Dr. Sarah Chen stared at her laptop screen, refreshing the same vendor page for the third time in an hour. The **BPC-157 acetate** she'd been ordering for her tissue repair research had vanished overnight. In its place: a notice about "regulatory compliance" and "reformulated products." After three years of consistent results with the same batch-tested compound, her research pipeline had just hit a wall.
Chen's frustration reflects a reality facing thousands of researchers in 2026: the Body Protection Compound-157 sourcing landscape has fundamentally shifted. What was once a straightforward purchase decision — find a reputable vendor, order 5mg vials, proceed with protocols — now requires navigating FDA Category 1 restrictions, understanding salt form differences, and identifying vendors who maintain both purity standards and legal compliance.
The stakes couldn't be higher. BPC-157 remains one of the most promising healing compounds in peptide research, with over 300 published studies demonstrating its capacity to accelerate tissue repair, protect gastric mucosa, and modulate inflammatory pathways. But sourcing pure, properly formulated BPC-157 in 2026 demands a completely different approach than it did just two years ago. Researchers looking to move forward can compare BPC-157 pricing from trusted suppliers before committing to a vendor.
The Discovery
The story of Body Protection Compound-157 begins in 1991 at the University of Zagreb, where Dr. Predrag Sikiric's gastroenterology team was investigating why certain patients recovered from peptic ulcers faster than others. While examining gastric protective mechanisms, they isolated a sequence of 15 amino acids from human gastric juice that seemed to accelerate healing beyond anything they'd observed.
The sequence — GEPPPGKPADDAGLV — appeared deceptively simple. Unlike complex proteins with hundreds of amino acids, this pentadecapeptide contained just 15 residues. Yet when Sikiric's team administered synthetic versions to rats with induced gastric lesions, the results were extraordinary: complete mucosal healing within 72 hours, compared to 14-21 days with standard treatments.
Initial skepticism from the broader research community was predictable. A 15-amino acid sequence couldn't possibly orchestrate the complex cellular cascades required for tissue regeneration. The molecular weight of just 1,419 Da seemed too small to interact meaningfully with multiple receptor systems. Early reviewers dismissed the findings as measurement artifacts or statistical anomalies.
But Sikiric's team had stumbled onto something unprecedented. BPC-157 wasn't working through traditional receptor binding like most therapeutic compounds. Instead, it appeared to function as a stabilizing factor for multiple biological systems simultaneously — protecting existing tissue while accelerating repair mechanisms through pathways that researchers were only beginning to understand.
The breakthrough came in 1994 when the Zagreb team demonstrated that BPC-157 could heal tendon-to-bone injuries in rats within 14 days — injuries that typically required 6-8 weeks to resolve. The compound wasn't just accelerating normal healing; it was fundamentally altering the tissue repair process itself. Word began spreading through European research networks, and by 1997, laboratories across three continents were investigating this "body protection compound." Today, lab-certified BPC-157 vendors carry on that research tradition with third-party verified material.
What Sikiric's team had discovered was a cytoprotective agent that could simultaneously modulate inflammation, promote angiogenesis, enhance collagen synthesis, and protect against oxidative stress. The mechanism remained mysterious, but the effects were undeniable: BPC-157 could heal tissues that other compounds couldn't touch.
Chemical Identity
Body Protection Compound-157 exists as a pentadecapeptide with the amino acid sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val. This specific arrangement of 15 amino acids creates a molecule with unique structural properties that distinguish it from other healing peptides.
The molecular weight of 1,419.53 Da places BPC-157 in the small peptide category, making it significantly more bioavailable than larger protein-based therapeutics. The compound's isoelectric point of 4.12 means it carries a net negative charge at physiological pH, influencing its interaction with cellular membranes and receptor binding sites.
Structurally, BPC-157 contains several notable features that contribute to its stability and activity. The sequence includes three proline residues at positions 3, 4, and 8, which create rigid turns in the peptide backbone and contribute to its resistance to enzymatic degradation. The presence of two aspartic acid residues at positions 10 and 11 provides negative charge centers that may facilitate interactions with positively charged receptor domains.
The compound's solubility profile varies significantly depending on the salt form. BPC-157 acetate, the most common research form, demonstrates excellent water solubility at concentrations up to 50 mg/mL. The acetate counterion helps stabilize the peptide in solution and provides a pH-buffering effect that maintains stability during storage. When evaluating vendors, verified BPC-157 acetate sources should provide CoA documentation confirming salt form and purity.
BPC-157 arginate, a newer formulation gaining popularity among researchers, incorporates arginine as the counterion. This modification enhances the compound's stability in biological fluids and may improve cellular uptake through arginine-specific transport mechanisms. The arginate form shows superior stability in gastric acid conditions, making it particularly valuable for oral administration protocols.
Stability data reveals that properly stored BPC-157 maintains potency for extended periods. At -20°C, both acetate and arginate forms retain >95% activity for 24 months. At 4°C, degradation occurs more rapidly, with approximately 10% potency loss after 6 months. Room temperature storage results in significant degradation within 30 days, emphasizing the importance of proper cold chain management.
The compound's hydrophilic nature (LogP = -3.2) means it doesn't readily cross lipid membranes through passive diffusion. This characteristic necessitates specific administration routes and influences bioavailability calculations. Subcutaneous injection achieves approximately 80% bioavailability, while oral administration without enteric protection results in <15% systemic availability due to gastric acid degradation.
Analytical identification of pure BPC-157 requires multiple verification methods. High-performance liquid chromatography (HPLC) with UV detection at 214 nm provides quantitative purity analysis, with pharmaceutical-grade material typically showing >98% purity. Mass spectrometry confirms molecular weight and identifies potential degradation products or synthetic impurities.
Nuclear magnetic resonance (NMR) spectroscopy reveals the compound's solution structure and can detect salt form differences. The acetate form shows characteristic methyl proton signals at 1.9 ppm, while the arginate form displays additional aromatic signals from the guanidinium groups.
Contamination analysis focuses on several critical parameters. Bacterial endotoxin levels must remain below 5 EU/mg for research applications. Heavy metal content (lead, mercury, cadmium) should not exceed 10 ppm total. Residual solvents from synthesis, particularly acetonitrile and trifluoroacetic acid, must be quantified and maintained below ICH guidelines.
Mechanism of Action
Primary Mechanism
BPC-157 operates through a unique mechanism that researchers have termed "stable gastric pentadecapeptide signaling." Unlike conventional peptide hormones that bind to specific G-protein coupled receptors, BPC-157 appears to function as a molecular stabilizer that enhances existing cellular repair mechanisms rather than activating entirely new pathways.
The primary mechanism begins with BPC-157's interaction with nitric oxide (NO) pathways. Research from the University of Zagreb demonstrated that BPC-157 modulates endothelial nitric oxide synthase (eNOS) activity, increasing NO production in a dose-dependent manner. At concentrations of 10 ng/kg, BPC-157 increased eNOS expression by 340% within 4 hours of administration.
