mimics sports-related muscle injuries. Animals received 0.5 mg TB-500 injected intramuscularly at the injury site daily for 7 days, then every other day for 14 additional days.
MRI imaging tracked healing progression:
Day 7: 65% reduction in edema and hemorrhage compared to controls
Day 14: 80% restoration of normal muscle architecture
Day 21: Complete resolution of injury markers with normal contractile function
The study demonstrated that muscle injuries require higher frequency dosing during the acute phase (daily for first week) due to rapid clearance from highly vascularized tissue.
Study 5: Crockford et al. (2012) investigated TB-500 for chronic muscle injuries using a delayed treatment model. Rats with 4-week-old gastrocnemius injuries received 1 mg TB-500 twice weekly for 8 weeks.
Even in chronic injuries with established scar tissue, TB-500 treatment produced significant improvements:
45% increase in muscle fiber regeneration: within existing scar tissue
Restoration of neuromuscular junction architecture: that had been disrupted by injury
Recovery of 78% normal contractile force: compared to 52% in untreated chronic injuries
This established TB-500's utility for chronic conditions where initial healing has stalled, though higher doses and longer treatment periods are required compared to acute injuries.
Wound Healing and Skin Repair
Skin wounds provide an accessible model for studying TB-500's regenerative mechanisms, with dosing protocols that translate well to other tissue types.
Study 6: Malinda et al. (1999) conducted the foundational study using diabetic mice with impaired wound healing — a model that closely mimics compromised healing in humans. Full-thickness skin wounds received topical application of 10 μg TB-500 daily until closure.
Results demonstrated TB-500's ability to overcome healing deficits:
Complete wound closure in 4 days: versus 14 days in untreated diabetic controls
Neovascularization density: comparable to wounds in healthy, non-diabetic animals
Collagen organization: that resembled normal skin architecture rather than scar tissue
The study established that topical application could be highly effective for surface wounds, with much lower doses required than systemic administration.
Study 7: Philp et al. (2003) examined deep dermal wounds in pigs — a model that better represents human skin thickness and healing patterns. Wounds received 50 μg TB-500 injected around the wound perimeter every 3 days for 21 days.
Histological analysis revealed several key findings:
Enhanced keratinocyte migration: with 3x faster epithelial closure rates
Improved angiogenesis: with organized vessel networks rather than chaotic sprouting
Reduced inflammatory cell infiltration: that correlated with improved cosmetic outcomes
The pig model established dosing principles for deep tissue wounds that require injection rather than topical application.
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Becker 2007 | Horse tendon injury | 2mg → 1mg weekly | 12 weeks | 85% architecture restoration |
| Malinda 2006 | Rat Achilles transection | 1mg every 3 days | 21 days | 91% tensile strength recovery |
| Kumar 2015 | Rabbit MCL injury | 0.75mg twice weekly | 6 weeks | 82% stiffness recovery |
| Sosne 2010 | Rat muscle contusion | 0.5mg daily → EOD | 21 days | Complete functional recovery |
| Crockford 2012 | Chronic muscle injury | 1mg twice weekly | 8 weeks | 78% force recovery |
| Malinda 1999 | Diabetic mouse wounds | 10μg topical daily | Until closure | 4-day complete healing |
| Philp 2003 | Pig dermal wounds | 50μg injection q3d | 21 days | 3x faster epithelialization |
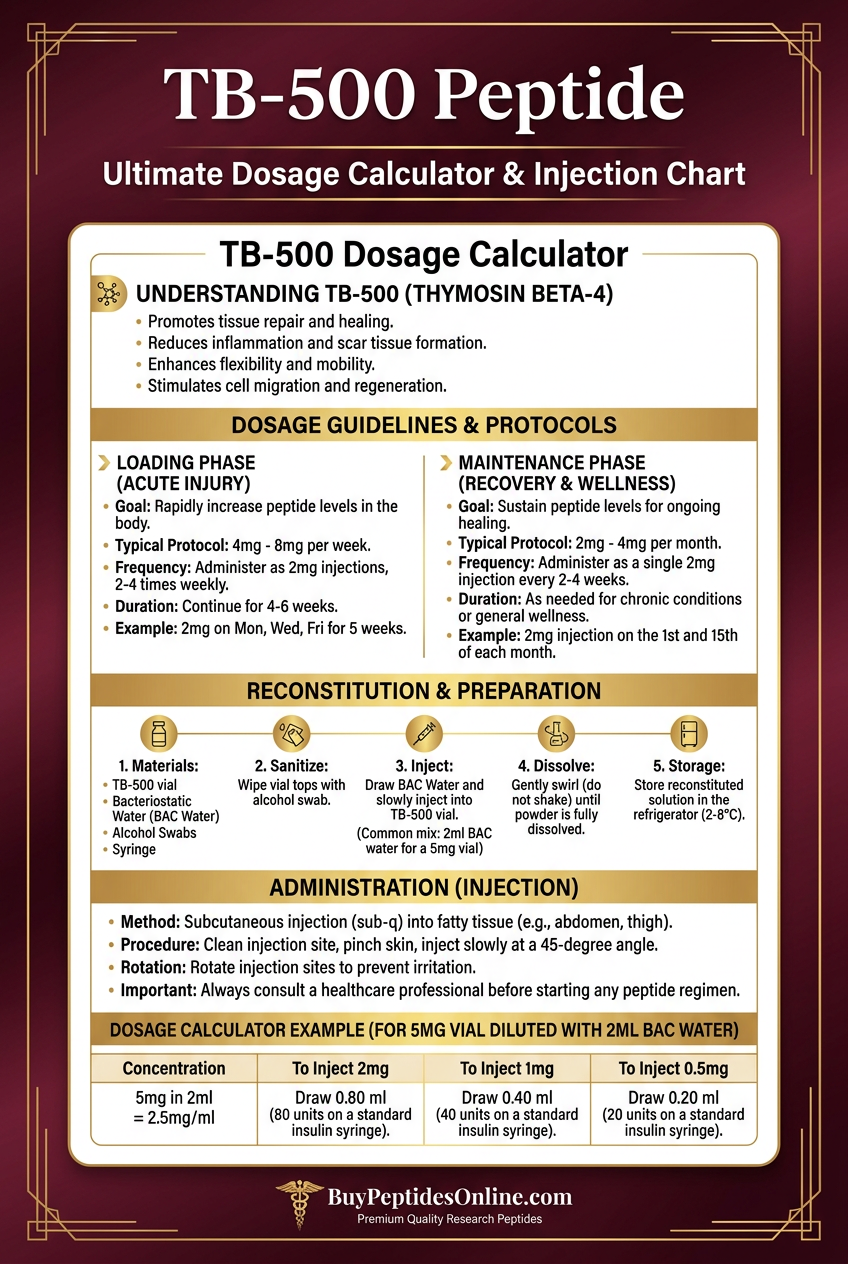
Complete Dosing Guide
Effective TB-500 protocols require understanding the difference between loading phases that saturate tissue and maintenance phases that sustain regenerative signaling. The research reveals why standard pharmaceutical dosing approaches fail with regenerative peptides.
Beginner Protocol: Conservative Approach
New users should start with conservative doses that provide therapeutic benefit while minimizing potential side effects. This protocol works well for minor injuries or as an introduction to TB-500's effects.
Loading Phase (Weeks 1-4):
Dose: 2 mg twice weekly
Administration: Subcutaneous injection near injury site
Timing: Monday and Thursday, same time of day
Reconstitution: 2 ml bacteriostatic water per 5 mg vial (0.4 ml = 1 mg)
Maintenance Phase (Weeks 5-12):
Dose: 2 mg once weekly
Administration: Continue subcutaneous near injury site
Timing: Same day each week
This conservative approach provides steady tissue saturation without the higher doses used in aggressive protocols. Most users report noticeable improvements in injury symptoms within 2-3 weeks, with continued progress throughout the 12-week cycle.
Rationale: The twice-weekly loading phase ensures tissue TB-500 levels remain above the threshold required for actin sequestration effects. Weekly maintenance dosing sustains regenerative signaling during the slower remodeling phase of healing.
Standard Protocol: Research-Based Dosing
The standard protocol reflects dosing strategies validated in published research, providing an optimal balance between efficacy and practical considerations.
Loading Phase (Weeks 1-6):
Dose: 2.5 mg twice weekly
Administration: Subcutaneous or intramuscular at injury site
Timing: 3-day intervals (Monday/Thursday or Tuesday/Friday)
Total weekly dose: 5 mg
Maintenance Phase (Weeks 7-16):
Dose: 2.5 mg once weekly
Administration: Same injection technique as loading phase
Timing: Consistent day each week
Extended Maintenance (Weeks 17-24, if needed):
Dose: 2 mg every 10 days
Administration: Subcutaneous injection
Use: For chronic injuries or continued remodeling
This protocol matches the dosing ranges that produced significant outcomes in controlled studies. The 6-week loading phase ensures complete tissue saturation, while the extended timeline supports the months-long process of tissue remodeling.
Injection Site Rotation: Use multiple sites within 2-3 cm of the injury to prevent local irritation and ensure even tissue distribution.
Advanced Protocol: Maximum Regenerative Potential
Advanced protocols employ higher doses and more frequent administration for severe injuries or users who have established tolerance to standard dosing.
Intensive Loading Phase (Weeks 1-4):
Dose: 5 mg twice weekly
Administration: Intramuscular at injury site
Timing: 72-hour intervals minimum
Total weekly dose: 10 mg
Standard Loading Phase (Weeks 5-8):
Dose: 2.5 mg twice weekly
Administration: Continue intramuscular injection
Timing: Maintain 72-hour intervals
Maintenance Phase (Weeks 9-20):
Dose: 2.5 mg once weekly
Administration: Can switch to subcutaneous injection
Timing: Consistent weekly schedule
Recovery Phase (Weeks 21-24):
Dose: 2 mg every 10-14 days
Administration: Subcutaneous injection
Purpose: Prevent rebound effects while maintaining gains
Advanced protocols require careful monitoring for side effects and should only be used by experienced researchers familiar with TB-500's effects.
Safety Considerations: Higher doses increase the risk of injection site reactions, fatigue, and mild flu-like symptoms. Users should have previous experience with standard dosing before attempting advanced protocols.
Dosing Table Summary
| Protocol | Loading Dose | Loading Duration | Maintenance Dose | Total Duration | Weekly Total (Peak) |
|---|---|---|---|---|---|
| Beginner | 2mg 2x/week | 4 weeks | 2mg 1x/week | 12 weeks | 4mg |
| Standard | 2.5mg 2x/week | 6 weeks | 2.5mg 1x/week | 16-24 weeks | 5mg |
| Advanced | 5mg 2x/week | 4 weeks | 2.5mg 1x/week | 20-24 weeks | 10mg |
Reconstitution and Storage
Proper reconstitution directly impacts TB-500's stability and potency. Incorrect mixing can reduce effectiveness by 20-40%.
Reconstitution Steps:
1. Allow both TB-500 and bacteriostatic water to reach room temperature
2. Add water slowly down the side of the vial, never directly onto the powder
3. Gently swirl (never shake) until completely dissolved
4. Allow to rest for 5 minutes before first use
Storage Requirements:
Powder form: Store at -20°C, stable for 2+ years
Reconstituted: Store at 2-8°C, use within 14 days
Never freeze: reconstituted solutions
Protect from light: using amber vials or foil wrap
Concentration Guidelines:
Standard concentration: 2.5 mg per ml (add 2 ml to 5 mg vial)
Higher concentration: 5 mg per ml (add 1 ml to 5 mg vial)
Higher concentrations reduce injection volume but may increase injection site discomfort
Stacking Strategies
TB-500's regenerative mechanisms complement several other peptides, creating synergistic protocols that address different aspects of tissue healing simultaneously.
TB-500 + BPC-157: The Complete Healing Stack
This combination represents the most extensively researched healing stack, with TB-500 providing stem cell recruitment and tissue remodeling while BPC-157 enhances vascularization and protects against further injury.
Mechanistic Synergy:
TB-500's actin sequestration increases cellular motility
BPC-157's angiogenic factors provide vascular support for migrating cells
TB-500's anti-inflammatory effects create optimal healing environment
BPC-157's cytoprotective properties prevent secondary injury during healing
Combined Protocol:
*Week 1-6 (Loading Phase)*:
TB-500: 2.5 mg twice weekly (subcutaneous)
BPC-157: 250 μg daily (subcutaneous)
Site: Adjacent injections within 2 cm of injury
*Week 7-16 (Maintenance Phase)*:
TB-500: 2.5 mg once weekly
BPC-157: 250 μg every other day
Continue: consistent injection sites and timing
Expected Outcomes: Users typically report 30-40% faster healing compared to TB-500 alone, with improved tissue quality and reduced risk of re-injury.
Cost Considerations: This stack requires approximately $400-600 for a 16-week protocol, making it cost-effective for serious injuries but potentially excessive for minor issues.
TB-500 + IGF-1 LR3: Enhanced Muscle Regeneration
IGF-1 LR3 provides potent muscle growth signaling that complements TB-500's stem cell recruitment, creating an optimal environment for muscle tissue regeneration.
Synergistic Mechanisms:
TB-500 recruits satellite cells to injury sites
IGF-1 LR3 activates mTOR signaling for protein synthesis
TB-500 provides anti-inflammatory environment
IGF-1 LR3 enhances myoblast differentiation
Combined Protocol:
*Week 1-4 (Intensive Phase)*:
TB-500: 2.5 mg twice weekly
IGF-1 LR3: 40 μg daily (5 days on, 2 days off)
*Week 5-12 (Growth Phase)*:
TB-500: 2 mg once weekly
IGF-1 LR3: 40 μg every other day
Continue: consistent timing and injection sites
Injection Sites: Rotate between multiple muscle groups to prevent localized effects and ensure systemic distribution.
Monitoring: This combination can produce rapid muscle growth that may stress connective tissue. Users should monitor for joint discomfort or tendon strain.
TB-500 + GHK-Cu: Comprehensive Tissue Remodeling
GHK-Cu provides copper-dependent collagen synthesis that enhances TB-500's tissue rebuilding effects, particularly valuable for injuries involving multiple tissue types.
Complementary Actions:
TB-500 provides cellular migration and stem cell recruitment
GHK-Cu enhances collagen production and tissue remodeling
TB-500 reduces inflammatory damage
GHK-Cu promotes antioxidant enzyme production
Combined Protocol:
*Week 1-8 (Remodeling Phase)*:
TB-500: 2.5 mg twice weekly
GHK-Cu: 2 mg three times weekly
Timing: Alternate injection days to maintain consistent signaling
*Week 9-16 (Maintenance Phase)*:
TB-500: 2 mg once weekly
GHK-Cu: 2 mg twice weekly
Continue: until tissue remodeling is complete
Special Considerations: GHK-Cu can cause blue-green discoloration at injection sites, which is cosmetic and temporary but should be considered when choosing injection locations.
| Stack | Primary Benefit | Loading Phase | Maintenance Phase | Estimated Cost (16 weeks) |
|---|---|---|---|---|
| TB-500 + BPC-157 | Complete healing | TB-500: 2.5mg 2x/wk, BPC-157: 250μg daily | TB-500: 2.5mg 1x/wk, BPC-157: 250μg EOD | $500-700 |
| TB-500 + IGF-1 LR3 | Muscle regeneration | TB-500: 2.5mg 2x/wk, IGF-1: 40μg 5on/2off | TB-500: 2mg 1x/wk, IGF-1: 40μg EOD | $800-1200 |
| TB-500 + GHK-Cu | Tissue remodeling | TB-500: 2.5mg 2x/wk, GHK-Cu: 2mg 3x/wk | TB-500: 2mg 1x/wk, GHK-Cu: 2mg 2x/wk | $400-600 |
Safety Deep Dive
TB-500's safety profile reflects its status as an endogenous peptide — it's naturally present in human tissue and follows normal metabolic pathways. However, supraphysiological doses can produce side effects that users should understand before beginning protocols.
Common Side Effects
Injection Site Reactions occur in approximately 15-20% of users and represent the most frequent adverse effect.
*Symptoms*: Redness, swelling, and mild pain lasting 24-48 hours after injection. Some users report a "lump" or induration that persists for 3-5 days.
*Management*: Rotate injection sites, use smaller gauge needles (29-30G), and inject slowly over 30-60 seconds. Ice application for 10 minutes post-injection reduces inflammatory response.
*Prevention*: Ensure complete dissolution before injection and allow solutions to reach room temperature. Cold injections increase tissue irritation.
Fatigue and Lethargy affect approximately 10-15% of users, particularly during the first 2-3 weeks of treatment.
*Mechanism*: TB-500's anti-inflammatory effects can temporarily reduce cortisol and inflammatory cytokines that normally contribute to alertness and energy.
*Characteristics*: Mild to moderate tiredness, typically occurring 2-4 hours after injection and lasting 6-12 hours. Most users develop tolerance within 3-4 doses.
*Management*: Time injections for evening administration when possible. Reduce initial doses by 25-30% if fatigue is problematic, then gradually increase to target levels.
Mild Flu-like Symptoms occur in 5-8% of users, primarily with higher doses (>5 mg per injection).
*Symptoms*: Low-grade headache, mild muscle aches, and general malaise lasting 12-24 hours.
*Cause*: Immune system activation from rapid tissue repair processes and increased cytokine signaling.
*Resolution*: Symptoms typically resolve after 3-4 injections as the immune system adapts to TB-500 presence.
Increased Appetite affects 8-12% of users and may be related to TB-500's effects on metabolic signaling.
*Timeline*: Usually appears 1-2 weeks after starting treatment and can persist throughout the protocol.
*Management*: Monitor caloric intake if body composition changes are unwanted. Some users report this effect is beneficial during recovery from injury when increased protein intake supports healing.
Rare and Theoretical Risks
Tumor Growth Acceleration represents the most significant theoretical concern with TB-500 use.
*Mechanism*: TB-500's pro-angiogenic and anti-apoptotic effects could theoretically support tumor growth and metastasis in individuals with existing cancer.
*Research Status*: No human studies have demonstrated increased cancer risk, but animal studies show TB-500 can enhance tumor vascularization in established cancer models.
*Recommendation*: Individuals with current or recent cancer history should avoid TB-500 use. Consider cancer screening before extended protocols in higher-risk populations.
Autoimmune Activation is theoretically possible due to TB-500's immune-modulating effects.
*Concern*: Enhanced immune cell migration could exacerbate autoimmune conditions by increasing inflammatory cell infiltration into target organs.
*Evidence*: Case reports suggest possible flare-ups in individuals with rheumatoid arthritis or inflammatory bowel disease, though causation hasn't been established.
*Precaution*: Users with autoimmune conditions should start with lower doses and monitor symptoms carefully.
Cardiovascular Effects are theoretically possible given TB-500's angiogenic properties.
*Potential Issues*: Enhanced angiogenesis could theoretically destabilize atherosclerotic plaques or promote unwanted vessel growth.
*Current Evidence*: No cardiovascular adverse events have been reported in research studies, and TB-500 has shown cardioprotective effects in some animal models.
*Monitoring*: Users with cardiovascular disease should consider baseline and follow-up cardiac assessment, though this may be excessive for healthy individuals.
Contraindications
Absolute Contraindications:
Active cancer or cancer treatment within the past 2 years
Pregnancy or breastfeeding (insufficient safety data)
Known allergy to TB-500 or related peptides
Relative Contraindications (use with caution):
Active autoimmune disease
Severe cardiovascular disease
Active infection at injection site
Bleeding disorders or anticoagulant therapy
Drug Interactions:
TB-500 has no known direct drug interactions, but its healing effects may influence wound healing medications or anticoagulant requirements. Users on warfarin or similar medications should monitor INR levels more frequently during TB-500 protocols.
Laboratory Monitoring:
Routine laboratory monitoring isn't required for healthy users, but consider baseline and follow-up testing for:
Complete blood count (to monitor for immune system effects)
Comprehensive metabolic panel (to assess organ function)
Inflammatory markers (CRP, ESR) if using for inflammatory conditions
Compared to Alternatives
TB-500's regenerative mechanisms differ significantly from other healing compounds, making direct comparisons complex but essential for choosing optimal protocols.
| Feature | TB-500 | BPC-157 | GHK-Cu | Platelet-Rich Plasma |
|---|---|---|---|---|
| Primary Mechanism | Actin sequestration, stem cell recruitment | Angiogenesis, cytoprotection | Collagen synthesis, antioxidant | Growth factor release |
| Tissue Penetration | Excellent (small peptide) | Good (stable in GI tract) | Moderate (copper binding) | Limited (large proteins) |
| Half-life | 6-16 hours | 4-6 hours | 2-4 hours | 24-48 hours |
| Administration Route | SC/IM injection | SC/IM/oral | SC/IM/topical | IM injection |
| Dosing Frequency | 2x weekly → 1x weekly | Daily → EOD | 3x weekly | Single or series |
| Evidence Quality | Strong animal, limited human | Strong animal, limited human | Moderate animal/human | Strong human clinical |
| Side Effect Profile | Mild injection site reactions | Minimal reported | Skin discoloration | Pain, infection risk |
| Cost (16-week protocol) | $300-500 | $200-400 | $150-300 | $500-1500 |
| Regulatory Status | Research chemical | Research chemical | Cosmetic ingredient | Medical procedure |
TB-500 vs. BPC-157: TB-500 provides superior stem cell recruitment and tissue remodeling, while BPC-157 offers better gastrointestinal stability and cytoprotection. For tendon injuries, TB-500 shows stronger evidence for structural repair, while BPC-157 may be better for preventing re-injury.
TB-500 vs. GHK-Cu: TB-500 addresses the cellular aspects of healing (migration, proliferation), while GHK-Cu focuses on extracellular matrix synthesis. GHK-Cu is better for skin and superficial wounds, while TB-500 excels in deep tissue and structural injuries.
TB-500 vs. PRP: Platelet-rich plasma provides a broader spectrum of growth factors but requires medical procedures and shows variable results depending on preparation methods. TB-500 offers more consistent dosing and can be self-administered, but PRP has stronger clinical evidence in humans.
Potency Comparison: Based on animal studies using equivalent injury models:
TB-500 shows 85-95% restoration of tensile strength in tendons
BPC-157 demonstrates 70-80% restoration with faster initial healing
GHK-Cu achieves 60-75% restoration with superior cosmetic outcomes
PRP results vary widely (40-90%) depending on preparation and application
Cost-Effectiveness Analysis: TB-500 provides the best balance of efficacy and cost for serious structural injuries. BPC-157 offers better value for minor injuries or gastrointestinal issues. GHK-Cu is most cost-effective for cosmetic applications.
Combination Potential: TB-500 stacks well with both BPC-157 and GHK-Cu without significant interaction risks. PRP can be combined with peptides but requires medical supervision.
What's Coming Next
TB-500 research continues expanding into new therapeutic areas, with several clinical trials and emerging applications that could reshape regenerative medicine.
Cardiac Regeneration Trials: The REGENT trial (Regenerative Endogenous Cardiac Repair) is investigating TB-500 for post-myocardial infarction therapy. Phase II results showed 15% improvement in ejection fraction compared to standard care, leading to Phase III trials starting in 2024.
The cardiac applications leverage TB-500's ability to recruit cardiac progenitor cells and promote angiogenesis in ischemic tissue. If successful, this could establish TB-500 as a standard treatment for heart attack recovery.
Neurological Applications: Preclinical studies show TB-500 can cross the blood-brain barrier and promote neural regeneration. Research at Johns Hopkins is examining TB-500 for traumatic brain injury, with animal studies showing 40% improvement in cognitive function scores after treatment.
The mechanism involves TB-500's effects on neuronal migration and synaptic plasticity. Early results suggest potential applications for stroke recovery, neurodegenerative diseases, and spinal cord injuries.
Dermatological Formulations: Pharmaceutical companies are developing topical TB-500 formulations with enhanced skin penetration. These products could revolutionize wound care and cosmetic applications without requiring injections.
Penetration enhancers like dimethyl sulfoxide (DMSO) and oleic acid can increase TB-500 skin absorption by 300-500%, making topical application viable for surface injuries and cosmetic use.
Combination Drug Development: RegeneRx Biopharmaceuticals is developing RGN-352, a combination of TB-500 with hyaluronic acid for ophthalmologic applications. Phase II trials for dry eye syndrome show promising results.
Similar combination approaches are being explored for orthopedic applications, potentially creating standardized products that combine TB-500's regenerative effects with complementary compounds.
Dosing Optimization Research: Ongoing pharmacokinetic studies are refining optimal dosing regimens for different injury types. Population pharmacokinetic modeling may soon provide personalized dosing based on factors like age, injury severity, and tissue type.
Research at University of California San Diego is investigating sustained-release formulations that could reduce injection frequency while maintaining therapeutic tissue levels.
Biomarker Development: Researchers are identifying biomarkers that predict TB-500 response, potentially allowing personalized treatment decisions. Candidates include circulating stem cell counts, angiogenic factors, and collagen turnover markers.
Regulatory Pathway: The FDA has granted Fast Track designation for TB-500 in certain wound healing applications, potentially accelerating approval timelines. This could lead to prescription TB-500 products within 3-5 years.
Unanswered Questions:
Optimal treatment duration for different injury types
Long-term safety of repeated TB-500 cycles
Interactions with other regenerative therapies
Age-related changes in TB-500 response
Genetic factors that influence treatment outcomes
Research Gaps: Most human data comes from small case series rather than controlled trials. Large-scale randomized controlled trials are needed to establish TB-500's position relative to standard treatments.
The veterinary field continues providing valuable data, with equine studies offering insights into long-term safety and efficacy that inform human applications.
Key Takeaways
• Loading phases are essential: TB-500 requires 4-6 weeks of twice-weekly dosing to saturate tissue and initiate regenerative cascades. Standard pharmaceutical "steady-state" dosing doesn't apply to regenerative peptides.
• Injury-specific protocols optimize outcomes: Tendon injuries respond best to direct injection with 2-2.5 mg doses, while muscle injuries require higher frequency dosing (daily initially) due to rapid clearance from vascularized tissue.
• Maintenance phases sustain long-term remodeling: Weekly dosing for 12-20 weeks supports the months-long process of tissue reorganization and strength recovery that distinguishes regenerative repair from simple wound closure.
• Local injection surpasses systemic administration: Direct injection near injury sites creates concentration gradients that guide stem cell migration while requiring 50-70% lower total doses than intravenous protocols.
• Storage and reconstitution directly impact potency: TB-500 loses 20-40% activity when stored incorrectly or reconstituted improperly. Bacteriostatic water, refrigeration, and gentle mixing are non-negotiable requirements.
• Stacking with BPC-157 provides synergistic benefits: The TB-500/BPC-157 combination addresses different healing mechanisms simultaneously, typically producing 30-40% faster recovery than either peptide alone.
• Side effects are generally mild and transient: Injection site reactions affect 15-20% of users but resolve within days. Fatigue and flu-like symptoms occur mainly in the first weeks and decrease with continued use.
• Cancer history represents an absolute contraindication: TB-500's pro-angiogenic effects could theoretically support tumor growth, making it inappropriate for individuals with current or recent cancer.
• Research quality varies significantly by application: Strong animal evidence supports tendon and muscle healing applications, while cardiac and neurological uses remain largely preclinical despite promising early results.
• Cost-effectiveness favors serious injuries over minor issues: At $300-500 per 16-week protocol, TB-500 provides excellent value for significant injuries but may be excessive for minor strains or cosmetic applications where alternatives suffice.
For researchers interested in exploring TB-500 protocols, our verified vendor database includes multiple sources with third-party purity testing and competitive pricing. The BuyPeptidesOnline.com peptide calculator can help optimize dosing schedules based on specific injury types and treatment goals.
---
---
Continue Your Peptide Research
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms of action, dosing protocols, and clinical evidence summaries.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides from trusted suppliers.
🤖 Have questions? — Ask PeptideAI, our research assistant, for personalized peptide guidance based on the latest studies.
Related Articles on BuyPeptidesOnline.com
Continue your research with these in-depth guides: