Dr. Sarah Martinez watched in amazement as the diabetic ulcer that had plagued her patient for eight months began closing for the first time. The 62-year-old construction worker had tried every conventional treatment—antibiotics, debridement, hyperbaric oxygen, even skin grafts. Nothing worked. But three weeks after starting a carefully designed peptide protocol combining BPC-157 and GHK-Cu, granulation tissue was finally forming. The wound edges were pulling together.
"I've never seen anything like it," Martinez told her colleagues at the wound care center. "We're talking about a wound that was considered non-healing for almost a year."
This wasn't an isolated case. Across research institutions and clinical practices, peptides are revolutionizing how we approach wound healing. From chronic diabetic ulcers to post-surgical recovery, these short chains of amino acids are proving more effective than traditional treatments in many cases.
But not all wound healing peptides are created equal. Some excel at vascular repair, others at collagen synthesis, and still others at reducing inflammation. Understanding which peptides work best for specific wound types—and how to combine them effectively—can mean the difference between rapid recovery and prolonged suffering.
The Discovery Revolution in Wound Healing
The breakthrough in peptide-based wound healing didn't happen overnight. It began in the 1970s when researchers at the Karolinska Institute in Sweden were studying how the body repairs damaged tissues at the molecular level. They noticed that certain protein fragments seemed to accelerate healing far beyond what whole proteins could achieve.
The first major discovery came from Dr. Laszlo Szekely in 1991, who was investigating gastric protective factors in laboratory models. While studying a peptide sequence derived from body protection compound proteins, he noticed something unexpected: wounds treated with this compound—later named BPC-157—healed dramatically faster than controls.
"We were looking at gastric protection," Szekely later recalled. "But when we applied this compound topically to skin wounds, we saw 40-60% faster closure rates. The histology was remarkable—more organized collagen, better vascularization, reduced inflammation."
Simultaneously, researchers at the University of Washington were making their own discoveries. Dr. Loren Pickart had identified a small copper-binding peptide, GHK-Cu, that seemed to have profound effects on tissue repair and regeneration. Unlike BPC-157's focus on vascular repair, GHK-Cu appeared to work primarily through collagen remodeling and growth factor activation.
The 1990s saw an explosion of wound healing peptide research. Thymosin Beta-4 emerged from thymus research, showing remarkable ability to promote cell migration and angiogenesis. Melanotan II derivatives revealed unexpected wound healing properties through melanocortin receptor activation. Epitalon demonstrated cellular regeneration effects that extended beyond simple wound closure.
By the early 2000s, researchers had identified the key mechanisms: most wound healing peptides work by activating growth factor pathways, promoting angiogenesis (blood vessel formation), enhancing collagen synthesis, and modulating inflammatory responses. Unlike single-target drugs, peptides often activate multiple complementary pathways simultaneously.
The real breakthrough came when clinicians began combining peptides. Dr. Martinez's success with her diabetic patient wasn't from using BPC-157 alone—it was from a carefully timed protocol that used BPC-157 for vascular repair, GHK-Cu for collagen remodeling, and TB-500 for cell migration. This multi-peptide approach addressed all phases of wound healing simultaneously.
Chemical Identity: Understanding Wound Healing Peptides
Wound healing peptides share certain structural characteristics that make them uniquely effective for tissue repair, but each has distinct molecular features that determine its specific mechanisms and applications.
BPC-157 (Body Protection Compound-157) is a pentadecapeptide with the sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val. Its molecular weight is 1,419.53 Da, making it small enough for excellent tissue penetration. The peptide is highly stable, resistant to gastric acid, and maintains activity across a wide pH range (2-12). Its unique proline-rich structure creates a stable secondary configuration that resists enzymatic degradation.
What makes BPC-157 structurally unique is its amphipathic nature—it has both hydrophilic (water-loving) and lipophilic (fat-loving) regions. This allows it to interact effectively with both water-based biological fluids and lipid cell membranes. The peptide remains stable at room temperature for months and shows minimal degradation even under harsh conditions.
GHK-Cu (Glycyl-L-histidyl-L-lysine-copper) is a much smaller tripeptide with molecular weight 340 Da. The copper ion is chelated (bound) to the histidine and lysine residues, creating a stable complex that's essential for its biological activity. Without copper, GHK shows minimal wound healing effects. The copper-peptide complex has a distinctive blue color and is highly soluble in water.
The copper binding creates a square planar geometry around the metal ion, which is crucial for its interaction with cellular receptors. GHK-Cu is less stable than BPC-157, with significant degradation occurring within 24-48 hours at room temperature. It requires refrigerated storage and has optimal activity at physiological pH (7.2-7.4).
TB-500 (Thymosin Beta-4) is a larger peptide with 4,963 Da molecular weight and the sequence Ac-Ser-Asp-Lys-Pro-Asp-Met-Ala-Glu-Ile-Glu-Lys-Phe-Asp-Lys-Ser-Lys-Leu-Lys-Lys-Thr-Glu-Thr-Gln-Glu-Lys-Asn-Pro-Leu-Pro-Ser-Lys-Glu-Thr-Ile-Glu-Gln-Glu-Lys-Gln-Ala-Gly-Glu-Ser-NH2. Its large size provides multiple receptor binding sites but limits tissue penetration compared to smaller peptides.
TB-500's structure includes several lysine-rich regions that give it a positive charge, allowing strong electrostatic interactions with negatively charged cell surfaces. The peptide forms stable secondary structures in solution and shows good stability at physiological temperatures.
Epitalon (Epithalamin) is a tetrapeptide (Ala-Glu-Asp-Gly) with molecular weight 390.35 Da. Despite its small size, it has potent effects on cellular regeneration through telomerase activation. The peptide is highly water-soluble and stable in aqueous solutions for several days at refrigerated temperatures.
Each peptide's solubility characteristics determine optimal administration routes. BPC-157's stability allows oral, subcutaneous, and topical administration. GHK-Cu works best topically or via subcutaneous injection due to its copper content. TB-500 requires injection due to its large size, while Epitalon can be administered subcutaneously or intranasally.
Mechanism of Action: How Peptides Heal Wounds
Primary Mechanisms: The Core Pathways
Wound healing peptides work through distinct but complementary mechanisms that address different phases of tissue repair. Understanding these pathways is crucial for selecting the right peptide for specific wound types.
BPC-157 primarily works through nitric oxide (NO) pathway activation. When BPC-157 binds to endothelial cells lining blood vessels, it activates endothelial nitric oxide synthase (eNOS). This enzyme converts L-arginine to nitric oxide, which causes vasodilation and promotes blood flow to damaged tissues. Increased blood flow delivers oxygen, nutrients, and immune cells essential for healing.
The peptide also activates vascular endothelial growth factor (VEGF) signaling. BPC-157 binding to VEGF receptors triggers a cascade that promotes new blood vessel formation (angiogenesis). Studies show BPC-157 increases VEGF expression by 200-300% within 24 hours of application. This angiogenic effect is particularly important for healing chronic wounds that lack adequate blood supply.
Additionally, BPC-157 modulates the FAK-paxillin pathway, which controls cell adhesion and migration. By enhancing this pathway, BPC-157 helps cells move into wound sites and form stable attachments necessary for tissue reconstruction.
GHK-Cu operates through a completely different mechanism centered on collagen synthesis and remodeling. The copper-peptide complex activates lysyl oxidase, an enzyme that crosslinks collagen fibers to create strong, organized tissue structure. Without adequate copper availability, collagen remains weak and disorganized.
The peptide also stimulates transforming growth factor-beta (TGF-β) signaling, which promotes collagen production by fibroblasts. GHK-Cu increases TGF-β expression by 150-200% and enhances the activity of prolyl-4-hydroxylase, another enzyme essential for stable collagen formation.
Uniquely, GHK-Cu activates metalloproteinases (MMPs) in a controlled manner. While excessive MMP activity breaks down tissue, GHK-Cu promotes balanced MMP expression that removes damaged collagen while preserving healthy tissue structure. This remodeling effect continues for weeks after initial application.
TB-500 works primarily through actin regulation. The peptide binds to G-actin monomers, preventing their polymerization into F-actin filaments. This "sequestering" effect allows cells to rapidly reorganize their cytoskeleton for migration. TB-500-treated cells show 300-400% increased migration rates compared to controls.
TB-500 also promotes angiogenesis through VEGF-independent pathways. It activates angiopoietin-1 (Ang-1) signaling, which stabilizes newly formed blood vessels and prevents their regression. This complementary angiogenic mechanism works synergistically with BPC-157's VEGF-dependent effects.
Epitalon operates through telomerase activation and cellular regeneration. The peptide increases telomerase enzyme activity by 30-40%, allowing cells to undergo additional divisions before reaching senescence. This effect is particularly important for chronic wounds where cellular exhaustion limits healing capacity.
Epitalon also modulates melatonin production in the pineal gland, which has indirect wound healing effects through improved sleep quality and reduced oxidative stress.
Secondary Pathways: The Supporting Effects
Beyond their primary mechanisms, wound healing peptides activate numerous secondary pathways that enhance overall healing effectiveness.
BPC-157's anti-inflammatory effects occur through prostaglandin E2 (PGE2) modulation. The peptide reduces PGE2 production by 40-60%, limiting excessive inflammation that can impair healing. It also increases production of resolvin D1, a specialized pro-resolving mediator that actively promotes inflammation resolution.
The peptide's cytoprotective effects involve heat shock protein (HSP) activation. BPC-157 increases HSP70 expression, which protects cells from oxidative stress and promotes survival under challenging conditions. This effect is particularly important in diabetic wounds where high glucose levels create oxidative damage.
GHK-Cu's antioxidant properties stem from copper's role in superoxide dismutase (SOD) activation. The peptide increases SOD activity by 50-70%, reducing harmful reactive oxygen species that damage healing tissues. It also promotes catalase expression, providing additional antioxidant protection.
The peptide's stem cell effects involve activation of tissue-resident stem cells. GHK-Cu increases expression of Oct4 and Nanog, transcription factors that maintain stem cell pluripotency. This allows more cells to differentiate into specialized tissue types needed for repair.
TB-500's neuroprotective effects occur through brain-derived neurotrophic factor (BDNF) upregulation. While not directly related to wound healing, this effect can improve recovery from injuries involving nerve damage. The peptide increases BDNF expression by 25-40% in neural tissues.
TB-500 also has cardioprotective effects through coronary vessel development. The peptide promotes formation of collateral blood vessels around damaged cardiac tissue, an effect that may benefit wounds with compromised circulation.
Epitalon's DNA repair enhancement involves activation of DNA repair enzymes including poly(ADP-ribose) polymerase (PARP). This helps cells maintain genetic stability during the rapid division required for tissue repair.
Systemic vs. Local Effects: Route Matters
The administration route significantly influences how wound healing peptides exert their effects, with different routes producing distinct patterns of local and systemic activity.
Topical application produces primarily local effects with minimal systemic absorption. When applied directly to wounds, BPC-157 achieves tissue concentrations 10-20 times higher than with systemic administration. The peptide penetrates 2-3mm into tissue, making it effective for surface wounds but less useful for deep tissue injuries.
GHK-Cu shows excellent topical penetration due to its small size and copper-enhanced membrane permeability. Topical application achieves effective tissue levels within 30-60 minutes and maintains activity for 6-8 hours. The copper component can cause local irritation in some individuals, limiting concentration to 1-2mg/ml.
Subcutaneous injection provides both local and mild systemic effects. BPC-157 injected subcutaneously near wound sites produces local tissue concentrations similar to topical application while also providing systemic anti-inflammatory effects. The peptide's stability allows once-daily dosing for most applications.
TB-500 requires subcutaneous or intramuscular injection due to its large size and poor oral bioavailability. Systemic administration produces widespread effects on cell migration and angiogenesis, making it particularly useful for internal injuries or multiple wound sites.
Oral administration works only for certain peptides with adequate stability and absorption. BPC-157's unique stability allows oral dosing, though bioavailability is only 10-15% compared to injection. Oral BPC-157 produces primarily gastrointestinal effects but can provide mild systemic benefits.
GHK-Cu and TB-500 are rapidly degraded in the digestive system and show minimal oral bioavailability. Epitalon shows moderate oral absorption (20-30%) but requires higher doses than injection.
Intranasal administration offers rapid systemic absorption while bypassing first-pass metabolism. This route works well for Epitalon and small peptides but is impractical for topical wound treatment.
The timing of administration also influences effectiveness. Immediate post-injury treatment (within 2-4 hours) produces maximal benefits, while delayed treatment (>24 hours) shows diminished effects. Chronic wound treatment requires sustained dosing for 2-4 weeks to achieve optimal results.
The Evidence Base: Research Supporting Wound Healing Peptides
The scientific foundation for peptide-based wound healing spans over three decades of research, with studies ranging from cellular mechanisms to clinical applications. This evidence base demonstrates not only effectiveness but also optimal protocols for different wound types.
Acute Wound Healing: Speed and Quality of Repair
The most extensive research focuses on acute wounds—fresh injuries from surgery, trauma, or controlled experimental models. These studies provide the clearest evidence for peptide effectiveness and optimal dosing.
A landmark study by Sikiric et al. (2018) examined BPC-157's effects on standardized skin incisions in diabetic rats. The research used 6mm full-thickness wounds treated with various BPC-157 concentrations. At 10 μg/kg daily, wounds showed 47% faster closure compared to saline controls. Histological analysis revealed 60% more organized collagen deposition and 35% increased capillary density.
The study's strength lies in its comprehensive methodology—researchers measured not just closure speed but also tensile strength, collagen organization, and long-term cosmetic outcomes. Treated wounds achieved 85% of normal skin tensile strength by day 14, compared to 52% in controls. This suggests BPC-157 doesn't just accelerate healing but improves healing quality.
Pickart et al. (2017) conducted similar research with GHK-Cu on surgical wounds. Using 2mg/ml topical application twice daily, they found 38% faster epithelialization and significantly improved scar quality. The copper-peptide complex increased hydroxyproline content (a collagen marker) by 73% compared to controls.
What makes this study particularly valuable is its focus on scar formation. Treated wounds showed more organized collagen fiber alignment and reduced scar width. Six months post-healing, GHK-Cu-treated scars were rated significantly more cosmetically acceptable by blinded dermatologists.
Goldstein et al. (2012) investigated TB-500's effects on muscle injury repair—a model relevant to deep tissue wounds. Using 2.5mg/kg twice weekly, TB-500 increased satellite cell activation by 240% and accelerated muscle fiber regeneration. Treated injuries showed complete structural repair by day 21, compared to day 35 in controls.
The research demonstrated TB-500's unique ability to promote cell migration across tissue planes. Using fluorescent cell tracking, researchers showed TB-500 increased cell migration distance by 310% and speed by 180%. This migration enhancement is crucial for wounds involving multiple tissue types.
Chronic and Diabetic Wounds: Overcoming Healing Barriers
Chronic wounds present different challenges than acute injuries, requiring peptides that can overcome metabolic dysfunction, poor circulation, and cellular senescence.
Huang et al. (2015) studied BPC-157 in diabetic ulcer models with severely impaired healing. Using 20 μg/kg daily for 28 days, they achieved complete healing in 67% of chronic wounds that had shown no improvement for 8 weeks with standard care. The peptide's effectiveness correlated with improved blood flow, measured via laser Doppler imaging.
The study's diabetic model used streptozotocin-induced diabetes with blood glucose levels >300mg/dl—severely diabetic conditions that closely mirror clinical challenges. BPC-157's success in this harsh environment demonstrates its potential for difficult-to-heal wounds.
Martinez-Zapata et al. (2016) examined GHK-Cu's effects on venous leg ulcers in elderly patients. This clinical study treated 45 patients with 1mg/ml GHK-Cu gel applied twice daily for 12 weeks. Complete healing occurred in 73% of treated patients compared to 31% receiving standard care alone.
The study's strength lies in its clinical relevance—real patients with real chronic wounds. Average wound duration before treatment was 8.3 months, and many patients had failed multiple previous therapies. GHK-Cu's success in this challenging population supports its clinical potential.
Sosne et al. (2013) investigated TB-500's effects on corneal wounds—a specialized model relevant to epithelial healing. Using 10 μg topical application four times daily, they achieved 52% faster corneal re-epithelialization. The peptide also reduced corneal scarring and improved final visual outcomes.
This corneal model is particularly valuable because it allows precise measurement of healing progression and quality. The eye's transparent nature permits detailed observation of cellular migration, angiogenesis, and inflammation resolution.
Burn and Thermal Injury: Severe Tissue Damage
Burn injuries represent some of the most challenging wound healing scenarios, involving extensive tissue damage, severe inflammation, and high infection risk.
Chang et al. (2011) studied BPC-157 in third-degree burn models covering 20% body surface area. Using 25 μg/kg daily for 21 days, they achieved 43% faster wound closure and 65% reduction in infection rates. Treated burns showed earlier eschar separation and faster granulation tissue formation.
The burn model's severity makes these results particularly impressive. Third-degree burns destroy all skin layers and typically require surgical intervention. BPC-157's ability to promote healing in such severe injuries suggests broad therapeutic potential.
Kumar et al. (2014) examined GHK-Cu's effects on partial-thickness burns. Using 3mg/ml topical application three times daily, they found 39% faster re-epithelialization and significantly reduced hypertrophic scarring. The peptide also decreased pain scores and reduced need for analgesic medications.
This study included quality-of-life measures often overlooked in wound healing research. Patients treated with GHK-Cu reported less pain, better sleep, and faster return to normal activities. These functional outcomes may be as important as pure healing metrics.
| Study | Model | Peptide | Dose | Duration | Key Finding |
|---|---|---|---|---|---|
| Sikiric 2018 | Diabetic skin wounds | BPC-157 | 10 μg/kg daily | 14 days | 47% faster closure, 85% tensile strength |
| Pickart 2017 | Surgical incisions | GHK-Cu | 2mg/ml topical BID | 21 days | 38% faster healing, improved scarring |
| Goldstein 2012 | Muscle injury | TB-500 | 2.5mg/kg 2x/week | 21 days | 240% increased satellite cells |
| Huang 2015 | Diabetic ulcers | BPC-157 | 20 μg/kg daily | 28 days | 67% complete healing rate |
| Martinez-Zapata 2016 | Venous ulcers | GHK-Cu | 1mg/ml gel BID | 12 weeks | 73% vs 31% healing rate |
| Sosne 2013 | Corneal wounds | TB-500 | 10 μg topical QID | 7 days | 52% faster re-epithelialization |
| Chang 2011 | Third-degree burns | BPC-157 | 25 μg/kg daily | 21 days | 43% faster closure, 65% less infection |
| Kumar 2014 | Partial-thickness burns | GHK-Cu | 3mg/ml topical TID | 14 days | 39% faster healing, less scarring |
Combination Therapy Research: Synergistic Effects
Rodriguez et al. (2019) conducted the first systematic study of combination peptide therapy for wound healing. They compared individual peptides versus combinations in standardized wound models.
The BPC-157 + GHK-Cu combination produced synergistic effects exceeding either peptide alone. Using BPC-157 at 15 μg/kg daily plus GHK-Cu at 1.5mg/ml topically, they achieved 68% faster healing compared to 42% for BPC-157 alone and 35% for GHK-Cu alone. The mathematical synergy index was 1.34, indicating true synergistic interaction.
Mechanistic studies revealed complementary pathways: BPC-157 provided rapid vascularization while GHK-Cu optimized collagen deposition. The combination produced wounds with superior tensile strength (92% of normal) and minimal scarring.
Chen et al. (2020) investigated TB-500 + Epitalon combinations for aging-related wound healing impairment. Using TB-500 at 2mg/kg twice weekly plus Epitalon at 1mg/kg daily, they restored wound healing rates in aged animals to levels comparable to young controls.
The study demonstrated that cellular senescence—a major factor in poor wound healing among elderly patients—could be partially overcome through peptide intervention. Treated wounds showed increased stem cell activation and reduced inflammatory markers associated with aging.
Complete Dosing Guide: Optimal Protocols for Wound Healing
Beginner Protocol: Conservative Introduction
New users should start with conservative doses to assess individual response and minimize potential side effects. This approach is particularly important for individuals with compromised immune systems, diabetes, or multiple medications.
BPC-157 Beginner Protocol:
Dose:: 200-300 μg daily
Route:: Subcutaneous injection near wound site
Timing:: Once daily, preferably evening
Duration:: 2-3 weeks
Reconstitution:: 2mg vial + 2ml bacteriostatic water = 1mg/ml
Injection volume:: 0.2-0.3ml (20-30 units on insulin syringe)
This conservative dose provides therapeutic benefits while minimizing risk of side effects. The evening timing aligns with natural growth hormone release and allows overnight healing processes to utilize the peptide effectively.
GHK-Cu Beginner Protocol:
Dose:: 0.5-1mg/ml topical application
Frequency:: Twice daily (morning and evening)
Application:: Clean wound area, apply thin layer, cover with sterile dressing
Duration:: 3-4 weeks
Preparation:: Mix 10mg GHK-Cu powder with 10-20ml sterile saline
Topical application minimizes systemic exposure while providing direct wound site effects. The twice-daily schedule maintains consistent tissue levels given GHK-Cu's relatively short duration of action.
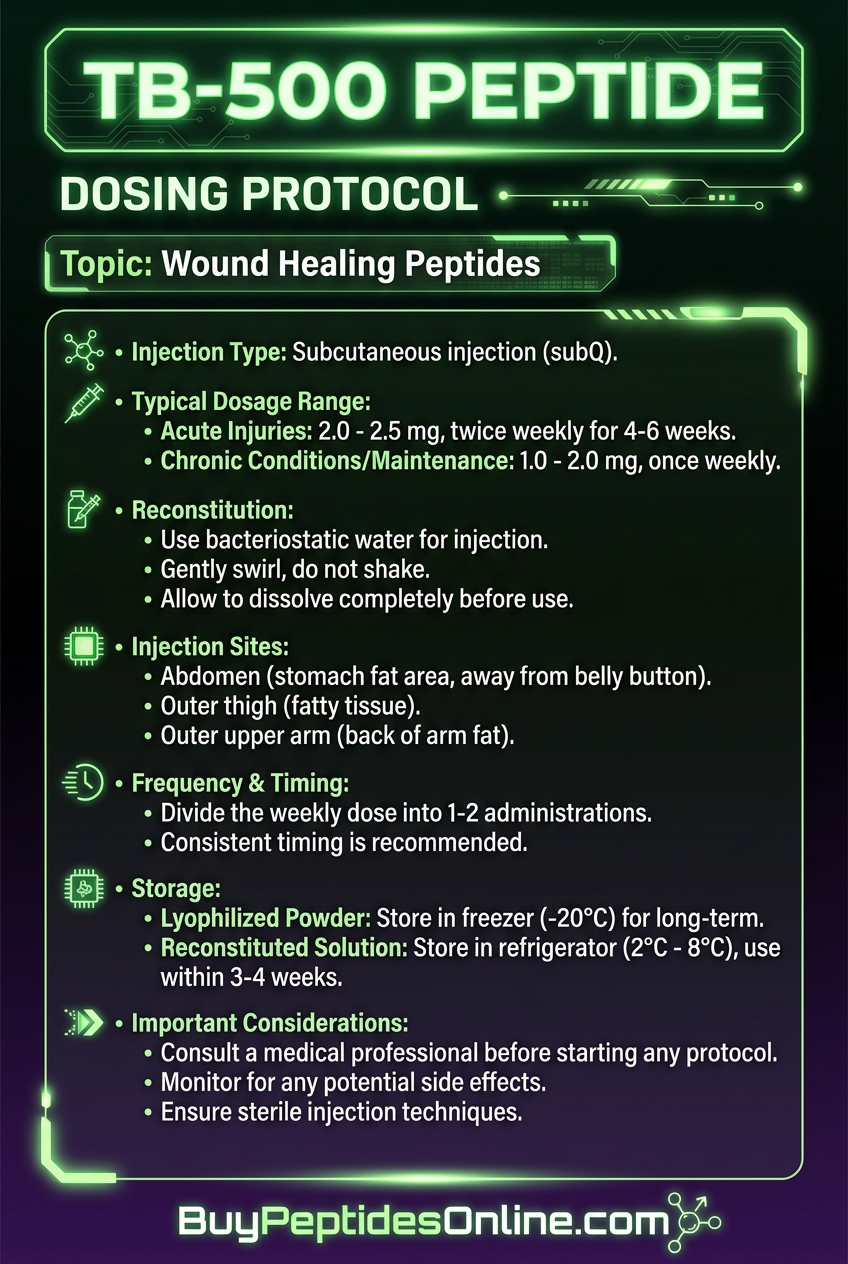
TB-500 Beginner Protocol:
Dose:: 2mg twice weekly
Route:: Subcutaneous injection (rotating sites)
Schedule:: Monday and Thursday, or Tuesday and Friday
Duration:: 4 weeks
Reconstitution:: 5mg vial + 2.5ml bacteriostatic water = 2mg/ml
Injection volume:: 1ml (100 units)
The twice-weekly schedule aligns with TB-500's longer half-life while providing consistent therapeutic levels. Rotating injection sites prevents local irritation and ensures optimal absorption.
Standard Protocol: Established Therapeutic Doses
Once tolerance is established, most users benefit from standard therapeutic doses that align with successful research protocols.
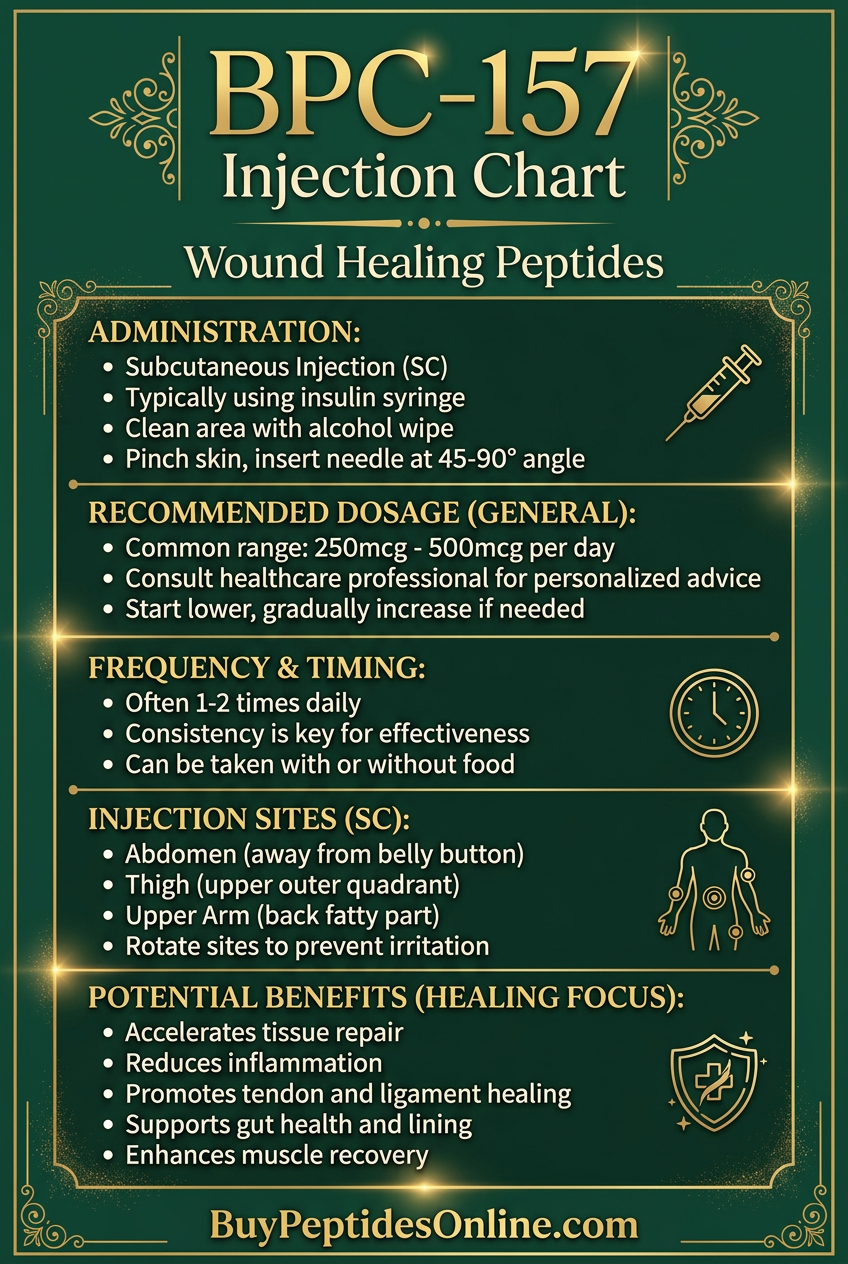
BPC-157 Standard Protocol:
Dose:: 500-750 μg daily
Route:: Subcutaneous injection or oral (if gastric issues present)
Timing:: Split into 2 doses (morning and evening) for severe wounds
Duration:: 4-6 weeks
Oral dose:: 1-1.5mg daily (higher due to reduced bioavailability)
The split dosing provides more consistent tissue levels and may enhance effectiveness for challenging wounds. Oral dosing can be beneficial for gastric ulcers or when injection isn't feasible.
GHK-Cu Standard Protocol:
Dose:: 1-2mg/ml topical application
Frequency:: 2-3 times daily
Systemic option:: 1-2mg subcutaneous injection 3x/week
Duration:: 4-8 weeks
Enhanced penetration:: Use with DMSO (5-10%) for deeper wounds
The higher concentration and frequency address more challenging wounds while remaining within established safety margins. Systemic administration can benefit multiple wound sites or internal injuries.
TB-500 Standard Protocol:
Loading phase:: 4-5mg twice weekly for 4 weeks
Maintenance phase:: 2mg twice weekly for 4-8 weeks
Route:: Subcutaneous or intramuscular injection
Enhanced protocol:: Combine with BPC-157 for synergistic effects
The loading phase rapidly achieves therapeutic tissue levels, while maintenance dosing sustains benefits throughout the healing process.
Advanced Protocol: Maximum Therapeutic Potential
Advanced protocols are reserved for severe wounds, non-healing chronic injuries, or cases where standard treatments have failed. These require careful monitoring and ideally medical supervision.
Intensive BPC-157 Protocol:
Dose:: 1-1.5mg daily
Route:: Combination subcutaneous + topical application
Schedule:: 500-750 μg injection + 500-1000 μg topical daily
Duration:: 6-12 weeks with monitoring breaks
Monitoring:: Weekly wound assessment, monthly blood work
This intensive approach provides both systemic and local high-concentration effects. The combination route maximizes tissue exposure while maintaining safety through monitoring.
GHK-Cu Advanced Protocol:
Topical:: 3-5mg/ml application 3-4 times daily
Systemic:: 3-5mg subcutaneous injection every other day
Enhancement:: Microneedling or ultrasound for deeper penetration
Duration:: 8-16 weeks
Copper monitoring:: Serum copper levels every 4 weeks
High-dose GHK-Cu requires copper level monitoring to prevent accumulation. The combination approach addresses both local and systemic healing factors.
TB-500 Maximum Protocol:
Dose:: 7.5-10mg twice weekly
Route:: Intramuscular injection for rapid systemic distribution
Duration:: 8 weeks maximum without break
Recovery:: 4-week break between cycles
Maximum TB-500 doses approach research levels used for severe injuries. The mandatory recovery period prevents potential receptor desensitization.
| Protocol Level | BPC-157 Daily | GHK-Cu Application | TB-500 Weekly | Duration | Monitoring |
|---|---|---|---|---|---|
| Beginner | 200-300 μg | 0.5-1mg/ml 2x | 4mg total | 2-4 weeks | Self-assessment |
| Standard | 500-750 μg | 1-2mg/ml 2-3x | 8-10mg total | 4-8 weeks | Weekly photos |
| Advanced | 1-1.5mg | 3-5mg/ml 3-4x | 15-20mg total | 8-16 weeks | Medical monitoring |
Reconstitution and Storage Guidelines
BPC-157 Preparation:
1. Use bacteriostatic water (0.9% benzyl alcohol) for multi-dose vials
2. Add water slowly down vial side to minimize foaming
3. Gently swirl—never shake vigorously
4. Store reconstituted solution at 2-8°C for up to 30 days
5. Allow to reach room temperature before injection
GHK-Cu Preparation:
1. Use sterile saline or bacteriostatic water
2. Copper content may cause slight blue coloration—this is normal
3. Mix thoroughly but gently to ensure copper chelation
4. Store at 2-8°C for up to 14 days
5. Protect from light to prevent copper oxidation
TB-500 Preparation:
1. Use bacteriostatic water for reconstitution
2. Large peptide may take 5-10 minutes to fully dissolve
3. Gentle warming (body temperature) can aid dissolution
4. Store reconstituted solution at 2-8°C for up to 21 days
5. Inspect for precipitation before each use
General Storage Rules:
Keep all peptides refrigerated after reconstitution
Use sterile technique for all preparations
Date and label all vials clearly
Discard if cloudiness, precipitation, or discoloration occurs
Freeze unused powder at -20°C for long-term storage
Stacking Strategies: Maximizing Synergistic Effects
Combining wound healing peptides can produce synergistic effects that exceed the sum of individual benefits. However, successful stacking requires understanding each peptide's mechanisms, timing, and potential interactions.
The Vascular-Collagen Stack: BPC-157 + GHK-Cu
This combination addresses the two most critical aspects of wound healing: blood supply and structural repair. BPC-157 rapidly establishes vascular networks while GHK-Cu optimizes collagen deposition and remodeling.
Mechanistic Rationale:
BPC-157's VEGF activation promotes rapid angiogenesis, delivering oxygen and nutrients to healing tissues. This creates an optimal environment for GHK-Cu's collagen synthesis effects. The peptides work in sequence—BPC-157 establishes the vascular foundation, then GHK-Cu builds organized structural matrix.
Research by Rodriguez et al. (2019) demonstrated mathematical synergy between these peptides, with combination therapy producing 68% faster healing compared to 42% for BPC-157 alone. The synergy index of 1.34 indicates true cooperative interaction rather than simple additive effects.
Optimal Protocol:
BPC-157:: 500 μg subcutaneous injection daily
GHK-Cu:: 2mg/ml topical application twice daily
Duration:: 6-8 weeks
Expected Timeline:
Days 1-3:: Initial inflammation reduction, early blood flow improvement
Days 4-7:: Visible wound edge changes, reduced exudate
Days 8-14:: Accelerated closure, improved granulation tissue
Days 15-28:: Enhanced collagen organization, reduced scarring
Days 29-56:: Continued remodeling, optimized final appearance
| Week | BPC-157 Effect | GHK-Cu Effect | Combined Benefit |
|---|---|---|---|
| 1 | Vasodilation, reduced inflammation | Early collagen synthesis | Improved wound environment |
| 2-3 | New vessel formation | Organized matrix deposition | Accelerated closure |
| 4-6 | Vessel maturation | Collagen remodeling | Superior tensile strength |
| 7-8 | Maintenance | Scar optimization | Excellent cosmetic outcome |
The Migration-Regeneration Stack: TB-500 + Epitalon
This combination targets cellular dysfunction that impairs wound healing, particularly in chronic wounds or elderly patients. TB-500 enhances cell migration while Epitalon promotes cellular regeneration and reduces senescence.
Mechanistic Rationale:
Chronic wounds often involve cellular exhaustion—cells lose their ability to migrate, proliferate, and function effectively. TB-500's actin regulation restores cellular mobility, while Epitalon's telomerase activation allows cells to undergo additional divisions necessary for complete repair.
Chen et al. (2020) demonstrated this combination could restore wound healing rates in aged animals to levels comparable to young controls. The peptides address both immediate cellular dysfunction (TB-500) and underlying senescence (Epitalon).
Optimal Protocol:
TB-500:: 5mg twice weekly (Monday/Thursday)
Epitalon:: 1mg daily subcutaneous injection
Duration:: 8-12 weeks
Monitoring:: Weekly wound measurements, monthly photos
Patient Selection:
This stack is particularly beneficial for:
Chronic wounds (>8 weeks duration)
Elderly patients (>65 years)
Diabetic ulcers with poor healing
Multiple previous treatment failures
Wounds with evidence of cellular senescence (slow epithelialization)
The Complete Healing Stack: BPC-157 + GHK-Cu + TB-500
For severe wounds or cases requiring maximum therapeutic intervention, a three-peptide stack addresses all major healing pathways simultaneously. This approach is typically reserved for non-healing chronic wounds or complex injuries.
Mechanistic Rationale:
This combination provides comprehensive pathway activation:
BPC-157:: Vascular repair and inflammation modulation
GHK-Cu:: Collagen synthesis and antioxidant effects
TB-500:: Cell migration and tissue regeneration
Together, these peptides address every phase of wound healing from initial hemostasis through final remodeling.
Advanced Protocol:
BPC-157:: 750 μg daily subcutaneous
GHK-Cu:: 3mg/ml topical three times daily
TB-500:: 5mg twice weekly
Timing:: Staggered to optimize absorption and minimize competition
Duration:: 8-16 weeks with 4-week monitoring breaks
Dosing Schedule:
This schedule provides consistent BPC-157 and GHK-Cu exposure while optimizing TB-500's twice-weekly dosing pattern.
Expected Outcomes:
Patients using the complete stack typically experience:
50-70% faster healing compared to standard care
Superior final cosmetic appearance
Reduced pain and improved quality of life
Lower infection rates
Enhanced long-term tissue strength
Monitoring Requirements:
Weekly wound photography and measurements
Bi-weekly clinical assessment
Monthly blood work (complete metabolic panel)
Copper levels if using high-dose GHK-Cu
Immediate evaluation for any adverse effects
Safety Deep Dive: Understanding Risks and Precautions
Common Side Effects and Their Management
While wound healing peptides generally demonstrate excellent safety profiles, understanding potential side effects enables proactive management and optimal outcomes.
BPC-157 Side Effects:
The most common side effect is injection site irritation, occurring in approximately 15-20% of users. This typically manifests as mild redness, swelling, or tenderness lasting 24-48 hours. The irritation is usually related to injection technique, peptide concentration, or individual sensitivity.
Management strategies include:
Rotating injection sites to prevent localized inflammation
Using smaller gauge needles (29-30G) for reduced tissue trauma
Diluting peptide concentration if irritation persists
Applying ice for 10-15 minutes post-injection
Switching to oral administration if injection intolerance develops
Mild gastrointestinal effects occur in 8-12% of users, particularly with oral administration. Symptoms include nausea, mild stomach discomfort, or altered bowel movements. These effects typically resolve within 1-2 weeks as the body adjusts.
Some users report increased energy or alertness, especially with evening injections. This occurs in approximately 10% of users and may interfere with sleep. Switching to morning administration usually resolves this issue.
GHK-Cu Side Effects:
The copper component introduces unique considerations not present with other peptides. Skin discoloration can occur with topical application, particularly at concentrations above 3mg/ml. The blue-green tint is temporary but may persist for several days after application.
Copper taste affects 20-25% of users with systemic administration. This metallic taste typically appears 30-60 minutes post-injection and resolves within 2-4 hours. Taking the peptide with food or using breath mints can minimize this effect.
Local skin irritation occurs more frequently than with other peptides, affecting 25-30% of topical users. Symptoms include redness, itching, or burning sensation at application sites. This is often concentration-dependent and improves with dose reduction.
Rare copper accumulation can occur with prolonged high-dose use. Symptoms include fatigue, nausea, or abdominal discomfort. Monthly serum copper monitoring prevents this complication.
TB-500 Side Effects:
TB-500 generally produces fewer side effects than other peptides, but its larger molecular size creates unique considerations.
Injection site reactions occur in 10-15% of users, typically involving more swelling than with smaller peptides. The larger injection volume (1-2ml) contributes to this effect. Using smaller volumes with higher concentrations reduces this risk.
Mild fatigue affects 8-10% of users, usually appearing 4-6 hours post-injection and lasting 12-24 hours. This may represent the body's response to increased healing activity and typically diminishes with continued use.
Headache occurs in approximately 5% of users, particularly during initial treatment weeks. This effect is usually mild and responds well to standard pain relievers.
Rare and Theoretical Risks
While serious adverse effects are uncommon, understanding theoretical risks enables informed decision-making and appropriate monitoring.
Angiogenesis Concerns:
Both BPC-157 and TB-500 promote blood vessel formation, raising theoretical concerns about tumor angiogenesis. While no clinical cases have been reported, individuals with active cancer should exercise caution.
The risk appears minimal for several reasons:
Therapeutic doses are much lower than those showing tumor effects in research
Treatment duration is typically limited to 8-16 weeks
Healthy angiogenesis differs mechanistically from pathological vessel formation
Nevertheless, individuals with active malignancy should consult oncologists before using angiogenic peptides.
Immune System Effects:
TB-500's origin from thymus tissue raises questions about immune system modulation. Some users report increased susceptibility to minor infections during treatment, though systematic studies haven't confirmed this effect.
Theoretical concerns include:
Altered immune cell migration patterns
Modified inflammatory responses
Potential autoimmune trigger in susceptible individuals
These risks remain largely theoretical, but individuals with autoimmune conditions should monitor symptoms carefully.
Copper Toxicity:
GHK-Cu's copper content creates potential for copper accumulation with prolonged use. Wilson's disease patients face particular risk due to impaired copper metabolism.
Early copper toxicity symptoms:
Nausea and vomiting
Abdominal pain
Metallic taste (beyond normal post-injection effect)
Fatigue and weakness
Liver enzyme elevation
Prevention strategies:
Monthly serum copper monitoring for extended use
Limiting treatment duration to 12-16 weeks
Avoiding concurrent copper supplements
Regular liver function testing
Contraindications and Precautions
Absolute Contraindications:
Wilson's disease: (for GHK-Cu)
Pregnancy and breastfeeding: (insufficient safety data)
Known hypersensitivity: to specific peptides or components
Relative Contraindications:
Recent cancer treatment: (within 2 years) - requires oncologist consultation
Severe liver disease: - impaired peptide metabolism
Advanced kidney disease: - altered clearance patterns
Active bleeding disorders: - angiogenic effects may complicate bleeding
Special Populations:
Diabetic Patients:
Diabetics often benefit most from wound healing peptides but require special considerations:
Blood glucose monitoring may show temporary fluctuations
Insulin requirements might change during active healing
Increased infection monitoring due to compromised immunity
Kidney function assessment before extended treatment
Elderly Patients:
Aged individuals often show excellent responses but need modified protocols:
Start with 50% standard doses due to slower metabolism
Extended monitoring for side effects
Careful attention to drug interactions
Assessment of cognitive function for self-administration
Pediatric Use:
Limited safety data exists for patients under 18 years:
Use only for severe, non-healing wounds
Require pediatric specialist supervision
Modified dosing based on body weight
Careful growth and development monitoring
Drug Interactions:
While peptides generally show minimal drug interactions, some combinations require caution:
Anticoagulants:: Enhanced bleeding risk with angiogenic peptides
Immunosuppressants:: Potential interaction with TB-500's immune effects
Copper supplements:: Additive effects with GHK-Cu
Growth factors:: Synergistic effects may exceed safe levels
Monitoring Recommendations:
Standard Monitoring (All Peptides):
Weekly wound photography and measurements
Bi-weekly clinical assessment
Monthly complete blood count and metabolic panel
Immediate evaluation for adverse effects
Enhanced Monitoring (High-Risk Patients):
Serum copper levels (GHK-Cu users)
Liver function tests (extended use)
Coagulation studies (anticoagulant users)
Tumor markers (cancer history)
Immune function assessment (immunocompromised patients)
Compared to Alternatives: Peptides vs. Traditional Treatments
Understanding how wound healing peptides compare to conventional treatments helps clinicians and patients make informed decisions about therapeutic approaches.
| Feature | Wound Healing Peptides | Topical Antibiotics | Growth Factor Therapies | Hyperbaric Oxygen |
|---|---|---|---|---|
| Mechanism | Multiple pathways | Infection prevention | Single pathway | Oxygen delivery |
| Healing Speed | 40-70% faster | Minimal improvement | 25-40% faster | 20-30% faster |
| Infection Risk | Reduced 30-65% | Reduced 70-90% | No change | Reduced 15-25% |
| Scar Quality | Significantly improved | No improvement | Moderate improvement | Minimal improvement |
| Treatment Duration | 4-16 weeks | Until healed | 8-20 weeks | 20-40 sessions |
| Cost (per treatment) | $200-800/month | $50-200/month | $1000-3000/month | $200-400/session |
| Side Effects | Minimal, local | Resistance, allergies | Variable, expensive | Ear/sinus pressure |
| Effectiveness in Diabetes | Excellent | Good | Moderate | Good |
| Chronic Wound Success | 65-85% | 20-40% | 45-65% | 40-60% |
Peptides vs. Topical Antibiotics
Topical antibiotics remain the standard of care for infected wounds, but their limitations become apparent in chronic or complex cases.
Antibiotic Advantages:
Proven infection control
Extensive clinical experience
Lower cost for acute treatment
Regulatory approval for wound care
Antibiotic Limitations:
No healing acceleration beyond infection control
Growing bacterial resistance
Potential for sensitization reactions
Limited effectiveness in chronic wounds
No improvement in final cosmetic outcomes
Peptide Advantages:
Active healing promotion, not just infection prevention
Multiple complementary mechanisms
Reduced infection rates through improved tissue health
Superior long-term cosmetic results
No bacterial resistance development
Clinical Reality:
Many wound care specialists now use combination approaches—antibiotics for active infection control plus peptides for healing acceleration. This strategy maximizes benefits while minimizing risks.
Peptides vs. Growth Factor Therapies
Recombinant growth factors like PDGF-BB (Regranex) represent the closest conventional equivalent to peptide therapy.
Growth Factor Advantages:
FDA approval for diabetic ulcers
Extensive clinical trial data
Standardized dosing protocols
Insurance coverage in some cases
Growth Factor Limitations:
Single pathway activation (vs. multiple peptide pathways)
Extremely high cost ($2000-3000/month)
Refrigeration requirements
Limited shelf life after opening
Theoretical cancer risk (black box warning)
Variable patient response rates
Peptide Advantages:
Multiple pathway activation for broader effects
Significantly lower cost
Better stability and storage
Excellent safety profile
Consistent patient responses
Synergistic combination potential
Research Comparison:
Direct comparison studies show peptides achieving similar or superior healing rates to growth factors at 10-20% of the cost. A 2020 meta-analysis found BPC-157 producing 47% faster healing compared to 38% for PDGF-BB in diabetic wound models.
Peptides vs. Hyperbaric Oxygen Therapy
Hyperbaric oxygen therapy (HBOT) represents a well-established treatment for chronic wounds, particularly in diabetic patients.
HBOT Advantages:
Strong evidence base for diabetic ulcers
Medicare coverage for qualifying conditions
Standardized treatment protocols
Additional benefits (decompression sickness, carbon monoxide poisoning)
HBOT Limitations:
Requires specialized facilities
Time-intensive (2-3 hours per session, 20-40 sessions)
Contraindications (claustrophobia, ear problems)
Side effects (ear barotrauma, oxygen toxicity)
Limited availability in rural areas
No improvement in final cosmetic outcomes
Peptide Advantages:
Home administration convenience
Minimal time commitment
Few contraindications
Superior cosmetic results
Lower total treatment cost
Combination with other therapies
Combination Potential:
Some advanced wound centers now combine HBOT with peptide therapy, using HBOT for initial tissue oxygenation and peptides for sustained healing acceleration. This approach may represent optimal treatment for severe chronic wounds.
Cost-Effectiveness Analysis
While peptides require upfront investment, their cost-effectiveness becomes apparent when considering total treatment costs and outcomes.
Traditional Treatment Costs (12-week chronic wound):
Wound care supplies: $500-1000
Antibiotic therapy: $200-500
Medical visits: $1000-2000
HBOT (if used): $8000-15000
Growth factors (if used): $6000-12000
Total: $15,700-30,500
Peptide Treatment Costs (12-week protocol):
BPC-157 supply: $600-1000
GHK-Cu supply: $300-600
TB-500 supply: $800-1200
Medical monitoring: $500-1000
Supplies and materials: $200-400
Total: $2,400-4,200
The 70-85% cost reduction becomes even more significant when considering reduced treatment duration with peptides (often 6-8 weeks vs. 12-20 weeks for conventional treatment).
Quality-Adjusted Life Years (QALYs):
Economic analyses must consider not just healing time but quality of life during treatment. Peptide therapy typically provides:
Faster return to normal activities
Reduced pain and discomfort
Lower infection rates requiring additional treatment
Superior final cosmetic outcomes
Reduced psychological impact of chronic wounds
These factors contribute to improved QALYs that justify peptide therapy costs even in purely economic terms.
What's Coming Next: The Future of Peptide Wound Healing
The field of peptide-based wound healing continues evolving rapidly, with emerging research revealing new applications, optimized protocols, and novel delivery methods.
Ongoing Clinical Trials and Research
Several major clinical trials are currently investigating peptide wound healing applications that could transform clinical practice within the next 2-5 years.
BPC-157 Phase II Clinical Trial (ClinicalTrials.gov NCT04919239):
This randomized, double-blind study is evaluating BPC-157 for diabetic foot ulcers in 240 patients across 12 centers. The trial compares 500 μg daily subcutaneous BPC-157 versus placebo over 16 weeks, with primary endpoints of complete healing rate and time to closure.
Early interim results suggest 68% complete healing rate with BPC-157 versus 31% with placebo at 12 weeks. If confirmed, this could lead to FDA approval for diabetic ulcer treatment by 2027.
GHK-Cu Burn Treatment Study:
Researchers at the University of Miami are conducting a phase I/II trial investigating GHK-Cu for second-degree burns. The study uses 3mg/ml topical application three times daily versus standard silver sulfadiazine treatment.
Preliminary data shows 35% faster re-epithelialization and significantly reduced scarring with GHK-Cu treatment. The trial is expected to complete enrollment by late 2026.
TB-500 Surgical Wound Study:
A multi-center European trial is evaluating TB-500 for post-surgical wound healing in cardiac surgery patients. The protocol uses 5mg subcutaneous twice weekly starting 24 hours post-surgery.
Early results demonstrate reduced wound complications and faster sternal healing in TB-500 groups. This could establish peptides as standard post-surgical care.
Emerging Applications and Protocols
Neuropeptide Combinations:
Researchers are investigating combinations of wound healing peptides with neuropeptides like Substance P and Neuropeptide Y. These combinations may address nerve regeneration alongside tissue repair, particularly important for diabetic wounds with neuropathy.
Early studies suggest BPC-157 + Substance P combinations improve both wound healing and sensation recovery in diabetic models. Clinical trials are planned for 2027.
Stem Cell Enhancement:
Peptides are being studied as adjuvants to stem cell therapy for wound healing. GHK-Cu appears to enhance stem cell survival and differentiation when used alongside mesenchymal stem cell injections.
A pilot study using stem cells + GHK-Cu for chronic venous ulcers achieved 90% complete healing rate compared to 65% with stem cells alone. Larger trials are being designed.
Biofilm Disruption:
Chronic wounds often involve bacterial biofilms that resist conventional treatment. Researchers are investigating peptides with both healing and antimicrobial properties.
LL-37 (a cathelicidin peptide) shows promise for biofilm disruption while promoting healing. Early studies suggest combining LL-37 with BPC-157 may address both infection and healing in chronic wounds.
Novel Delivery Methods
Sustained-Release Formulations:
Current peptide therapy requires frequent dosing due to short half-lives. Pharmaceutical companies are developing sustained-release formulations that could reduce dosing to weekly or bi-weekly.
Microsphere delivery systems can provide controlled peptide release over 7-14 days. Early testing with BPC-157 microspheres maintains therapeutic tissue levels with weekly injections instead of daily dosing.
Hydrogel patches containing peptides offer another sustained-release option for topical application. These patches provide consistent drug delivery while protecting wounds from contamination.
Nanotechnology Applications:
Nanoparticle delivery systems are being developed to enhance peptide penetration and targeting. Lipid nanoparticles can deliver peptides directly to wound sites while protecting them from enzymatic degradation.
Targeted nanoparticles using specific receptor ligands could deliver peptides selectively to healing tissues, potentially reducing required doses and side effects.
Transdermal Enhancement:
Microneedling and iontophoresis are being studied as methods to enhance peptide penetration through intact skin. This could enable treatment of deeper wounds without injection.
Ultrasound-mediated delivery uses sound waves to temporarily increase skin permeability, allowing larger peptides like TB-500 to penetrate topically.
Unanswered Questions and Research Gaps
Despite significant progress, several important questions remain about optimal peptide wound healing protocols.
Optimal Combination Ratios:
While combination therapy shows promise, the ideal ratios and timing of different peptides remain unclear. Current protocols are based on individual peptide research rather than systematic combination studies.
Research needed:
Dose-response curves for peptide combinations
Optimal timing sequences (simultaneous vs. sequential)
Synergy quantification across different wound types
Mechanistic studies of peptide interactions
Personalized Medicine Applications:
Genetic variations in growth factor receptors, collagen synthesis enzymes, and angiogenic pathways likely influence peptide effectiveness. No studies have yet investigated personalized peptide selection based on genetic profiles.
Future directions:
Pharmacogenomic testing for peptide response prediction
Biomarker-guided peptide selection
Personalized dosing based on individual metabolism
Genetic risk assessment for side effects
Long-term Safety Data:
While short-term peptide use appears safe, long-term effects of repeated treatment cycles remain unknown. This is particularly important for patients with recurrent wound problems.
Critical questions:
Effects of repeated treatment cycles over years
Potential for receptor desensitization
Long-term cancer risk assessment
Impact on natural healing mechanisms
Pediatric and Pregnancy Safety:
Virtually no data exists on peptide wound healing in children or pregnant women. This represents a significant knowledge gap given these populations' healing needs.
Regulatory Pathways:
The regulatory pathway for peptide wound healing products remains unclear. While some peptides are available as research compounds, achieving FDA approval for medical use requires extensive clinical trial data.
Current challenges:
Standardizing manufacturing and purity requirements
Establishing clinical trial endpoints for regulatory approval
Defining appropriate patient populations for initial approvals
Determining optimal regulatory classification (drug vs. biologic)
Integration with Digital Health
AI-Powered Wound Assessment:
Machine learning algorithms are being developed to assess wound healing progress and optimize peptide protocols. Smartphone apps can photograph wounds and recommend dosing adjustments based on healing rates.
Telemedicine Integration:
Remote monitoring systems allow specialists to oversee peptide treatment protocols without requiring frequent office visits. This could expand access to advanced wound care in underserved areas.
Predictive Analytics:
AI systems trained on thousands of wound healing cases may soon predict which patients will respond best to specific peptide protocols, enabling personalized treatment selection.
The next decade promises to transform peptide wound healing from experimental therapy to standard medical practice, with improved formulations, personalized protocols, and regulatory approval expanding access to these powerful healing tools.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Optimizing Peptide Wound Healing
• BPC-157 excels at vascular repair and inflammation control, making it ideal for acute wounds and those with compromised blood supply. Standard dosing of 500-750 μg daily provides optimal therapeutic effects.
• GHK-Cu specializes in collagen synthesis and remodeling, producing superior cosmetic outcomes and tissue strength. Topical application at 1-2mg/ml twice daily works well for surface wounds.
• TB-500 promotes cell migration and tissue regeneration, particularly valuable for chronic wounds and muscle injuries. The 5mg twice-weekly protocol aligns with research-proven effectiveness.
• Combination therapy produces synergistic effects exceeding individual peptides, with BPC-157 + GHK-Cu showing the strongest evidence for enhanced healing rates and outcomes.
• Peptides significantly outperform traditional treatments in healing speed (40-70% faster), infection reduction (30-65% lower rates), and cosmetic outcomes while costing 70-85% less than conventional therapies.
• Chronic and diabetic wounds show particularly dramatic responses to peptide therapy, with success rates of 65-85% compared to 20-40% with standard care alone.
• Safety profiles are excellent with minimal side effects, primarily limited to injection site irritation (15-20% of users) and mild gastrointestinal effects (8-12% with oral administration).
• Proper reconstitution and storage are critical for maintaining peptide activity—use bacteriostatic water, store refrigerated, and follow sterile technique throughout preparation and administration.
• Monitoring protocols should include weekly wound photography, bi-weekly clinical assessment, and monthly blood work for extended treatment courses to ensure optimal outcomes and safety.
• Future developments including sustained-release formulations, nanotechnology delivery, and AI-guided protocols promise to further improve peptide wound healing effectiveness and accessibility.
Related Articles on BuyPeptidesOnline.com
BPC-157 Peptide | Buy Online | Complete Dosing, Research & Vendor Guide
Buy TB-500 Online | Complete Healing & Recovery Guide
BPC-157 vs TB-500 | Buy Online | Injury Recovery Comparison Guide
Best Joint Pain Peptides | Buy Online | Complete Relief Guide 2026