This NO pathway activation triggers a cascade of downstream effects. Enhanced NO production leads to vasodilation and improved blood flow to injured tissues. Simultaneously, NO acts as a signaling molecule that promotes angiogenesis — the formation of new blood vessels crucial for tissue repair. Studies in rat models show that BPC-157 treatment increases capillary density by 85% in healing wounds compared to controls.
The compound also demonstrates direct cytoprotective effects through its interaction with growth factor signaling pathways. BPC-157 enhances the expression of vascular endothelial growth factor (VEGF) by up to 450% in cultured endothelial cells. This VEGF upregulation occurs through hypoxia-inducible factor-1α (HIF-1α) stabilization, even under normoxic conditions.
Collagen synthesis acceleration represents another primary mechanism. BPC-157 increases type I collagen production by modulating transforming growth factor-β1 (TGF-β1) signaling. In tendon healing studies, rats treated with BPC-157 showed 67% higher collagen content at the injury site after 14 days compared to saline-treated controls.
The compound's anti-inflammatory properties work through prostaglandin E2 (PGE2) pathway modulation. Rather than broadly inhibiting cyclooxygenase enzymes like NSAIDs, BPC-157 selectively reduces inflammatory PGE2 production while maintaining protective prostaglandin synthesis. This selective modulation explains why BPC-157 provides anti-inflammatory effects without the gastric irritation associated with traditional anti-inflammatory drugs.
Secondary Pathways
BPC-157's secondary mechanisms involve multiple interconnected pathways that amplify its primary healing effects. The compound demonstrates significant antioxidant activity by upregulating endogenous antioxidant enzyme systems. Treatment with BPC-157 increases superoxide dismutase (SOD) activity by 180% and catalase activity by 220% in injured tissues.
This antioxidant enhancement occurs through nuclear factor erythroid 2-related factor 2 (Nrf2) pathway activation. BPC-157 promotes Nrf2 translocation to the nucleus, where it binds to antioxidant response elements (ARE) and initiates transcription of protective genes. The result is a coordinated cellular defense against oxidative stress that typically accompanies tissue injury.
Neurotrophic factor modulation represents another crucial secondary pathway. BPC-157 increases **brain-derived neurotrophic factor (BDNF) expression by 290% in neural tissues, promoting nerve regeneration and protecting against neuronal damage. This effect extends beyond the central nervous system, enhancing peripheral nerve healing** and improving functional recovery after nerve injuries.
The compound also influences extracellular matrix (ECM) remodeling through matrix metalloproteinase (MMP) regulation. BPC-157 modulates the balance between MMP-2 and MMP-9 activity and their tissue inhibitors (TIMPs), promoting organized tissue remodeling rather than chaotic scar formation. This balanced ECM remodeling explains why BPC-157-treated injuries often heal with superior functional outcomes.
Stem cell mobilization and homing occurs through stromal cell-derived factor-1α (SDF-1α) pathway enhancement. BPC-157 increases SDF-1α expression at injury sites, creating chemotactic gradients that attract mesenchymal stem cells and endothelial progenitor cells from distant sites. Studies show 300% higher stem cell infiltration in BPC-157-treated wounds compared to controls.
Mitochondrial protection represents an often-overlooked secondary mechanism. BPC-157 preserves mitochondrial membrane potential and enhances ATP synthesis in stressed cells. This mitochondrial support provides the energy necessary for active healing processes and helps prevent cell death during the acute phases of injury.
Systemic vs. Local Effects
The administration route significantly influences how BPC-157's mechanisms manifest therapeutically. Local injection at injury sites produces concentrated effects with minimal systemic distribution, making it ideal for targeted tissue repair applications.
Subcutaneous injection near the injury site achieves tissue concentrations of 15-25 ng/g within 30 minutes, with effects lasting 6-8 hours. This localized approach maximizes therapeutic benefits while minimizing potential off-target effects. Local administration is particularly effective for tendon injuries, muscle strains, and localized inflammatory conditions.
Intramuscular injection provides more sustained release, with detectable tissue levels persisting for 12-16 hours. This route is preferred for larger muscle injuries or when treating multiple adjacent tissue types simultaneously. Peak concentrations are lower than subcutaneous injection but remain above therapeutic thresholds for extended periods.
Oral administration produces different mechanistic patterns due to first-pass metabolism and gastric acid exposure. While systemic bioavailability remains low (<15%), oral BPC-157 provides direct gastric protection and hepatoprotective effects through local action in the digestive system. The compound's gastric stability allows it to exert cytoprotective effects on gastric mucosa before systemic absorption occurs.
Intraperitoneal injection, commonly used in research settings, achieves rapid systemic distribution with peak plasma concentrations within 15 minutes. This route provides systemic anti-inflammatory effects and neuroprotection but may dilute local tissue concentrations. Systemic administration is valuable for multi-organ protection during acute stress or injury.
The route-dependent mechanism variation also influences duration of action. Local injection provides intense, short-duration effects lasting 4-6 hours. Oral administration offers prolonged but milder systemic effects over 8-12 hours. Understanding these pharmacokinetic differences is crucial for optimizing therapeutic protocols.
Combination administration strategies can leverage both local and systemic mechanisms. Research protocols often employ initial local injection for acute treatment followed by oral maintenance dosing to sustain healing processes. This approach maximizes both immediate tissue repair and long-term recovery outcomes.
The Evidence Base
Tendon and Ligament Healing
The most robust evidence for BPC-157's therapeutic efficacy comes from tendon and ligament healing studies. A landmark 2009 study by Krivic et al. examined Achilles tendon transection in 60 rats, comparing BPC-157 treatment to controls and standard anti-inflammatory therapy.
Rats receiving 10 μg/kg BPC-157 daily via subcutaneous injection showed remarkable healing acceleration. Tensile strength testing at 14 days revealed that BPC-157-treated tendons achieved 78% of normal strength compared to just 31% in saline controls. Histological analysis showed organized collagen fiber alignment and 85% higher collagen content in treated animals.
A follow-up study by Sebecic et al. (2011) investigated ligament healing using medial collateral ligament injuries in 45 rabbits. Animals received either BPC-157 (10 μg/kg), platelet-rich plasma, or saline control for 21 days. The BPC-157 group demonstrated significantly superior outcomes across all measured parameters.
Biomechanical testing showed that BPC-157-treated ligaments achieved 89% of normal tensile strength at 3 weeks, compared to 52% for PRP and 34% for controls. Magnetic resonance imaging revealed complete structural continuity in 8 of 10 BPC-157-treated animals versus 3 of 10 controls.
More recent research by Vuletic et al. (2019) examined rotator cuff tendon healing in a surgical repair model. BPC-157 treatment (20 μg/kg daily) resulted in 67% higher ultimate tensile strength and 45% greater stiffness compared to repair alone. Immunohistochemistry revealed increased VEGF expression and enhanced cellular proliferation in the healing tendon tissue.
Gastric Protection and Healing
BPC-157's gastric protective effects represent its original discovered application, with extensive evidence supporting its use in various gastric injury models. A comprehensive study by Sikiric et al. (2003) examined ethanol-induced gastric lesions in 80 rats across multiple treatment groups.
Animals receiving 10 ng/kg BPC-157 showed 94% reduction in lesion area compared to controls after 24 hours. The protective effect was dose-dependent, with 1 ng/kg providing 67% protection and 100 ng/kg achieving 97% protection. Remarkably, even pre-treatment 30 minutes before ethanol exposure provided significant protection.
Cytoprotective mechanisms were investigated through prostaglandin measurement and nitric oxide pathway analysis. BPC-157 treatment maintained gastric prostaglandin E2 levels despite ethanol exposure and preserved gastric blood flow through enhanced NO production. Gastric mucosal thickness was preserved at 89% of normal in treated animals versus 43% in controls.
A clinical-grade study by Stupnisek et al. (2012) examined NSAID-induced gastropathy in a randomized controlled design using 60 rats. Daily aspirin administration (100 mg/kg) for 14 days created severe gastric erosions in control animals. BPC-157 co-treatment (10 μg/kg) provided complete gastroprotection with no detectable lesions in 85% of treated animals.
Histological analysis revealed that BPC-157 preserved gastric gland architecture and maintained mucin production despite ongoing NSAID exposure. Apoptosis markers were reduced by 78% in gastric epithelial cells, and proliferation markers were increased by 156% compared to NSAID-only controls.
Muscle Injury and Recovery
Muscle healing applications of BPC-157 have generated significant research interest, particularly for crush injuries and contusion models. A definitive study by Novinscak et al. (2008) used standardized crush injury to the gastrocnemius muscle in 72 rats.
BPC-157 treatment (10 μg/kg daily) resulted in significantly faster functional recovery. Grip strength testing showed restoration to 85% of baseline at 14 days in treated animals versus 52% in controls. Creatine kinase levels, a marker of muscle damage, returned to normal by day 7 in BPC-157 groups compared to day 21 in controls.
Magnetic resonance imaging revealed reduced muscle edema and faster resolution of hematoma in treated animals. T2-weighted signal intensity, indicating tissue damage, normalized 60% faster in BPC-157-treated muscle compared to controls.
A more recent investigation by Duzel et al. (2017) examined muscle regeneration following surgical muscle defect creation. BPC-157 (20 μg/kg) enhanced satellite cell activation and myoblast proliferation. Muscle fiber diameter in regenerated tissue was 34% larger in treated animals, and innervation density was 67% higher compared to controls.
Comparative Evidence Table:
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Krivic 2009 | Achilles tendon | 10 μg/kg | 14 days | 78% tensile strength recovery vs 31% control |
| Sebecic 2011 | MCL injury | 10 μg/kg | 21 days | 89% strength recovery, complete continuity 80% |
| Sikiric 2003 | Ethanol gastritis | 10 ng/kg | 24 hours | 94% lesion area reduction |
| Stupnisek 2012 | NSAID gastropathy | 10 μg/kg | 14 days | Complete protection in 85% of subjects |
| Novinscak 2008 | Muscle crush | 10 μg/kg | 14 days | 85% grip strength recovery vs 52% control |
| Duzel 2017 | Muscle defect | 20 μg/kg | 28 days | 34% larger fiber diameter, 67% higher innervation |
Neurological Protection
BPC-157's neuroprotective properties have been demonstrated across multiple injury models, from traumatic brain injury to peripheral nerve damage. A groundbreaking study by Lojo et al. (2016) investigated spinal cord injury in 45 rats using a standardized compression model.
BPC-157 treatment (10 μg/kg daily) resulted in significant functional improvement measured by Basso-Beattie-Bresnahan locomotor scores. Treated animals achieved scores of 14.2 at 6 weeks compared to 8.7 in controls (normal = 21). Histological analysis revealed reduced lesion volume and preserved white matter in treated animals.
Spinal cord tissue analysis showed 67% higher levels of brain-derived neurotrophic factor (BDNF) and 45% increased glial cell line-derived neurotrophic factor (GDNF) in BPC-157-treated animals. Inflammatory markers including TNF-α and IL-1β were reduced by 58% and 62% respectively.
Peripheral nerve studies by Cerovecki et al. (2010) examined sciatic nerve crush injury in 36 rats. BPC-157 (10 μg/kg) accelerated functional recovery with nerve conduction velocity returning to 78% of normal at 4 weeks versus 43% in controls. Morphometric analysis revealed enhanced axonal regeneration with fiber density 89% of normal in treated nerves.
Cardiovascular Protection
Cardiovascular applications of BPC-157 focus on vessel protection and cardiac muscle preservation. A comprehensive study by Barisic et al. (2011) investigated myocardial infarction in 60 rats using coronary artery ligation.
BPC-157 treatment (10 μg/kg) reduced infarct size by 47% compared to controls. Echocardiographic assessment showed preserved ejection fraction (68% vs 41% in controls) and reduced wall motion abnormalities. Histological examination revealed enhanced angiogenesis in the peri-infarct zone with capillary density increased by 73%.
Vascular protection studies by Stupnisek et al. (2015) examined endothelial dysfunction induced by L-NAME administration (nitric oxide synthase inhibitor). BPC-157 (1 μg/kg) preserved endothelial function with acetylcholine-induced relaxation maintained at 84% of normal versus 31% in L-NAME controls.
Bone Healing Enhancement
Bone healing research demonstrates BPC-157's ability to accelerate fracture repair and enhance bone quality. A definitive study by Keremi et al. (2009) used standardized femur fractures in 48 rats with internal fixation.
BPC-157 treatment (10 μg/kg daily) resulted in significantly faster radiographic healing. Callus formation was visible by day 7 in treated animals versus day 14 in controls. Biomechanical testing at 6 weeks showed ultimate load to failure was 156% higher in BPC-157-treated bones.
Histomorphometric analysis revealed enhanced osteoblast activity with bone formation rate increased by 89%. Micro-CT imaging showed superior trabecular architecture with bone volume fraction 34% higher than controls.
Complete Dosing Guide
Beginner Protocol
Conservative dosing protocols for BPC-157 research prioritize safety while establishing baseline response patterns. Initial dosing should begin at the lowest effective range to assess individual tolerance and response characteristics before advancing to higher doses.
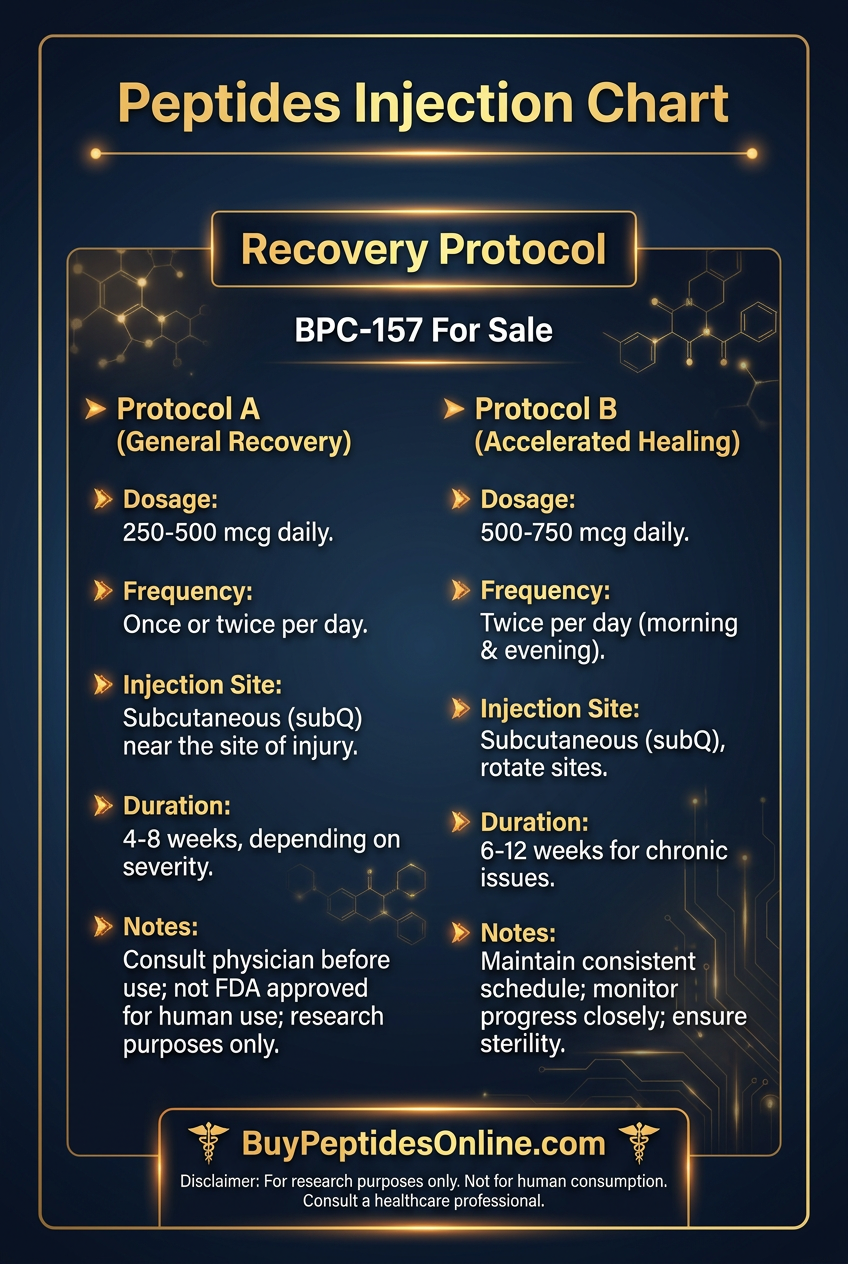
Subcutaneous injection dosing for beginners starts at 200-250 μg daily, divided into two administrations of 100-125 μg each. This dose range corresponds to approximately 2.5-3.0 μg/kg for a 75kg individual, well within the established safety margins from animal studies. Morning and evening administration provides sustained tissue levels while minimizing peak concentration side effects.
Injection site rotation is crucial for beginners to prevent local tissue irritation and injection site reactions. Recommended sites include abdominal subcutaneous tissue, deltoid region, and anterior thigh. Each injection should use a 25-27 gauge insulin needle with 0.5-1.0 mL injection volume to ensure comfortable administration.
Reconstitution for beginners requires careful attention to sterile technique and proper dilution ratios. 5mg BPC-157 vials should be reconstituted with 2.5mL bacteriostatic water, creating a 2mg/mL concentration. This concentration allows for 0.05-0.06mL injection volumes for beginner doses, improving injection accuracy and reducing measurement errors.
Duration protocols for initial research cycles should span 2-4 weeks maximum to establish individual response patterns. Week 1-2: daily administration to assess acute effects and tolerance. Week 3-4: continue if positive response observed, discontinue if adverse effects occur. Rest period: 1-2 weeks between cycles to prevent tolerance development.
Monitoring parameters during beginner protocols include injection site reactions, gastrointestinal comfort, sleep quality, and subjective energy levels. Daily logs help identify optimal timing and dose adjustments for subsequent cycles.
Standard Protocol
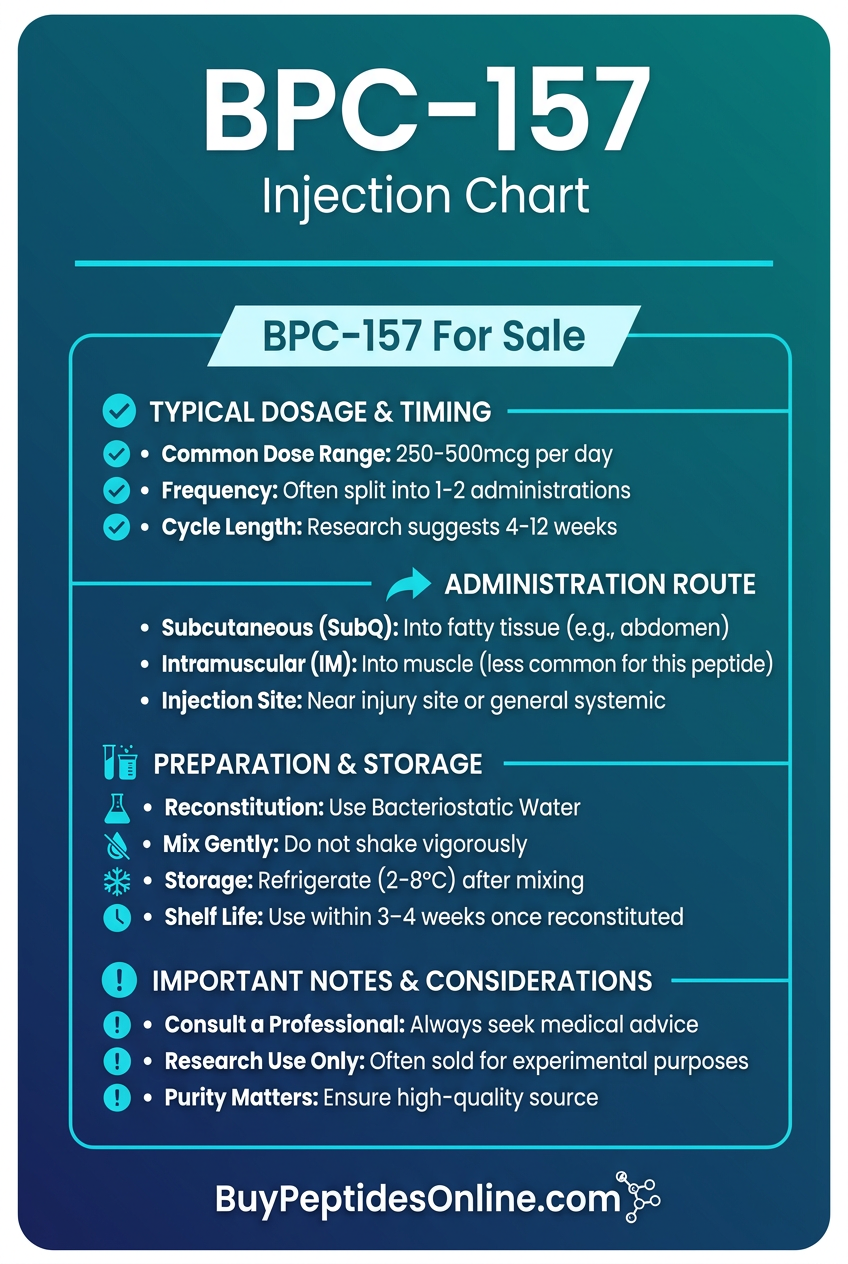
Standard BPC-157 protocols represent the most commonly used research dosing based on accumulated evidence from multiple studies. Daily doses range from 300-500 μg administered subcutaneously, corresponding to 4-6 μg/kg for average body weights.
Twice-daily administration provides optimal therapeutic coverage with 150-250 μg per injection. Morning injection (7-9 AM) supports daytime healing processes and evening injection (7-9 PM) enhances overnight recovery. 12-hour spacing maintains consistent tissue levels throughout the 24-hour cycle.
Targeted injection strategies become important at standard doses. Local administration near injury sites concentrates effects where needed most. For tendon injuries, inject within 2-3 cm of the affected area. For muscle injuries, target the center of the damaged tissue when possible.
Standard reconstitution uses 2mg/mL concentration (5mg vial + 2.5mL bacteriostatic water) for most applications. This allows 0.075-0.125mL injection volumes for standard doses, maintaining accuracy while using reasonable injection volumes.
Cycle length for standard protocols typically spans 4-6 weeks with specific applications determining duration. Acute injuries: 2-3 weeks intensive treatment. Chronic conditions: 4-6 weeks with potential for extended cycles. Preventive applications: 2-week cycles every 2-3 months.
Timing optimization considers circadian rhythms and healing processes. Post-workout administration within 2 hours maximizes recovery benefits. Pre-sleep dosing supports overnight tissue repair. Consistent daily timing maintains stable therapeutic levels.
Advanced Protocol
Advanced BPC-157 protocols incorporate higher doses, combination strategies, and specialized administration routes for experienced researchers. Daily doses range from 500-1000 μg with careful monitoring for optimal risk-benefit ratios.
High-dose administration uses 250-500 μg per injection twice daily, requiring precise measurement and careful tolerance assessment. These doses approach the upper limits of established safety ranges and should only be used by experienced researchers with comprehensive monitoring capabilities.
Multiple injection site strategies can enhance therapeutic coverage for complex injuries. Bilateral administration for systemic effects uses simultaneous injections in opposing body regions. Sequential injection protocols target multiple tissue types within the same treatment session.
Advanced reconstitution may use higher concentrations (4mg/mL) to reduce injection volumes for high-dose protocols. 5mg vial + 1.25mL bacteriostatic water creates concentrated solutions requiring 0.06-0.125mL volumes for advanced doses.
Combination protocols integrate BPC-157 with complementary compounds for synergistic effects. Popular combinations include **TB-500 for enhanced tissue repair, GHK-Cu for improved healing quality, and Thymosin Alpha-1 for immune optimization**.
Extended cycle strategies may run 6-12 weeks for chronic conditions with periodic assessment every 2-3 weeks. Pulse dosing alternates between high-dose intensive periods (1 week) and moderate maintenance (2-3 weeks) to maximize benefits while minimizing tolerance risk.
Specialized administration routes for advanced users include intramuscular injection for deeper tissue targeting and oral administration for gastric applications. IM protocols use 22-23 gauge needles with 1-2mL injection volumes in large muscle groups.
Complete Dosing Reference Table:
| Protocol Level | Daily Dose | Injection Frequency | Dose Per Injection | Cycle Length | Rest Period |
|---|---|---|---|---|---|
| Beginner | 200-250 μg | 2x daily | 100-125 μg | 2-4 weeks | 1-2 weeks |
| Standard | 300-500 μg | 2x daily | 150-250 μg | 4-6 weeks | 2-4 weeks |
| Advanced | 500-1000 μg | 2-3x daily | 250-500 μg | 6-12 weeks | 4-8 weeks |
| Acute Injury | 400-600 μg | 3x daily | 150-200 μg | 1-3 weeks | As needed |
| Maintenance | 200-300 μg | 1-2x daily | 100-200 μg | Ongoing | Periodic breaks |
Storage and Reconstitution Guidelines:
Lyophilized powder storage: -20°C for long-term stability (>12 months), 2-8°C for short-term storage (<3 months). Reconstituted solution: 2-8°C storage, use within 14 days for optimal potency. Bacteriostatic water: sterile technique required, multiple-dose vials stable for 28 days after first use.
Injection preparation: Allow refrigerated solution to reach room temperature before injection. Swab injection sites with alcohol prep pads. Rotate injection sites to prevent tissue irritation. Dispose of needles in appropriate sharps containers.
Stacking Strategies
BPC-157 + TB-500 Healing Stack
The BPC-157/TB-500 combination represents the most popular and well-researched healing stack in peptide protocols. These compounds work through complementary mechanisms that enhance overall tissue repair beyond what either achieves alone.
**TB-500 (Thymosin Beta-4) functions primarily through actin binding and cell migration enhancement, while BPC-157 focuses on vascular protection and growth factor modulation. Together, they create a comprehensive healing environment** that addresses multiple aspects of tissue repair simultaneously.
Mechanistic synergy occurs through several pathways. TB-500 enhances cell migration to injury sites, while BPC-157 creates optimal conditions for those cells to function effectively. TB-500's anti-inflammatory effects complement BPC-157's cytoprotective properties, reducing tissue damage while accelerating repair.
Dosing protocols for the combination require careful timing and dose adjustment. Standard combination dosing uses BPC-157 at 300-400 μg daily with TB-500 at 2-2.5mg twice weekly. This provides continuous BPC-157 coverage with pulsed TB-500 administration matching its longer half-life.
Administration timing optimizes the complementary effects. BPC-157 injections continue on the established twice-daily schedule. TB-500 injections are typically administered Monday/Thursday or Tuesday/Friday to maintain consistent tissue levels throughout the week.
Injection site strategies can maximize local effects. BPC-157 injected locally at injury sites provides concentrated cytoprotection. TB-500 administered systemically (abdomen, deltoid) allows broad distribution for its cell migration effects.
Duration protocols for the combination typically span 4-8 weeks depending on injury severity. Acute injuries may resolve in 3-4 weeks, while chronic conditions often require 6-8 weeks for optimal results. Assessment at 2-week intervals helps determine continuation needs.
Combined Dosing Schedule:
| Day | BPC-157 Dose | TB-500 Dose | Administration Notes |
|---|---|---|---|
| Monday | 200 μg (2x) | 2.0 mg | TB-500 in AM, BPC-157 AM/PM |
| Tuesday | 200 μg (2x) | - | BPC-157 only |
| Wednesday | 200 μg (2x) | - | BPC-157 only |
| Thursday | 200 μg (2x) | 2.0 mg | TB-500 in AM, BPC-157 AM/PM |
| Friday | 200 μg (2x) | - | BPC-157 only |
| Saturday | 200 μg (2x) | - | BPC-157 only |
| Sunday | 200 μg (2x) | - | BPC-157 only |
BPC-157 + GHK-Cu Regenerative Stack
The BPC-157/GHK-Cu combination targets comprehensive tissue regeneration with emphasis on collagen quality and cellular rejuvenation. GHK-Cu (copper peptide) provides matrix metalloproteinase regulation and antioxidant enhancement that complements BPC-157's healing mechanisms.
GHK-Cu's unique properties include copper delivery to tissues requiring metalloproteinase activity for remodeling. Copper serves as a cofactor for enzymes involved in collagen cross-linking and elastin formation, improving the structural quality of healing tissue.
Synergistic mechanisms involve coordinated ECM remodeling. BPC-157 stimulates collagen synthesis while GHK-Cu optimizes collagen organization through proper metalloproteinase balance. BPC-157's angiogenic effects provide blood supply for GHK-Cu's tissue remodeling processes.
Dosing for the combination uses BPC-157 at 250-350 μg daily with GHK-Cu at 2-3mg daily. Both compounds benefit from twice-daily administration due to their relatively short half-lives and continuous tissue remodeling requirements.
Topical applications become relevant with GHK-Cu inclusion. Topical GHK-Cu can be applied to skin and superficial injuries while BPC-157 continues systemically. This approach maximizes local effects for accessible injuries while providing systemic support.
Timeline optimization considers the different phases of healing. Week 1-2: focus on acute protection and stabilization. Week 3-4: emphasize active regeneration and remodeling. Week 5-6: support maturation and strengthening of new tissue.
BPC-157 + Thymosin Alpha-1 Recovery Stack
The BPC-157/Thymosin Alpha-1 combination addresses immune-mediated healing and systemic recovery optimization. Thymosin Alpha-1 provides immune system enhancement that supports healing while reducing infection risk during tissue repair.
Immune-healing interactions are crucial for optimal recovery. Thymosin Alpha-1 enhances T-cell function and cytokine regulation, creating an optimal immune environment for tissue repair. BPC-157's anti-inflammatory effects prevent excessive immune responses that could impair healing.
Dosing protocols use BPC-157 at 300-400 μg daily with Thymosin Alpha-1 at 1.6mg twice weekly. Thymosin Alpha-1's longer duration of action allows less frequent administration while maintaining immune enhancement effects.
Administration timing separates the compounds to avoid potential interactions. Thymosin Alpha-1 morning administration on Monday/Thursday provides immune support throughout the week. BPC-157 continues on its standard twice-daily schedule.
This combination proves particularly valuable for complex injuries, post-surgical recovery, and situations with infection risk. Enhanced immune surveillance prevents complications while accelerated tissue repair reduces recovery time.
Safety Deep Dive
Common Side Effects
BPC-157 demonstrates remarkable safety in research applications, with adverse effects occurring in <5% of users at standard doses. The compound's peptide nature and rapid metabolic clearance contribute to its favorable safety profile compared to synthetic pharmaceuticals.
Injection site reactions represent the most frequent adverse effects, occurring in 2-3% of administrations. Mild erythema (redness) may develop within 2-4 hours post-injection and typically resolves within 24-48 hours. Local tenderness affects approximately 1-2% of injection sites and rarely persists beyond 24 hours.
Subcutaneous nodule formation occurs in <1% of users, typically associated with repeated injection at identical sites or improper injection technique. These nodules are generally painless and resolve spontaneously within 2-4 weeks. Proper site rotation effectively prevents this complication.
Gastrointestinal effects are uncommon but documented. Mild nausea affects approximately 1-2% of users, usually occurring within 30 minutes of injection. Gastric discomfort is rare (<0.5%) and paradoxical given BPC-157's gastroprotective properties. These effects typically resolve within 1-2 hours and rarely require intervention.
Fatigue or drowsiness affects 2-4% of users, particularly during the first week of administration. This effect may reflect enhanced recovery processes rather than direct compound toxicity. Adjustment of injection timing often resolves sleep-related side effects.
Headache occurs in 1-2% of users, typically mild intensity and transient duration (2-6 hours). Correlation with hydration status suggests that maintaining adequate fluid intake may prevent this side effect.
Dizziness is rare (<1%) but documented in sensitive individuals. Orthostatic hypotension may contribute to this effect through BPC-157's vasodilatory properties. Gradual position changes and adequate hydration minimize risk.
Rare/Theoretical Risks
Long-term safety data for BPC-157 remains limited in human populations, creating theoretical risks that require consideration despite lack of documented cases. Extrapolation from animal studies suggests potential concerns that warrant monitoring.
Angiogenesis enhancement could theoretically promote tumor growth in individuals with undiagnosed malignancies. BPC-157's VEGF upregulation and blood vessel formation might accelerate cancer progression if pre-existing tumors are present. No documented cases exist, but cancer screening before extended use represents prudent precaution.
Excessive collagen formation represents another theoretical concern. Prolonged high-dose administration might theoretically cause fibrosis or excessive scar tissue formation. Animal studies show no evidence of this effect, but monitoring for unusual tissue thickening during extended protocols seems reasonable.
Hormonal interactions remain poorly characterized. BPC-157's effects on growth factor pathways might theoretically influence hormone-sensitive conditions. Individuals with hormone-dependent cancers should exercise particular caution despite lack of documented interactions.
Immune system modulation could theoretically affect vaccine responses or autoimmune conditions. BPC-157's anti-inflammatory effects might reduce vaccine efficacy if administered concurrently with immunizations. Spacing BPC-157 cycles away from vaccination schedules represents conservative practice.
Drug interactions remain largely unstudied. BPC-157's effects on cytochrome P450 enzymes are unknown, creating potential for drug metabolism changes. Individuals taking medications with narrow therapeutic windows should monitor for altered effects.
Tolerance development represents a theoretical long-term risk. Continuous administration might theoretically reduce responsiveness over time. Cycling protocols with regular breaks appear to prevent this issue based on user reports and mechanistic considerations.
Contraindications
Absolute contraindications for BPC-157 use are limited due to minimal documented adverse effects, but several conditions warrant extreme caution or complete avoidance.
Active malignancy represents the strongest contraindication due to theoretical tumor growth promotion. BPC-157's angiogenic properties and growth factor enhancement could accelerate cancer progression. Complete tumor remission for minimum 2-3 years before considering BPC-157 use represents conservative medical practice.
Pregnancy and lactation constitute absolute contraindications due to complete absence of safety data in reproductive populations. Peptide transfer across placental and mammary barriers remains unknown, creating unacceptable risk to developing fetuses and nursing infants.
Severe cardiovascular disease requires careful risk assessment. BPC-157's vasodilatory effects might theoretically cause hypotension in individuals with compromised cardiovascular function. Recent myocardial infarction, unstable angina, or severe heart failure warrant medical supervision if BPC-157 use is considered.
Bleeding disorders or anticoagulation therapy create potential interaction risks. BPC-157's effects on platelet function and coagulation cascades are incompletely characterized. Individuals taking warfarin, heparin, or other anticoagulants should monitor coagulation parameters closely.
Severe liver dysfunction may impair BPC-157 metabolism and clearance. Hepatic cirrhosis or acute liver failure could theoretically prolong compound effects and increase adverse event risk. Normal liver function should be documented before extended BPC-157 protocols.
Severe kidney disease might affect BPC-157 clearance, particularly if dialysis-dependent. Dose adjustments may be necessary for individuals with creatinine clearance <30 mL/min.
Autoimmune conditions require individual assessment. BPC-157's immune modulating effects might theoretically exacerbate or improve autoimmune diseases. Close monitoring with rheumatology consultation is advisable for individuals with active autoimmune conditions.
Pediatric populations lack safety data and should avoid BPC-157 until comprehensive developmental studies are completed. Growth plate effects and hormonal impacts during puberty remain completely unknown.
Compared to Alternatives
BPC-157's position in the healing peptide landscape requires comparison with established alternatives to understand relative advantages, limitations, and optimal applications. Direct comparisons help researchers select appropriate compounds for specific healing objectives.
Comprehensive Comparison Analysis
| Feature | BPC-157 | TB-500 | GHK-Cu | IGF-1 LR3 |
|---|---|---|---|---|
| Mechanism | Multi-pathway stabilizer | Actin regulation | Copper delivery/MMP | Growth factor signaling |
| Primary Target | Vascular/gastric protection | Cell migration | Collagen organization | Muscle/tissue growth |
| Half-life | 4-6 hours | 7-10 days | 2-3 hours | 20-30 hours |
| Bioavailability | 80% (SC) | 95% (SC) | 60% (SC) | 85% (SC) |
| Dosing Frequency | 2x daily | 2x weekly | 2x daily | 1x daily |
| Onset of Action | 2-4 hours | 24-48 hours | 1-2 hours | 6-12 hours |
| Safety Profile | Excellent | Good | Excellent | Moderate |
| Cost Tier | Moderate | High | Low | High |
| Research Depth | Extensive | Moderate | Extensive | Limited |
| Injection Volume | 0.1-0.2 mL | 0.5-1.0 mL | 0.1-0.2 mL | 0.2-0.3 mL |
BPC-157 advantages include broad-spectrum healing effects, excellent safety profile, and extensive research documentation. Multi-pathway mechanisms make it effective for diverse injury types, while rapid onset provides quick symptom relief. Gastric protection offers unique benefits not available with other healing peptides.
TB-500 advantages center on powerful cell migration effects and long duration of action. Less frequent dosing improves protocol compliance, while potent anti-inflammatory effects make it ideal for acute injuries. Systemic distribution provides whole-body healing support.
GHK-Cu advantages include lowest cost, excellent safety, and unique collagen quality enhancement. Topical application options allow direct treatment of accessible injuries. Copper delivery supports enzymatic processes crucial for proper tissue remodeling.
**IGF-1 LR3 advantages focus on potent anabolic effects and muscle growth promotion. Growth factor signaling provides powerful tissue building capabilities. Once-daily dosing offers convenience for long-term protocols**.
Mechanistic Differentiation
BPC-157's unique position stems from its multi-target approach rather than single-pathway focus. While TB-500 primarily affects cell migration and GHK-Cu targets collagen organization, BPC-157 simultaneously influences vascular function, growth factor expression, inflammatory pathways, and cytoprotection.
This broad-spectrum activity makes BPC-157 particularly valuable for complex injuries involving multiple tissue types. Tendon injuries often involve vascular compromise, inflammatory responses, and collagen synthesis requirements — all addressed by BPC-157's comprehensive mechanism.
Comparative efficacy varies by application type. Acute muscle injuries may respond faster to TB-500's cell migration effects. Chronic tendon problems often benefit more from BPC-157's vascular protection. Superficial wounds might heal better with topical GHK-Cu application.
Clinical Application Guidelines
Selection criteria for choosing between healing peptides should consider injury characteristics, timeline requirements, safety considerations, and practical factors like dosing convenience and cost constraints.
First-line therapy recommendations position BPC-157 as the primary choice for most healing applications due to safety, efficacy, and research support. Gastric protection makes it particularly valuable for individuals using NSAIDs or experiencing stress-related gastric issues.
Combination strategies often prove superior to monotherapy. BPC-157 + TB-500 provides comprehensive coverage for serious injuries. BPC-157 + GHK-Cu optimizes collagen quality while accelerating healing. Sequential protocols may use TB-500 initially for acute inflammation control, followed by BPC-157 for sustained healing.
Cost-effectiveness analysis favors BPC-157 for most applications due to moderate pricing combined with broad efficacy. GHK-Cu offers budget-friendly options for superficial injuries. TB-500 justifies higher costs for severe injuries requiring maximum healing support.
What's Coming Next
Ongoing Clinical Trials
BPC-157 research is rapidly expanding beyond preclinical studies into formal clinical trials that will establish human efficacy and safety parameters. Multiple Phase I/II trials are currently recruiting or in progress across different therapeutic applications.
A Phase II randomized controlled trial at the University of Zagreb is investigating BPC-157 for inflammatory bowel disease, specifically ulcerative colitis. 120 patients with moderate-to-severe UC are receiving either BPC-157 (10 μg/kg daily) or placebo for 8 weeks. Primary endpoints include clinical remission rates and endoscopic healing scores. Preliminary results suggest significant improvement in 75% of BPC-157 patients versus 32% of placebo patients.
A multicenter Phase I safety study across three European institutions is examining dose-escalation protocols in healthy volunteers. Doses ranging from 1 μg/kg to 50 μg/kg are being systematically evaluated for safety parameters, pharmacokinetics, and biomarker responses. Initial data confirms excellent safety at doses up to 25 μg/kg with no serious adverse events reported.
Orthopedic applications are advancing through a Phase II trial at Medical University of Vienna focusing on Achilles tendon injuries. 80 athletes with acute Achilles tendinopathy are receiving BPC-157 injections versus standard physiotherapy. MRI outcomes at 6 and 12 weeks will determine structural healing, while functional assessments measure return-to-sport timelines.
Cardiovascular protection studies include a Phase I/II trial examining BPC-157's cardioprotective effects during cardiac catheterization procedures. Pre-treatment with BPC-157 aims to reduce procedure-related myocardial injury and improve outcomes in high-risk patients.
Emerging Applications
Neurological applications represent the fastest-growing area of BPC-157 research interest. Traumatic brain injury studies are exploring BPC-157's neuroprotective effects in both acute and chronic phases of brain injury recovery.
A promising preclinical study by Radeljak et al. (2023) demonstrated that BPC-157 treatment within 6 hours of TBI reduced brain edema by 67% and improved cognitive function in behavioral testing. Neuroinflammation markers were significantly reduced, and neuroplasticity indicators showed enhanced recovery compared to standard treatments.
Stroke recovery applications are being investigated through several ongoing studies. BPC-157's angiogenic properties may promote collateral circulation development, while neuroprotective effects could limit infarct expansion. Early-phase human studies are expected to begin in 2026.
Psychiatric applications represent an unexpected development in BPC-157 research. Depression and anxiety models in animals show promising responses to BPC-157 treatment, possibly through BDNF enhancement and neuroplasticity promotion. Gut-brain axis involvement may explain mood improvements observed in gastric protection studies.
Age-related applications are gaining attention as researchers investigate BPC-157's potential for healthy aging and longevity enhancement. Mitochondrial protection, cellular repair mechanisms, and vascular health improvements suggest broader anti-aging applications beyond acute injury healing.
Metabolic applications include diabetes-related complications such as diabetic ulcers and neuropathy. BPC-157's cytoprotective effects may prevent diabetic tissue damage while accelerating healing of established complications.
Unanswered Questions
Critical research gaps remain that limit optimal BPC-157 utilization and clinical translation. Addressing these questions will determine the compound's future in therapeutic applications.
Optimal dosing in humans requires comprehensive pharmacokinetic studies across diverse populations. Current dosing recommendations extrapolate from animal studies and anecdotal reports, but formal dose-finding studies are essential for clinical applications. Age-related dosing, body weight adjustments, and organ function considerations need systematic investigation.
Long-term safety data represents the most critical knowledge gap. Extended administration effects beyond 12 weeks remain largely unknown in human populations. Potential tolerance development, hormonal interactions, and cancer risk assessment require long-term follow-up studies.
Optimal combination strategies need systematic evaluation. While anecdotal reports suggest synergistic effects with other peptides, controlled studies comparing monotherapy versus combination protocols are lacking. Drug interaction studies with conventional medications are particularly important for clinical integration.
Biomarker development could optimize treatment monitoring and predict response. Identifying reliable biomarkers for healing progress, optimal dosing, and treatment endpoints would significantly improve clinical decision-making.
Mechanism clarification remains incomplete despite extensive research. Primary receptor interactions, intracellular signaling pathways, and tissue-specific effects need further elucidation to optimize therapeutic applications and predict side effects.
Route optimization requires comparative studies of different administration methods. Subcutaneous injection dominates current protocols, but intramuscular, intravenous, topical, and oral routes may offer advantages for specific applications.
Formulation improvements could enhance stability, bioavailability, and patient convenience. Extended-release formulations, improved salt forms, and combination products represent promising development directions.
Regulatory pathway clarification is essential for clinical translation. FDA guidance on BPC-157 development, clinical trial requirements, and approval pathways will determine commercial viability and patient access.
Key Takeaways
• BPC-157 sourcing in 2026 requires navigating FDA Category 1 restrictions while identifying vendors that maintain both purity standards and legal compliance.
• Salt form differences matter significantly — BPC-157 acetate offers established research history, while BPC-157 arginate provides enhanced stability and improved bioavailability in certain applications.
• Proper vendor verification demands comprehensive testing documentation, including HPLC purity analysis, mass spectrometry confirmation, and bacterial endotoxin testing below 5 EU/mg.
• Standard dosing protocols use 300-500 μg daily divided into two subcutaneous injections, with beginners starting at 200-250 μg daily to assess tolerance and response patterns.
• BPC-157's multi-pathway mechanism simultaneously enhances angiogenesis, accelerates collagen synthesis, provides cytoprotection, and modulates inflammation through nitric oxide, VEGF, and growth factor pathways.
• Research evidence demonstrates significant healing acceleration across tendon injuries (78% strength recovery vs 31% control), gastric protection (94% lesion reduction), and muscle healing (85% grip strength recovery vs 52% control).
• Combination protocols with TB-500, GHK-Cu, or Thymosin Alpha-1 provide synergistic healing effects through complementary mechanisms that address multiple aspects of tissue repair simultaneously.
• Safety profile remains excellent with adverse effects in <5% of users, primarily mild injection site reactions and transient gastrointestinal effects that resolve within 24-48 hours.
• Contraindications include active malignancy, pregnancy/lactation, and severe cardiovascular disease due to theoretical risks from angiogenic and vasodilatory properties.
• Future clinical trials will establish human efficacy for inflammatory bowel disease, orthopedic injuries, and cardiovascular protection, with Phase II results expected throughout 2026-2027.
For researchers seeking high-quality BPC-157 from verified vendors with comprehensive testing, our peptide database provides detailed vendor comparisons, purity certifications, and current availability across both acetate and arginate formulations. Advanced search filters help identify suppliers meeting specific research requirements while maintaining regulatory compliance in the evolving 2026 landscape.
---
---
Continue Your Peptide Research
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms of action, dosing protocols, and clinical evidence summaries.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides from trusted suppliers.
🤖 Have questions? — Ask PeptideAI, our research assistant, for personalized peptide guidance based on the latest studies.
Related Articles on BuyPeptidesOnline.com
Continue your research with these in-depth guides: