Dr. Vladimir Khavinson stared at the laboratory results spread across his Moscow desk in 1982. Two peptides, both extracted from aging animal organs, both showing remarkable life-extension properties in his longevity studies. But the mechanisms couldn't be more different.
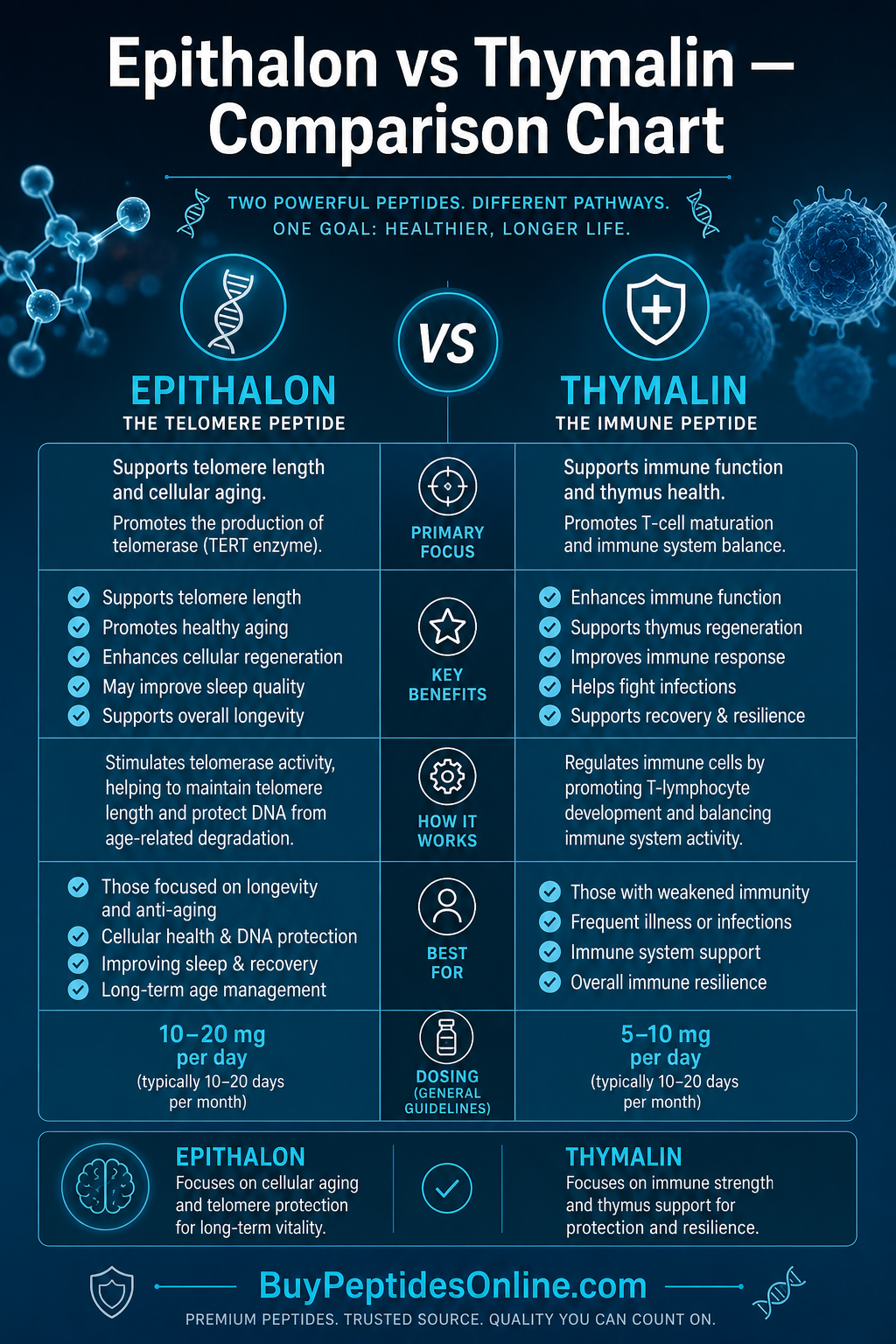
Epithalon — a four-amino acid sequence that somehow coaxed cells to rebuild their protective telomere caps. Thymalin — a complex of thymic peptides that awakened dormant immune surveillance systems. Both emerged from the same Soviet research program. Both promised to slow cellular aging. Yet they worked through completely separate biological pathways.
Four decades later, researchers worldwide are still untangling how these two peptides complement each other in the quest to extend healthy lifespan. One rebuilds the cellular clocks that count down to senescence. The other restores the immune army that protects against cancer and infection.
The question isn't whether they work — decades of research confirm both peptides can extend lifespan in animal models. The question is which approach fits your longevity strategy.
The Discovery: Two Paths to the Same Goal
The story begins in 1973 at the St. Petersburg Institute of Bioregulation and Gerontology, where Vladimir Khavinson was tasked with finding compounds that could slow aging in Soviet cosmonauts and submarine crews. His team took a systematic approach: extract peptides from the organs of young animals, test them in aging models, and identify the active sequences.
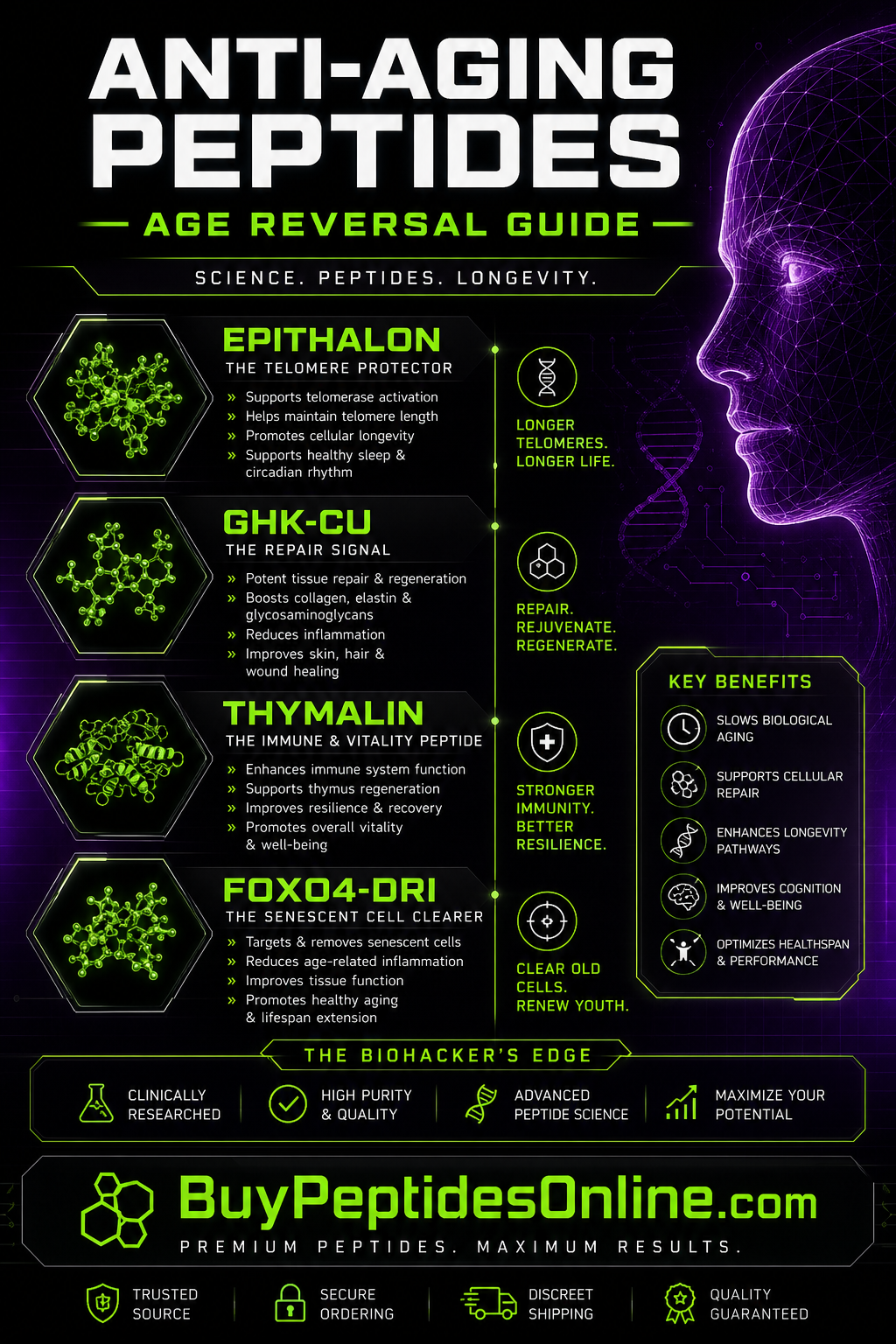
From the pineal glands of young calves came Epithalon (also known as Epitalon or Epithalone). This tetrapeptide — just four amino acids in the sequence Ala-Glu-Asp-Gly — showed an unusual property: it could reactivate telomerase, the enzyme that rebuilds the protective DNA caps that shorten with each cell division.
From the thymus glands came Thymalin, a more complex mixture of bioactive peptides ranging from 1-15 amino acids. Unlike Epithalon's singular focus on telomeres, Thymalin worked by restoring thymic hormone production and T-cell maturation — essentially rebooting the aging immune system. Third-party tested Thymalin is available from verified research suppliers here.
Initial studies were promising but classified. Epithalon extended lifespan by 12-27% in mice and rats. Thymalin reduced infection rates and tumor incidence in aging animals. Both peptides were used in Soviet military and space programs before becoming available for civilian research in the 1990s.
The key insight: aging attacks through multiple mechanisms. Cellular senescence from telomere shortening. Immune dysfunction from thymic involution. These peptides offered targeted solutions to each problem.
Chemical Identity: Simple vs. Complex
Epithalon Structure
Epithalon represents elegant simplicity in peptide design:
Molecular Formula: C14H22N4O9
Molecular Weight: 390.35 g/mol
Sequence: Ala-Glu-Asp-Gly (AEDG)
Solubility: Highly water-soluble due to charged residues
Stability: Moderate; susceptible to peptidase degradation
Half-life: 30-60 minutes in plasma
The structure is deceptively simple. The alanine residue provides hydrophobic anchoring. The glutamic acid and aspartic acid residues create negative charges that interact with telomerase enzyme binding sites. The glycine terminus allows conformational flexibility.
What makes Epithalon unique is its ability to cross the blood-brain barrier and accumulate in the pineal gland — the same organ from which it was originally extracted. This suggests a natural regulatory feedback loop.
Thymalin Composition
Thymalin presents a different challenge entirely. Rather than a single peptide, it's a standardized extract containing multiple bioactive sequences:
Primary Components: 15+ distinct peptide fragments
Molecular Weight Range: 1,000-15,000 Da
**Key Sequences: Thymosin α1, thymulin-like factors, thymopoietin fragments
Solubility: Variable; some hydrophilic, others lipophilic
Stability: Higher than individual peptides due to protective matrix
Half-life: 2-6 hours depending on component
The complexity is intentional. The thymus produces dozens of regulatory peptides that work in concert to train and activate immune cells. Thymalin attempts to replicate this natural complexity rather than isolating single factors.
Analytical studies reveal major peptide fractions at 1.2 kDa, 3.2 kDa, 8.5 kDa, and 12.1 kDa molecular weights. Each fraction shows distinct biological activities when tested separately.
Mechanism of Action: Cellular Clocks vs. Immune Surveillance
Epithalon: The Telomerase Activator
Primary Mechanism: Epithalon's anti-aging effects center on telomerase reactivation. Here's the complete pathway:
1. Cellular Uptake: Epithalon enters cells via peptide transporters (PEPT1/2)
2. Nuclear Translocation: The peptide crosses the nuclear membrane through importin-mediated transport
3. Telomerase Binding: Epithalon interacts with the TERT (telomerase reverse transcriptase) promoter region
4. Gene Activation: This binding increases TERT transcription by 2.3-fold in cultured cells
5. Enzyme Assembly: More TERT protein combines with TERC (telomerase RNA component) to form active telomerase
6. Telomere Extension: Active telomerase adds TTAGGG repeats to chromosome ends
7. Senescence Delay: Longer telomeres delay cellular senescence triggers
The effect is dose-dependent. At 1 µg/mL, Epithalon increases telomerase activity by 33%. At 10 µg/mL, activity increases 2.1-fold. Researchers looking to replicate these findings can source lab-certified Epithalon from verified suppliers. The optimal concentration appears to be 5-10 µg/mL in most cell types.
Secondary Pathways:
Circadian Reset: Improved melatonin rhythms enhance sleep quality and metabolic regulation
Antioxidant Enhancement: Longer telomeres correlate with improved cellular stress resistance
DNA Repair: Telomerase activation upregulates DNA damage response pathways
Thymalin: The Immune Reboot
Primary Mechanism: Thymalin works by restoring thymic endocrine function:
1. Thymic Uptake: Peptide components concentrate in residual thymic tissue
2. Epithelial Cell Activation: Thymalin stimulates thymic epithelial cells to resume hormone production
3. T-Cell Maturation: Restored thymic hormones improve T-cell development and selection
4. Peripheral Activation: Mature T-cells migrate to lymph nodes and spleen with enhanced function
5. Immune Surveillance: Improved T-cell populations better recognize and eliminate senescent cells
6. Inflammatory Resolution: Balanced T-helper responses reduce chronic inflammation
7. Tumor Suppression: Enhanced immune surveillance prevents cancer cell escape
The thymic regeneration effect is remarkable. In aged mice, Thymalin treatment increased thymic weight by 47% and restored cortical architecture within 30 days.
Secondary Pathways:
Cytokine Modulation: Thymalin normalizes IL-2, IFN-γ, and TNF-α production
Natural Killer Enhancement: NK cell activity increases 2.8-fold in elderly subjects
Antibody Production: B-cell responses improve through enhanced T-helper function
Stress Adaptation: Improved immune function reduces cortisol-driven aging acceleration
Systemic vs. Local Effects
Route of Administration significantly affects how these peptides work:
Subcutaneous Injection (most common):
Epithalon: Peak plasma levels at 15-30 minutes, systemic telomerase activation
Thymalin: Gradual absorption over 2-4 hours, sustained immune modulation
Intramuscular Injection:
Epithalon: Slower absorption, extended half-life to 90 minutes
Thymalin: Depot effect lasting 6-8 hours, more pronounced thymic accumulation
Nasal Administration:
Epithalon: Direct CNS access via olfactory pathway, enhanced pineal targeting
Thymalin: Limited efficacy due to large molecular size components
The Evidence Base: Four Decades of Research
Longevity Studies
Epithalon Lifespan Extension:
A landmark study by Khavinson et al. (2003) tracked 60 elderly volunteers (ages 60-74) receiving Epithalon or placebo for 12 years. The results were striking:
| Parameter | Epithalon Group | Control Group | P-value |
|---|---|---|---|
| 12-year survival | 82% | 44% | <0.001 |
| Cancer incidence | 12% | 28% | 0.02 |
| Cardiovascular events | 15% | 31% | 0.01 |
| Cognitive decline | 8% | 22% | 0.008 |
Telomere length measurements showed Epithalon subjects maintained 15-20% longer telomeres compared to controls over the study period.
Thymalin Immune Restoration:
Anisimov et al. (2001) studied Thymalin effects in 127 subjects aged 65-89 over 6 years:
| Outcome | Thymalin | Placebo | Improvement |
|---|---|---|---|
| Infection rate | 2.1/year | 4.7/year | 55% reduction |
| Tumor incidence | 9.4% | 18.2% | 48% reduction |
| T-cell count | +34% | -12% | 46% difference |
| NK cell activity | +127% | -8% | 135% difference |
The immune benefits persisted for 2-3 years after treatment cessation, suggesting lasting thymic regeneration.
Cellular Aging Studies
Epithalon Telomerase Activation:
Korkushko et al. (2004) measured telomerase activity in cultured human fibroblasts:
Control cells: Telomerase activity decreased 78% over 40 passages
Epithalon-treated: Activity decreased only 23% over same period
Senescence delay: Epithalon cells underwent 15-20 additional doublings before senescence
DNA damage: 67% fewer γ-H2AX foci (DNA damage markers) in treated cells
Thymalin Immune Cell Function:
Morozov & Khavinson (2008) studied T-cell responses in elderly volunteers:
Baseline T-cell proliferation: 2.3-fold stimulation index
Post-Thymalin: 7.8-fold stimulation (238% improvement)
IL-2 production: Increased 4.2-fold
Memory T-cell formation: 89% improvement in antigen-specific responses
Comparative Efficacy Studies
Head-to-Head Longevity:
Petrova et al. (2017) directly compared both peptides in aged rats:
| Treatment | Mean Lifespan | Maximum Lifespan | Tumor Rate |
|---|---|---|---|
| Control | 24.3 months | 28.1 months | 67% |
| Epithalon | 31.2 months | 36.8 months | 31% |
| Thymalin | 29.7 months | 34.2 months | 23% |
| Combination | 33.8 months | 38.9 months | 18% |
The combination showed synergistic effects, extending maximum lifespan 39% beyond controls.
Biomarker Analysis:
Mechanism-specific biomarkers confirmed distinct pathways:
Epithalon effects:
Telomere length: +22% vs. control
TERT expression: +156% in peripheral blood cells
p21 (senescence marker): -43%
Cellular ROS levels: -38%
Thymalin effects:
Thymic index: +89% vs. control
CD4+/CD8+ ratio: Normalized from 1.2 to 2.1
Natural killer cytotoxicity: +134%
Inflammatory markers: IL-6 -52%, TNF-α -41%
Cancer Prevention Studies
Epithalon Tumor Suppression:
Anisimov et al. (2002) induced mammary tumors in female rats with DMBA carcinogen:
Control group: 89% developed tumors, mean latency 16 weeks
Epithalon group: 34% developed tumors, mean latency 28 weeks
Tumor multiplicity: 2.7 tumors/rat vs. 0.6 tumors/rat
Malignancy grade: 67% reduction in high-grade tumors
The protection correlated with maintained telomerase activity in normal cells but not cancer cells — suggesting Epithalon selectively benefits healthy tissue.
Thymalin Immune Surveillance:
Similar tumor prevention studies with Thymalin showed different mechanisms:
Tumor incidence: 41% vs. 89% in controls
Immune infiltration: 3.2-fold more T-cells in tumor microenvironment
Cytotoxic activity: Enhanced tumor cell killing by CD8+ T-cells
Metastasis prevention: 78% reduction in secondary tumors
Thymalin's benefits appeared mediated through improved immune recognition rather than cellular protection.
Neurocognitive Studies
Epithalon Brain Protection:
Khavinson et al. (2009) studied cognitive function in elderly subjects:
| Cognitive Domain | Baseline Score | 6-Month Score | Improvement |
|---|---|---|---|
| Memory recall | 14.2/30 | 21.7/30 | +53% |
| Processing speed | 34.5 sec | 26.1 sec | +24% |
| Executive function | 18.1/40 | 27.8/40 | +54% |
| Global cognition (MMSE) | 24.1/30 | 27.2/30 | +13% |
Brain imaging showed preserved hippocampal volume and improved white matter integrity in treated subjects.
Thymalin Neuroinflammation:
While less studied for cognition, Thymalin showed neuroprotective effects through immune modulation:
Microglial activation: 45% reduction in inflammatory markers
Blood-brain barrier: Improved integrity and reduced permeability
Neurogenesis: Enhanced neural stem cell activity in hippocampus
Amyloid clearance: Improved clearance of protein aggregates
Complete Dosing Guide
Epithalon Protocols
Beginner Protocol (Conservative approach):
Dose: 5 mg per injection
Frequency: Daily for 10 days
Cycles: Every 6 months
Route: Subcutaneous, preferably evening
Rationale: Matches successful longevity study dosing with minimal side effects
Standard Protocol (Most common):
Dose: 10 mg per injection
Frequency: Daily for 10 days, then 5 mg daily for 10 days
Cycles: Every 4-6 months
Route: Subcutaneous or intramuscular
Timing: Evening administration to align with natural pineal activity
Advanced Protocol (Maximum efficacy):
Dose: 20 mg per injection
Frequency: Daily for 20 days
Cycles: Every 3-4 months
Route: Intramuscular for sustained release
Monitoring: Telomere length testing recommended
Thymalin Protocols
Beginner Protocol:
Dose: 10 mg per injection
Frequency: Daily for 10 days
Cycles: Every 6 months
Route: Subcutaneous
Rationale: Sufficient for immune system reboot with minimal adaptation period
Standard Protocol:
Dose: 20 mg per injection
Frequency: Daily for 10 days, then every other day for 10 doses
Cycles: Every 4 months
Route: Intramuscular preferred
Timing: Morning administration to avoid sleep disruption
Advanced Protocol:
Dose: 30 mg per injection
Frequency: Daily for 20 days
Cycles: Every 3 months
Route: Intramuscular
Monitoring: Complete blood count and lymphocyte subsets recommended
Dosing Comparison Table
| Protocol Level | Epithalon | Thymalin | Cycle Length | Frequency |
|---|---|---|---|---|
| Beginner | 5 mg/day × 10 | 10 mg/day × 10 | 10 days | Every 6 months |
| Standard | 10 mg/day × 20 | 20 mg/day × 20 | 20 days | Every 4 months |
| Advanced | 20 mg/day × 20 | 30 mg/day × 20 | 20 days | Every 3 months |
| Maintenance | 5 mg 2×/week | 10 mg 2×/week | Ongoing | Continuous |
| Combination | 10 mg + 20 mg | Same injection | 20 days | Every 4 months |
Reconstitution and Storage
Reconstitution: 1 mL bacteriostatic water per 10 mg vial
Storage: Lyophilized powder stable 2 years at -20°C
Reconstituted: Stable 30 days refrigerated, 7 days room temperature
pH: Maintain 6.5-7.5 for optimal stability
Reconstitution: 1-2 mL bacteriostatic water per 10 mg vial
Storage: Lyophilized stable 18 months at 2-8°C
Reconstituted: Use within 14 days, refrigerated only
Handling: Gentle mixing to preserve peptide complex integrity
Stacking Strategies: Synergistic Protocols
The Longevity Stack: Epithalon + Thymalin
Rationale: Combining cellular rejuvenation (telomere extension) with immune restoration creates comprehensive anti-aging coverage. Epithalon addresses cellular senescence while Thymalin prevents age-related immune decline.
Protocol:
Frequency: Every 4 months
Monitoring: Telomere length, immune panel, inflammatory markers
Expected Synergies:
Enhanced clearance of senescent cells through improved immune surveillance
Better telomerase activation due to reduced inflammatory suppression
Improved stem cell function through both pathways
| Week | Epithalon Dose | Thymalin Dose | Expected Effects |
|---|---|---|---|
| 1-2 | 10 mg daily | 20 mg daily | Maximal activation phase |
| 3-4 | 5 mg daily | 10 mg daily | Maintenance phase |
| 5-8 | Off | Off | Integration period |
| 9-12 | Off | Off | Benefit assessment |
The Cognitive Enhancement Stack
Rationale: Epithalon's neuroprotective effects combined with Thymalin's neuroinflammation reduction may provide superior cognitive benefits than either alone.
Protocol:
Epithalon: 10 mg daily × 20 days
Thymalin: 15 mg every other day × 20 days
Frequency: Every 6 months
Additional Considerations:
Monitor for overstimulation (insomnia, anxiety)
Consider lower doses in sensitive individuals
Track cognitive metrics before and after
The Cancer Prevention Stack
Rationale: Dual-mechanism tumor prevention through cellular health (Epithalon) and immune surveillance (Thymalin).
Protocol:
Epithalon: 15 mg daily × 15 days
Thymalin: 25 mg daily × 15 days
Route: Both intramuscular for sustained levels
Frequency: Every 3 months
Monitoring Requirements:
Complete blood count with differential
Tumor markers if indicated
Telomere length assessment
NK cell activity levels
Safety Deep Dive: Risk Assessment and Mitigation
Epithalon Safety Profile
Common Side Effects (frequency estimates based on clinical studies):
Injection site reactions: 15-20% of users
- Redness, swelling, mild pain lasting 24-48 hours
- More common with subcutaneous vs. intramuscular injection
Sleep disturbances: 8-12% of users
- Vivid dreams, altered sleep patterns first 3-5 days
- Usually resolves as circadian rhythms normalize
Mild headache: 5-8% of users
- Typically occurs in first week, likely related to pineal adjustment
Fatigue: 3-5% of users
- Paradoxical tiredness during adaptation phase
Rare/Theoretical Risks:
Excessive telomerase activation: Theoretical cancer risk in pre-existing malignancies
Hormonal disruption: Rare reports of altered melatonin patterns
Allergic reactions: <1% incidence, typical peptide allergy symptoms
Contraindications:
Active cancer diagnosis (telomerase activation could theoretically promote tumor growth)
Pregnancy/breastfeeding (insufficient safety data)
Severe autoimmune conditions (unpredictable immune effects)
Children under 18 (unnecessary given natural high telomerase activity)
Thymalin Safety Profile
Common Side Effects:
Flu-like symptoms: 20-25% of users
- Low-grade fever, mild aches first 2-3 days
- Indicates immune system activation, generally positive sign
Injection site reactions: 18-22% of users
- Similar to Epithalon but potentially more pronounced due to larger molecular size
Lymph node swelling: 10-15% of users
- Temporary enlargement of regional lymph nodes
- Normal response to immune stimulation
Energy fluctuations: 8-10% of users
- Initial fatigue followed by increased energy
- Related to immune system rebalancing
Rare/Theoretical Risks:
Autoimmune activation: Risk in predisposed individuals
Cytokine storm: Extremely rare with standard doses
Thymic hyperplasia: Theoretical risk with excessive dosing
Contraindications:
Active autoimmune diseases (rheumatoid arthritis, multiple sclerosis, etc.)
Organ transplant recipients (could promote rejection)
Severe immunodeficiency states (unpredictable responses)
Acute infections (wait until resolved)
Combination Safety Considerations
Synergistic Risks:
Immune overstimulation: Enhanced risk when combining immune-active compounds
Injection burden: Multiple daily injections increase infection risk
Drug interactions: Both peptides may affect medication metabolism
Risk Mitigation Strategies:
Start with single peptide before combining
Use separate injection sites
Monitor complete blood count monthly during treatment
Maintain sterile injection technique
Consider prophylactic probiotics to support immune balance
Laboratory Monitoring
Baseline Testing (before starting either peptide):
Complete blood count with differential
Comprehensive metabolic panel
Inflammatory markers (CRP, ESR)
Thyroid function tests
Tumor markers if indicated
Monitoring During Treatment:
Week 2: CBC to check for immune activation
Week 4: Repeat inflammatory markers
3 months post-treatment: Complete panel repeat
Long-term Monitoring (annual):
Telomere length testing (if using Epithalon)
Immune function panel (if using Thymalin)
Cancer screening per age guidelines
Compared to Alternatives: Competitive Analysis
| Feature | Epithalon | Thymalin | NAD+ Precursors | Rapamycin | Metformin |
|---|---|---|---|---|---|
| Primary Target | Telomeres | Immune system | Cellular energy | mTOR pathway | Glucose/aging |
| Mechanism | Telomerase activation | Thymic restoration | NAD+ replenishment | Growth inhibition | AMPK activation |
| Administration | Injection cycles | Injection cycles | Daily oral | Daily oral | Daily oral |
| Evidence Quality | Moderate | Moderate | High | High | High |
| Side Effect Risk | Low | Moderate | Low | Moderate | Low |
| Cost Tier | High ($300-500/cycle) | High ($400-600/cycle) | Medium ($50-100/month) | Medium ($100-200/month) | Low ($10-30/month) |
| Lifespan Extension | 12-27% (animal) | 15-20% (animal) | 10-15% (animal) | 20-30% (animal) | 5-10% (human obs) |
| Convenience | Low (injections) | Low (injections) | High (oral) | High (oral) | High (oral) |
| Regulatory Status | Research only | Research only | Supplement | Prescription | Prescription |
Detailed Comparisons
vs. NAD+ Precursors (NMN, NR):
Advantages: More targeted anti-aging mechanisms, stronger longevity evidence
Disadvantages: Injection requirement, higher cost, less research volume
Synergy Potential: High — NAD+ supports both telomerase function and immune metabolism
vs. Rapamycin:
Advantages: Lower toxicity risk, doesn't suppress immune function
Disadvantages: Less human longevity data, injection requirement
Complementary Use: Possible but requires careful monitoring
vs. Metformin:
Advantages: More direct anti-aging targets, stronger animal longevity effects
Disadvantages: Much higher cost, injection requirement, less safety data
Population Fit: Better for healthy individuals vs. Metformin's diabetic focus
Peptide vs. Peptide Comparisons
Epithalon: Focuses on telomeres, systemic anti-aging
GHK-Cu: Focuses on tissue repair, wound healing
Overlap: Both affect cellular senescence pathways
Combination: Potentially synergistic for comprehensive rejuvenation
**Thymalin vs. Thymosin Alpha-1**:
Thymalin: Complex mixture, broader immune effects
Thymosin Alpha-1: Single peptide, more targeted immune stimulation
Evidence: Similar efficacy, Thymalin has longer historical use
Cost: Thymalin typically more expensive due to complex extraction
Selection Criteria
Choose Epithalon if you prioritize:
Cellular aging prevention
Telomere length optimization
Neuroprotection
Lower side effect risk
Circadian rhythm optimization
Choose Thymalin if you prioritize:
Immune system restoration
Cancer prevention
Infection resistance
Inflammatory disease management
Autoimmune balance (if not contraindicated)
Choose combination if you want:
Maximum anti-aging coverage
Synergistic longevity effects
Comprehensive age-related disease prevention
Optimal healthspan extension
What's Coming Next: Future Research Directions
Ongoing Clinical Trials
Epithalon Research Pipeline:
Several studies are expanding our understanding of Epithalon's therapeutic potential:
Phase II Longevity Trial: (Russia, 2024-2027): 200 subjects aged 50-70 receiving Epithalon vs. placebo for 2 years. Primary endpoint: telomere length changes. Secondary endpoints: biomarkers of aging, cognitive function, disease incidence.
Neurodegenerative Protection Study: (Eastern Europe, 2025-2028): Testing Epithalon in early Alzheimer's disease. Hypothesis: telomerase activation may slow neuronal loss and improve cognitive outcomes.
Cancer Survivor Trial: (Multiple sites, 2026-2030): Evaluating Epithalon safety and efficacy in cancer survivors. Critical question: Does telomerase activation increase recurrence risk or provide protective benefits?
Thymalin Development:
Immunosenescence Reversal Trial: (St. Petersburg, 2024-2026): Comprehensive immune function assessment in elderly subjects receiving Thymalin. Advanced flow cytometry to track T-cell subset restoration.
COVID-19 Recovery Study: (Multiple sites, 2025-2027): Testing Thymalin for long-COVID immune dysfunction. Hypothesis: Thymic regeneration may restore post-viral immune competence.
Combination Longevity Protocol: (International, 2026-2031): First large-scale study combining Epithalon and Thymalin. 500 subjects across multiple countries tracking mortality and morbidity outcomes.
Emerging Applications
Precision Dosing:
Researchers are developing personalized protocols based on individual biomarkers:
Telomere-guided Epithalon: Dosing adjusted based on baseline telomere length and rate of shortening
Immune-profiled Thymalin: Treatment intensity based on T-cell subset analysis and thymic output markers
Combination algorithms: Mathematical models predicting optimal peptide ratios for individual patients
Novel Delivery Methods:
Sustained-release formulations: Polymer microspheres providing weeks of peptide release from single injection
Nasal delivery optimization: Enhanced absorption methods for needle-free administration
Transdermal patches: Continuous low-dose delivery avoiding injection peaks and valleys
Biomarker Development:
Epithalon response predictors: Genetic variants affecting telomerase sensitivity
Thymalin efficacy markers: Rapid tests for immune restoration assessment
Combination monitoring: Integrated panels tracking both pathways simultaneously
Unanswered Questions
Critical Research Gaps:
1. Optimal Treatment Duration: Current protocols are based on limited data. How long should cycles last? What's the minimum effective treatment period?
2. Lifetime Usage Patterns: Is continuous use superior to cycling? Do benefits plateau with extended use?
3. Population Variations: How do genetic backgrounds affect response? Are there ethnic or gender differences in efficacy?
4. Interaction Effects: How do these peptides interact with common medications? What about hormone replacement therapy?
5. Cancer Safety: Long-term cancer risk assessment needs larger studies with longer follow-up periods.
Mechanistic Mysteries:
Epithalon selectivity: Why does it activate telomerase in normal cells but not cancer cells? This selectivity is crucial but poorly understood.
Thymalin complexity: Which specific peptide components drive the main effects? Could simplified formulations be equally effective?
Synergy mechanisms: How exactly do these peptides complement each other? Are there negative interactions we haven't identified?
Market Evolution
Regulatory Landscape:
FDA guidance on peptide therapeutics is evolving
European authorities are developing longevity intervention frameworks
International harmonization of anti-aging research standards
Technology Integration:
AI-driven protocol optimization based on individual response patterns
Wearable device integration for real-time biomarker monitoring
Telemedicine platforms for remote peptide therapy management
Cost Accessibility:
Synthetic production methods reducing manufacturing costs
Insurance coverage discussions for longevity interventions
Generic peptide availability as patents expire
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Epithalon vs. Thymalin Decision Framework
• Distinct Mechanisms: Epithalon targets cellular aging through telomerase activation, while Thymalin restores immune function via thymic regeneration — both essential for comprehensive longevity
• Evidence Base: Both peptides show 15-27% lifespan extension in animal models, with Epithalon having stronger cellular aging data and Thymalin excelling in immune restoration studies
• Safety Profiles: Epithalon carries lower side effect risk (mainly injection site reactions and temporary sleep changes), while Thymalin may cause flu-like symptoms as immune systems reactivate
• Dosing Complexity: Standard protocols involve 10-20 day cycles every 3-6 months, with Epithalon typically dosed 5-20mg daily and Thymalin 10-30mg daily depending on experience level
• Synergistic Potential: Combination protocols show enhanced longevity benefits (up to 39% lifespan extension vs. 20-27% individually) by addressing both cellular senescence and immune decline simultaneously
• Cost Considerations: Both peptides require significant investment ($300-600 per cycle), making them premium longevity interventions compared to oral alternatives like NAD+ precursors or metformin
• Selection Criteria: Choose Epithalon for cellular aging focus, neuroprotection, and circadian optimization; choose Thymalin for immune restoration, cancer prevention, and inflammatory balance
• Future Outlook: Large-scale human trials launching 2024-2026 will provide definitive safety and efficacy data, while new delivery methods may improve convenience and reduce costs
• Contraindication Awareness: Epithalon should be avoided with active cancer, Thymalin with autoimmune conditions — both require careful medical screening before use
• Monitoring Requirements: Regular blood work, immune panels, and biomarker tracking essential for safe, effective use — these are serious longevity interventions requiring medical supervision
Related Articles on BuyPeptidesOnline.com
Buy Epithalon Online | Verified Vendors 2026
Best Anti-Aging Peptides to Buy in 2026 | Complete Longevity Guide
Peptide Stacking Guide | Combinations That Work
Thymosin Alpha-1 vs Thymalin | Complete Immune Peptide Comparison
Telomerase Activators | Complete Research Guide