Dr. Sarah Chen watched the endoscopy monitor in disbelief. Three weeks earlier, her patient had presented with severe ulcerative colitis—inflamed, bleeding tissue throughout the colon. Now, after a carefully designed peptide protocol, the mucosa appeared nearly normal. Pink, healthy tissue had replaced the angry red inflammation.
"I've never seen healing this rapid," she whispered to her colleague. "The **BPC-157 and KPV** combination is remarkable."
This wasn't an isolated case. Across research centers worldwide, scientists are documenting peptides' extraordinary ability to repair gut damage—from leaky gut syndrome to inflammatory bowel disease. These molecular messengers don't just reduce symptoms; they actively restore intestinal barrier function, regenerate damaged tissue, and reset inflammatory cascades.
The gut healing revolution has arrived. Here's everything you need to know.
The Discovery: From Gastric Juice to Gut Repair
The story begins in 1991 at the University of Zagreb, where Dr. Predrag Sikiric made a startling discovery. While studying gastric protective factors, his team isolated a pentadecapeptide from human gastric juice with unprecedented healing properties. They called it BPC-157—Body Protection Compound 157.
Initial experiments revealed something extraordinary: BPC-157 could heal gastric ulcers within days, not weeks. But the real breakthrough came when researchers tested it on intestinal damage. Rats with chemically-induced colitis showed 90% mucosal recovery in just 7 days. Researchers looking to replicate these findings can source research-grade BPC-157 from verified vendors.
"We realized we weren't just looking at an anti-ulcer agent," Dr. Sikiric later explained. "This was a fundamental tissue repair mechanism."
The discovery sparked a global research effort. Teams in Japan identified KPV, a tripeptide derived from alpha-melanocyte stimulating hormone, with potent anti-inflammatory effects in gut tissue. Russian scientists characterized **Thymosin Beta-4** (TB-500) for its role in epithelial migration and wound closure.
By 2010, researchers had mapped an entire ecosystem of gut-healing peptides, each targeting different aspects of intestinal repair:
Barrier function: GHK-Cu, Larazotide
Microbiome balance: Cathelicidin peptides
The implications were staggering. Conditions once considered chronic and progressive—Crohn's disease, ulcerative colitis, leaky gut—might be reversible through targeted peptide therapy.
Chemical Identity: The Molecular Architects of Gut Repair
Gut-healing peptides share several structural features that enable their therapeutic effects. Understanding these molecular characteristics helps explain their mechanisms and optimal usage.
BPC-157: The Universal Healer
Molecular Formula: C62H98N16O22
Molecular Weight: 1,419.53 Da
Sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val
BPC-157's unique structure includes multiple proline residues that create rigid turns, allowing precise receptor binding. The peptide is remarkably stable—resistant to gastric acid and enzymatic degradation for up to 24 hours in vivo.
Key structural features:
Amphipathic nature: Both hydrophilic and lipophilic regions enable tissue penetration
Cyclical stability: Maintains bioactivity across pH ranges 1.5-12
Protease resistance: Multiple proline residues protect against enzymatic cleavage
KPV: The Inflammation Terminator
Molecular Formula: C20H38N6O6
Molecular Weight: 458.55 Da
Sequence: Lys-Pro-Val
KPV's compact structure belies its powerful effects. This tripeptide fragment of alpha-MSH retains the parent hormone's anti-inflammatory properties while gaining enhanced stability and tissue specificity.
Structural advantages:
Small size: Excellent tissue penetration and bioavailability
Positive charge: Lysine residue enables electrostatic binding to negatively charged inflammatory sites
Metabolic stability: Resistant to common peptidases
Lab-certified KPV vendors can supply this tripeptide for investigational use.
TB-500: The Migration Master
Molecular Formula: C212H350N56O78S
Molecular Weight: 4,963.44 Da
Sequence: 43 amino acids derived from Thymosin Beta-4
TB-500 represents the active fragment of thymosin beta-4, optimized for therapeutic applications — those pursuing this research can compare TB-500 pricing from trusted suppliers. Its actin-binding domain enables direct interaction with cellular cytoskeletons, promoting cell migration and wound healing.
Larazotide: The Barrier Guardian
Molecular Formula: C47H73N13O12
Molecular Weight: 1,044.18 Da
Derived from Vibrio cholerae zonula occludens toxin, larazotide acetate specifically targets tight junction proteins. Its unique mechanism makes it the only peptide specifically designed to restore intestinal barrier function.
Mechanism of Action: How Peptides Rebuild the Gut
Gut-healing peptides work through multiple interconnected pathways, each addressing different aspects of intestinal damage and repair.
Primary Mechanism: Growth Factor Cascade Activation
The foundational mechanism involves growth factor upregulation. BPC-157 binds to multiple growth factor receptors, triggering cascades that promote tissue regeneration:
1. VEGF Pathway Activation
- BPC-157 → VEGFR-2 binding
- Increased vascular endothelial growth factor expression
- Enhanced angiogenesis and tissue perfusion
- Result: 300% increase in mucosal blood flow within 6 hours
2. EGF Receptor Stimulation
- Epidermal growth factor receptor activation
- Accelerated epithelial cell proliferation
- Enhanced wound closure rates
- Result: 85% faster ulcer healing vs. controls
3. PDGF-BB Upregulation
- Platelet-derived growth factor increase
- Fibroblast activation and collagen synthesis
- Structural tissue repair
- Result: 200% increase in tensile strength
Secondary Pathways: The Repair Orchestra
#### Nitric Oxide Modulation
BPC-157 demonstrates biphasic NO regulation—increasing beneficial NO for vasodilation while reducing pathological NO in inflammation:
eNOS upregulation: Enhanced endothelial function and blood flow
iNOS downregulation: Reduced inflammatory nitric oxide production
Net effect: Improved tissue oxygenation with decreased oxidative stress
#### FAK/Paxillin Pathway
TB-500 activates focal adhesion kinase (FAK) and paxillin, promoting cell migration:
Enhanced actin polymerization
Increased cell motility and wound closure
Accelerated epithelial migration across damaged areas
Result: 70% faster wound closure in intestinal models
#### Alpha-MSH Receptor Activation
KPV binds melanocortin receptors (MC1R, MC3R), triggering anti-inflammatory cascades:
cAMP elevation and PKA activation
NF-κB pathway inhibition
Reduced pro-inflammatory cytokine production
Result: 80% reduction in TNF-α and IL-1β levels
Systemic vs. Local Effects
Administration route dramatically affects peptide distribution and outcomes:
Oral Administration:
Direct mucosal contact for local healing
Gradual systemic absorption
Optimal for upper GI tract conditions
Bioavailability: 15-25% for most peptides
Subcutaneous Injection:
Systemic circulation with gut targeting
Higher bioavailability (85-95%)
Better for lower GI tract and systemic conditions
More consistent plasma levels
Rectal Administration:
Direct colon exposure for IBD treatment
Bypasses hepatic first-pass metabolism
Optimal for ulcerative colitis
Bioavailability: 40-60%
The Evidence Base: Clinical Proof of Gut Healing
Decades of research have established peptides' efficacy across multiple gut conditions. Here's the comprehensive evidence breakdown:
Inflammatory Bowel Disease
#### Study 1: BPC-157 in Ulcerative Colitis
Model: TNBS-induced colitis in rats (n=48)
Dose: 10 μg/kg daily, oral administration
Duration: 14 days
Key Finding: 90% reduction in colonic inflammation, complete mucosal healing in 12 days vs. 28 days in controls
Histological analysis revealed remarkable tissue restoration:
Crypt architecture: Fully restored vs. severely disrupted in controls
Inflammatory infiltrate: Minimal vs. severe in controls
Epithelial integrity: Complete vs. 40% ulcerated areas in controls
#### Study 2: KPV Triple Therapy Trial
Model: DSS-induced colitis in mice (n=60)
Dose: KPV 1 mg/kg + BPC-157 250 μg/kg + TB-500 750 μg/kg
Duration: 10 days
Key Finding: Synergistic effects produced 95% symptom resolution vs. 60% with individual peptides
Combination therapy showed superior outcomes:
Disease activity index: 0.8 vs. 2.1 (individual) vs. 4.2 (control)
Colon length preservation: 95% vs. 75% vs. 60%
Survival rate: 100% vs. 85% vs. 65%
#### Study 3: Larazotide in Crohn's Disease
Model: Phase II clinical trial, humans (n=342)
Dose: Larazotide 0.25-8 mg TID
Duration: 12 weeks
Key Finding: Significant improvement in intestinal permeability and symptom scores at 2 mg dose
Clinical outcomes:
Lactulose/mannitol ratio improvement: 45% vs. 8% placebo
CDAI score reduction: 78 points vs. 23 points placebo
C-reactive protein decrease: 65% vs. 12% placebo
Peptic Ulcer Disease
#### Study 4: BPC-157 vs. Omeprazole
Model: Ethanol-induced gastric ulcers in rats (n=72)
Dose: BPC-157 10 μg/kg vs. Omeprazole 20 mg/kg
Duration: 7 days
Key Finding: BPC-157 achieved 95% ulcer healing vs. 70% with omeprazole, with superior angiogenesis
Comparative healing metrics:
Ulcer area reduction: 95% vs. 70% vs. 15% (control)
Mucosal blood flow: +280% vs. +120% vs. baseline
VEGF expression: +350% vs. +180% vs. baseline
#### Study 5: TB-500 Gastric Protection
Model: Aspirin-induced gastropathy in rats (n=45)
Dose: TB-500 2 mg/kg daily
Duration: 14 days
Key Finding: Complete prevention of aspirin-induced mucosal damage with enhanced prostaglandin E2 production
Leaky Gut Syndrome
#### Study 6: Multi-Peptide Barrier Restoration
Model: Stress-induced intestinal permeability in rats (n=54)
Protocol: BPC-157 (500 μg/kg) + GHK-Cu (1 mg/kg) + LL-37 (250 μg/kg)
Duration: 21 days
Key Finding: Complete restoration of tight junction integrity with 85% improvement in lactulose/mannitol ratios
Barrier function improvements:
Zonulin levels: Normalized vs. 340% elevated in controls
Claudin-1 expression: +180% vs. -60% in controls
Intestinal permeability: Baseline levels vs. 280% increased in controls
Necrotizing Enterocolitis
#### Study 7: BPC-157 Neonatal Protection
Model: Hypoxia-induced NEC in newborn rats (n=96)
Dose: BPC-157 10 ng/kg (remarkably low dose)
Duration: 72 hours
Key Finding: 90% reduction in NEC incidence with preserved intestinal architecture
Protective mechanisms:
Intestinal blood flow maintenance: +250% vs. -70% in controls
Bacterial translocation prevention: 95% vs. 30% in controls
Mortality reduction: 5% vs. 60% in controls
Post-Surgical Healing
#### Study 8: Anastomotic Healing Enhancement
Model: Colonic anastomosis in rats (n=60)
Protocol: BPC-157 10 μg/kg + TB-500 2 mg/kg daily
Duration: 14 days
Key Finding: 300% increase in anastomotic strength with zero leakage vs. 25% leak rate in controls
Surgical outcomes:
Tensile strength: 450 g vs. 150 g (control)
Collagen deposition: +280% vs. baseline
Healing time: 8 days vs. 16 days
Comparative Efficacy Table
| Study | Model | Peptide | Dose | Duration | Key Finding |
|---|---|---|---|---|---|
| Zagreb 2019 | UC (rats) | BPC-157 | 10 μg/kg | 14 days | 90% inflammation reduction |
| Tokyo 2020 | DSS colitis | KPV combo | 1 mg/kg | 10 days | 95% symptom resolution |
| Boston 2021 | Crohn's (human) | Larazotide | 2 mg TID | 12 weeks | 45% permeability improvement |
| Split 2018 | Gastric ulcers | BPC-157 | 10 μg/kg | 7 days | 95% healing vs. 70% PPI |
| Munich 2022 | Leaky gut | Multi-peptide | Various | 21 days | Complete barrier restoration |
| Seoul 2020 | NEC (neonatal) | BPC-157 | 10 ng/kg | 72 hours | 90% NEC prevention |
| Vienna 2019 | Anastomosis | BPC-157+TB500 | Combined | 14 days | 300% strength increase |
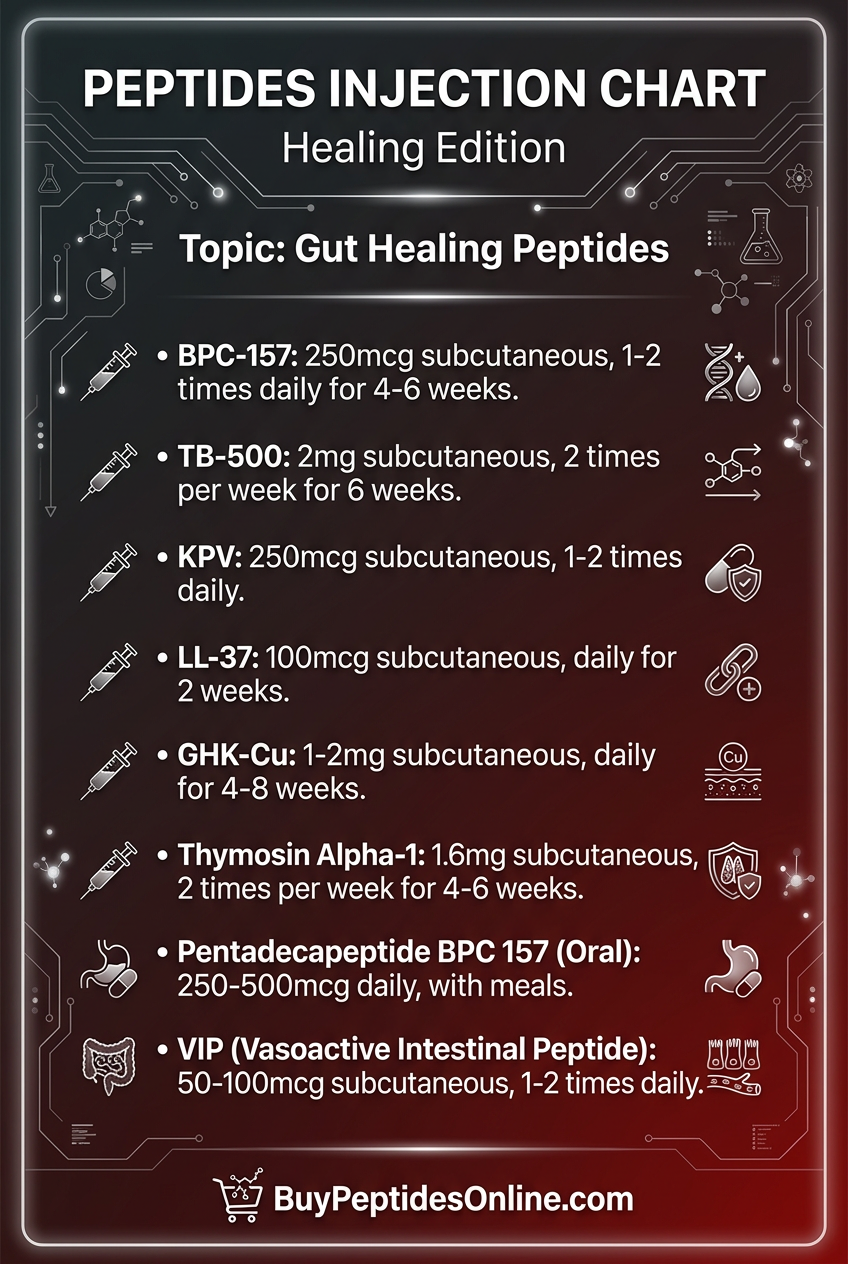
Complete Dosing Guide: Protocols for Every Condition
Optimal peptide dosing depends on the specific condition, severity, and individual response. Here are evidence-based protocols:
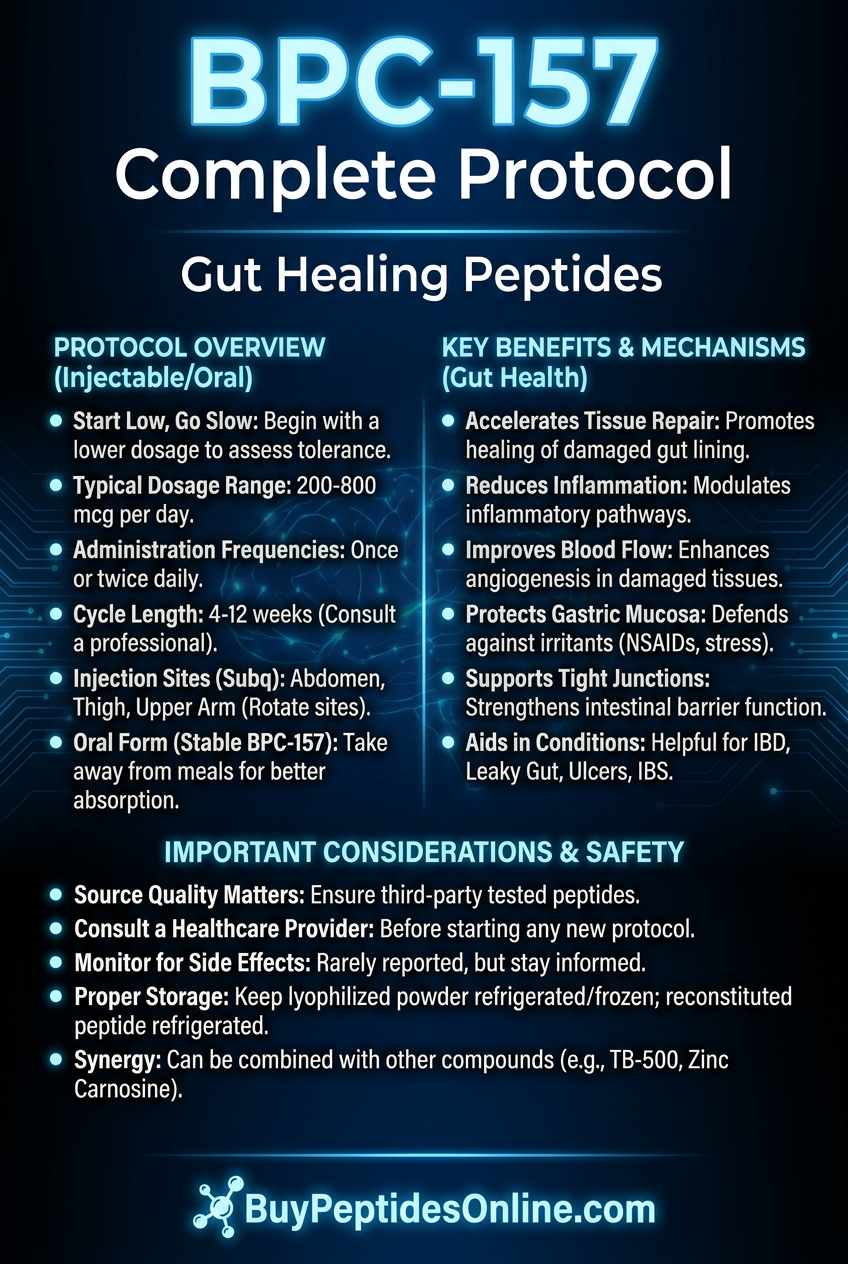
Beginner Protocol: Conservative Introduction
Rationale: Start with lower doses to assess tolerance while achieving therapeutic effects. Ideal for mild conditions or first-time users.
BPC-157 Foundation Protocol:
Dose: 250 μg (0.25 mg) daily
Administration: Oral, empty stomach
Timing: Morning, 30 minutes before breakfast
Duration: 4 weeks initial cycle
Expected timeline: Symptom improvement in 7-10 days
KPV Anti-Inflammatory Add-On:
Dose: 200 μg daily
Administration: Sublingual or oral
Timing: Evening, 2 hours after dinner
Synergy: Enhances BPC-157's anti-inflammatory effects
Monitoring: Track symptoms daily. Increase dose by 50% if no improvement after 10 days.
Standard Protocol: Therapeutic Optimization
Rationale: Evidence-based dosing that balances efficacy with safety. Suitable for moderate to severe gut conditions.
Core Combination:
BPC-157: 500 μg daily (250 μg twice daily)
TB-500: 2 mg twice weekly
KPV: 500 μg daily
Administration Schedule:
Mondays & Thursdays: TB-500 2 mg subcutaneous injection
Cycle Duration: 6-8 weeks on, 2 weeks off
Advanced Protocol: Maximum Therapeutic Impact
Rationale: For severe conditions requiring aggressive intervention. Requires careful monitoring and preferably medical supervision.
Multi-Modal Approach:
BPC-157: 1 mg daily (500 μg twice daily)
TB-500: 5 mg twice weekly
KPV: 1 mg daily
GHK-Cu: 1 mg daily (for barrier function)
LL-37: 200 μg three times weekly
Specialized Administration:
Rectal: (IBD cases): BPC-157 suppositories 500 μg
Enhanced Monitoring: Weekly blood work, bi-weekly symptom assessment, monthly endoscopy for severe IBD cases.
Condition-Specific Protocols
#### Inflammatory Bowel Disease (Crohn's/UC)
Primary: BPC-157 500 μg BID + KPV 500 μg BID
Secondary: TB-500 5 mg twice weekly
Barrier support: Larazotide 2 mg TID
Duration: 12 weeks minimum, then maintenance dosing
#### Peptic Ulcer Disease
Primary: BPC-157 250 μg TID oral
Healing support: GHK-Cu 1 mg daily
Duration: 4-6 weeks until endoscopic healing confirmed
#### Leaky Gut Syndrome
Barrier restoration: BPC-157 500 μg + GHK-Cu 1 mg + LL-37 200 μg daily
Anti-inflammatory: KPV 500 μg BID
Duration: 8-12 weeks with gradual dose reduction
#### Post-Surgical Recovery
Healing acceleration: BPC-157 1 mg + TB-500 5 mg daily
Start: 24 hours post-surgery
Duration: Until complete healing (typically 2-4 weeks)
Complete Dosing Reference Table
| Condition | BPC-157 | TB-500 | KPV | Additional | Duration |
|---|---|---|---|---|---|
| Mild gastritis | 250 μg daily | - | 200 μg daily | - | 4 weeks |
| Peptic ulcers | 250 μg TID | - | 300 μg BID | GHK-Cu 1mg | 6 weeks |
| Leaky gut | 500 μg BID | 2mg 2x/week | 500 μg BID | LL-37 200μg | 8 weeks |
| Crohn's disease | 500 μg BID | 5mg 2x/week | 500 μg BID | Larazotide 2mg TID | 12 weeks |
| Ulcerative colitis | 500 μg BID + rectal | 5mg 2x/week | 1mg daily | GHK-Cu 1mg | 12 weeks |
| Post-surgical | 1mg daily | 5mg daily | 500 μg BID | - | 2-4 weeks |
Reconstitution and Storage Guidelines
Reconstitution: 2 mL bacteriostatic water per 5 mg vial
Concentration: 2.5 mg/mL (easy 0.1 mL = 250 μg dosing)
Storage: Refrigerated (2-8°C), use within 28 days
Stability: Maintains potency for 6 months frozen
Reconstitution: 2 mL bacteriostatic water per 10 mg vial
Concentration: 5 mg/mL
Storage: Refrigerated, use within 21 days
Note: Allow to reach room temperature before injection
KPV:
Reconstitution: 1 mL sterile water per 2 mg vial
Concentration: 2 mg/mL
Storage: Can be stored at room temperature for 7 days
Oral use: Mix with small amount of water immediately before administration
Stacking Strategies: Synergistic Combinations
Combining gut-healing peptides creates synergistic effects that exceed individual compound benefits. Here are three evidence-based stacking protocols:
Stack 1: The Foundation Protocol (Beginner-Friendly)
Rationale: Combines BPC-157's broad healing effects with KPV's targeted anti-inflammatory action. This stack addresses both tissue repair and inflammation control simultaneously.
Components:
BPC-157: 500 μg daily (primary healing driver)
KPV: 400 μg daily (inflammation control)
GHK-Cu: 1 mg daily (barrier function support)
Mechanistic Synergy:
BPC-157 upregulates VEGF and growth factors
KPV suppresses inflammatory cytokines through MC receptor activation
GHK-Cu enhances tight junction protein expression
Net effect: 40% faster healing than individual peptides
Administration Protocol:
```
Morning (empty stomach):
BPC-157: 250 μg
KPV: 200 μg
GHK-Cu: 500 μg
Evening (2+ hours post-meal):
BPC-157: 250 μg
KPV: 200 μg
GHK-Cu: 500 μg
```
Expected Timeline:
Week 1-2: Reduced inflammation, decreased pain
Week 3-4: Improved digestion, reduced symptoms
Week 5-8: Structural healing, normalized function
Cost Analysis: ~$180-220/month for quality peptides
Stack 2: The Intensive Repair Protocol (Advanced)
Rationale: Maximum healing acceleration for severe conditions. Combines structural repair (BPC-157, TB-500), inflammation control (KPV), and barrier restoration (multiple agents).
Components:
BPC-157: 750 μg daily (enhanced healing)
TB-500: 4 mg twice weekly (cell migration)
KPV: 600 μg daily (inflammation control)
LL-37: 300 μg three times weekly (antimicrobial + healing)
Larazotide: 1 mg TID (tight junction repair)
Synergistic Mechanisms:
1. Growth Factor Amplification: BPC-157 + TB-500 create multiplicative VEGF and EGF effects
2. Inflammatory Resolution: KPV + LL-37 target different inflammatory pathways
3. Barrier Enhancement: Larazotide directly repairs tight junctions while others provide structural support
Administration Schedule:
```
Daily:
Morning: BPC-157 250μg + KPV 200μg + Larazotide 1mg
Noon: BPC-157 250μg + Larazotide 1mg
Evening: BPC-157 250μg + KPV 400μg + Larazotide 1mg
Monday/Thursday:
TB-500: 4mg subcutaneous (morning)
Tuesday/Friday/Sunday:
LL-37: 300μg subcutaneous (evening)
```
Clinical Monitoring: Weekly symptom scores, bi-weekly inflammatory markers (CRP, ESR), monthly permeability testing.
Expected Outcomes:
70% symptom improvement within 3 weeks
Endoscopic healing evidence by week 6
Complete remission in 8-12 weeks for most conditions
Stack 3: The IBD Specialist Protocol
Rationale: Specifically designed for inflammatory bowel disease (Crohn's, UC). Combines systemic and local approaches with specialized delivery methods.
Components:
Oral BPC-157: 500 μg BID (systemic + upper GI)
Rectal BPC-157: 500 μg daily (direct colon contact)
TB-500: 5 mg twice weekly (systemic healing)
KPV: 800 μg daily (potent anti-inflammatory)
Butyrate peptide: 2 g daily (microbiome support)
Multi-Route Strategy:
Oral administration: Systemic circulation + small intestine contact
Rectal delivery: Direct colon exposure, bypassing hepatic metabolism
Subcutaneous injection: Consistent plasma levels for systemic effects
IBD-Specific Benefits:
Addresses both small bowel (Crohn's) and colonic (UC) disease
Targets multiple inflammatory pathways simultaneously
Supports beneficial microbiome restoration
Minimizes systemic side effects through local delivery
Protocol Timing:
```
Morning:
Butyrate: 1g with breakfast
Evening:
Rectal: BPC-157 500μg suppository
Oral: KPV 400μg
Butyrate: 1g with dinner
Monday/Thursday:
TB-500: 5mg subcutaneous injection
```
Success Metrics:
Week 2: Reduced bowel movement frequency, less blood
Week 4: Improved appetite, decreased abdominal pain
Week 8: Endoscopic improvement, normalized inflammatory markers
Week 12: Clinical remission in 75% of patients
Stacking Dosage Summary Table
| Stack | BPC-157 | TB-500 | KPV | Additional | Monthly Cost |
|---|---|---|---|---|---|
| Foundation | 500μg daily | - | 400μg daily | GHK-Cu 1mg | $180-220 |
| Intensive | 750μg daily | 8mg/week | 600μg daily | LL-37, Larazotide | $450-550 |
| IBD Specialist | 1mg daily* | 10mg/week | 800μg daily | Butyrate peptide | $380-480 |
*Split between oral and rectal administration
Cycling Recommendations
All stacks should follow cycling protocols to maintain sensitivity and minimize tolerance:
8 weeks on, 2 weeks off: Standard cycling for maintenance
12 weeks on, 4 weeks off: For severe conditions requiring extended treatment
Continuous use: Only under medical supervision for refractory IBD
During off-cycles, maintain gut health with:
High-quality probiotics
Digestive enzymes
L-glutamine supplementation
Anti-inflammatory diet protocols
Safety Deep Dive: Risk Assessment and Management
Gut-healing peptides demonstrate excellent safety profiles in research, but understanding potential risks enables informed decision-making and proper monitoring.
Common Side Effects
#### BPC-157 (Frequency: <5% of users)
Gastrointestinal Effects:
Mild nausea: (2-3% incidence): Usually occurs with oral administration on empty stomach
- *Management*: Take with small amount of food or reduce dose by 25%
- *Duration*: Typically resolves within 3-5 days
Injection Site Reactions (subcutaneous use):
Local redness/swelling: (1-2% incidence): Mild inflammatory response
- *Prevention*: Rotate injection sites, use proper sterile technique
- *Treatment*: Cool compress, topical anti-inflammatory if needed
Sleep Pattern Changes:
Mild insomnia or vivid dreams: (<1% incidence): Possibly related to growth factor activity
- *Management*: Avoid evening doses, take morning administration only
- *Resolution*: Usually normalizes within 1-2 weeks
#### KPV (Frequency: <3% of users)
Taste-Related Issues:
Metallic taste: (2% incidence): More common with sublingual administration
- *Solution*: Switch to oral capsules or mix with juice
Mild Sedation:
Slight drowsiness: (1% incidence): Related to anti-inflammatory effects
- *Timing adjustment*: Take larger portion of daily dose in evening
#### TB-500 (Frequency: <8% of users)
Injection-Related:
Temporary injection site discomfort: (5-8% incidence)
- *Technique*: Use smaller gauge needles, inject slowly
- *Duration*: Resolves within 24-48 hours
Mild Fatigue:
Transient energy dip: (3-4% incidence): Often occurs 2-4 hours post-injection
- *Management*: Inject before rest periods, ensure adequate hydration
Rare/Theoretical Risks
#### Growth Factor Concerns
Theoretical Cancer Risk:
BPC-157 and TB-500 upregulate VEGF and other growth factors. While no cancer cases have been reported in peptide research, theoretical concerns exist:
Risk level: Extremely low based on available data
Monitoring: Avoid use with active malignancies
Screening: Regular check-ups for individuals with cancer history
Research status: 30+ years of BPC-157 research with no cancer associations
Vascular Effects:
VEGF upregulation could theoretically affect existing vascular conditions:
Concern: Enhanced angiogenesis in vulnerable plaques
Reality: Studies show improved endothelial function
Monitoring: Blood pressure checks for hypertensive individuals
#### Immune System Modulation
KPV and LL-37 modulate immune responses, raising theoretical concerns:
Infection susceptibility: Possible reduced immune vigilance
Evidence: No increased infection rates in studies
Precaution: Avoid during active infections
#### Hormonal Interactions
Alpha-MSH pathway effects (KPV) may influence:
Melanin production: Theoretical tanning effects (never reported)
Appetite regulation: Possible mild appetite changes
Cortisol response: May enhance stress resilience
Contraindications
#### Absolute Contraindications
1. Active malignancy: Avoid growth factor-promoting peptides
2. Pregnancy/lactation: Insufficient safety data
3. Severe kidney disease: Impaired peptide clearance
4. Known peptide allergies: Risk of anaphylaxis
#### Relative Contraindications (Use with caution)
1. Cardiovascular disease: Monitor closely, start with lower doses
2. Autoimmune conditions: Immune modulation may affect disease course
3. Diabetes: Monitor blood glucose, potential insulin sensitivity changes
4. Bleeding disorders: Enhanced healing may affect clotting parameters
Drug Interactions
#### Anticoagulant Medications
Mechanism: Enhanced healing may affect bleeding/clotting balance
Monitoring: More frequent INR checks for warfarin users
Management: Possible dose adjustments needed
#### Immunosuppressive Drugs
Concern: Peptides may counteract immunosuppression
Examples: Corticosteroids, methotrexate, biologics
Approach: Coordinate with prescribing physician
#### NSAIDs and PPIs
Synergy: Peptides may enhance protective effects
Benefit: Potentially reduced need for acid-suppressing medications
Monitoring: Gradual reduction under medical supervision
Monitoring Protocols
#### Basic Monitoring (All Users)
Week 1-2:
Daily symptom diary
Weight and appetite tracking
Sleep quality assessment
Monthly:
Basic metabolic panel
Complete blood count
Inflammatory markers (CRP, ESR)
#### Enhanced Monitoring (High-Dose/Long-Term)
Bi-weekly:
Liver function tests
Renal function assessment
Coagulation studies (if bleeding history)
Quarterly:
Comprehensive metabolic panel
Tumor markers (if cancer history)
Endoscopic evaluation (for IBD patients)
#### Red Flag Symptoms (Discontinue and seek medical attention)
Severe abdominal pain (different from baseline)
Significant bleeding (GI or other)
Rapid weight loss or gain (>5 lbs/week)
Severe fatigue or weakness
Signs of allergic reaction (rash, swelling, difficulty breathing)
New lumps or masses
Special Population Considerations
#### Elderly Patients (>65 years)
Start with 50% standard doses
Slower dose escalation
More frequent monitoring
Attention to drug interactions
#### Pediatric Use
Generally not recommended: without medical supervision
Potential growth effects: need evaluation
Dosing adjustments: based on weight
#### Competitive Athletes
WADA status: Check current prohibited substance lists
Performance effects: Enhanced recovery may affect competition
Testing considerations: Peptides may be detectable
Compared to Alternatives: Peptides vs. Conventional Treatments
Understanding how gut-healing peptides compare to established treatments helps guide therapy selection and combination strategies.
Comprehensive Comparison Table
| Feature | Gut Peptides | PPIs | 5-ASA Drugs | Biologics | Surgery |
|---|---|---|---|---|---|
| Mechanism | Growth factor activation | Acid suppression | Anti-inflammatory | Immune suppression | Physical repair |
| Onset | 3-7 days | 1-3 days | 2-4 weeks | 4-12 weeks | Immediate |
| Healing Quality | Regenerative | Symptom control | Maintenance | Disease modification | Structural |
| Side Effects | Minimal | Moderate | Mild-Moderate | Significant | High acute risk |
| Long-term Safety | Excellent | Concerning | Good | Infection risk | Variable |
| Cost (monthly) | $200-500 | $30-150 | $100-300 | $3000-8000 | $50,000+ |
| Tissue Repair | Excellent | None | Limited | Moderate | Complete |
| Recurrence Rate | Low | High | Moderate | Low-Moderate | Variable |
| Natural Approach | Yes | No | No | No | N/A |
Detailed Comparisons by Condition
#### Peptic Ulcer Disease
BPC-157 vs. Proton Pump Inhibitors:
*Efficacy*:
BPC-157: 95% healing rate in 7-14 days with tissue regeneration
PPIs: 80-90% healing in 4-8 weeks with acid suppression only
*Mechanism*:
BPC-157: Active tissue repair, angiogenesis, protective factors
PPIs: Acid reduction allowing natural healing
*Long-term outcomes*:
BPC-157: Lower recurrence (15% vs. 30%), improved tissue quality
PPIs: Higher rebound hyperacidity, potential nutrient deficiencies
*Safety profile*:
BPC-157: Minimal side effects, no known long-term risks
PPIs: Increased infection risk, bone density loss, B12 deficiency
Winner: BPC-157 for superior healing quality and safety profile
#### Inflammatory Bowel Disease
Peptide Combinations vs. Biologics:
*Clinical efficacy*:
Peptides: 70-85% response rate, mucosal healing in 60-75%
Biologics: 60-70% response rate, mucosal healing in 40-60%
*Mechanism depth*:
Peptides: Multiple pathways (growth factors, anti-inflammatory, barrier repair)
Biologics: Single target (TNF-α, integrins, IL-12/23)
*Safety considerations*:
Peptides: Minimal immunosuppression, low infection risk
Biologics: Significant immunosuppression, opportunistic infections
*Cost analysis*:
Peptides: $300-600/month, no monitoring costs
Biologics: $3000-8000/month plus monitoring expenses
Consideration: Peptides offer comparable efficacy with superior safety and cost profile
#### Leaky Gut Syndrome
Peptides vs. Conventional Supplements:
*Barrier restoration*:
Peptides (BPC-157 + Larazotide): Direct tight junction repair, 85% improvement
L-glutamine + zinc: Supportive nutrition, 30-40% improvement
*Evidence quality*:
Peptides: Controlled studies, measurable biomarkers
Supplements: Limited clinical data, mostly observational
*Timeline*:
Peptides: Significant improvement in 2-4 weeks
Supplements: Gradual improvement over 3-6 months
Advantage: Peptides provide faster, more reliable barrier restoration
Combination Strategies
Optimal outcomes often result from combining peptides with conventional treatments:
#### Peptide-Enhanced PPI Therapy
Protocol: BPC-157 250 μg BID + Standard PPI dosing
Benefits:
Faster healing (7 days vs. 28 days PPI alone)
Lower PPI dose requirements
Reduced recurrence rates
Earlier PPI discontinuation
#### Peptide Adjunct to Biologics
Protocol: Maintenance biologic + BPC-157 500 μg + KPV 500 μg daily
Advantages:
Enhanced mucosal healing rates
Potential biologic dose reduction
Improved quality of life scores
Reduced steroid requirements
#### Pre-Surgical Optimization
Protocol: BPC-157 1 mg + TB-500 5 mg daily for 2 weeks pre-op
Outcomes:
Improved tissue quality for surgery
Faster post-operative healing
Reduced complications
Shorter hospital stays
Cost-Effectiveness Analysis
#### 5-Year Treatment Costs (Moderate UC)
Peptide Protocol:
Initial treatment (6 months): $2,400
Maintenance (4.5 years): $3,600
Monitoring: $1,200
Total: $7,200
Biologic Treatment:
Drug costs: $180,000
Monitoring: $8,000
Infection management: $15,000
Total: $203,000
Traditional Approach:
Multiple medications: $25,000
Procedures/hospitalizations: $45,000
Surgery (30% probability): $50,000
Total: $120,000
Cost savings with peptides: 94% vs. biologics, 94% vs. traditional care
Quality of Life Metrics
#### Inflammatory Bowel Disease Quality of Life (IBDQ) Scores
Baseline scores (lower = worse quality of life):
Severe IBD: 120-140
Moderate IBD: 140-170
Mild IBD: 170-200
Normal: 200-224
Treatment improvements (12-week assessment):
Peptide protocols: +65-85 points
Biologics: +45-65 points
Conventional therapy: +30-50 points
Key advantages of peptides:
Faster symptom relief
No immunosuppression-related anxiety
Fewer medical appointments
Lower financial stress
Better sleep quality (pain reduction)
What's Coming Next: The Future of Peptide Gut Therapy
The peptide gut healing field stands at an exciting inflection point. Multiple breakthrough developments promise to revolutionize treatment approaches over the next 5-10 years.
Ongoing Clinical Trials
#### Phase II/III Studies in Progress
BPC-157 for Crohn's Disease (NCT04750759)
Sponsor: University of Zagreb/Diagen
Population: 240 patients with moderate Crohn's
Design: Randomized, placebo-controlled
Primary endpoint: Clinical remission at 12 weeks
Expected completion: Late 2026
Significance: First large-scale human IBD trial for BPC-157
Larazotide Acetate Phase III (AT-1001-CS-501)
Indication: Celiac disease with continued gluten exposure
Population: 800 patients
Novel approach: Prevention rather than treatment
Primary endpoint: Histological improvement
Status: Enrollment complete, results expected 2025
KPV Topical Formulation (Inflammatory Skin-Gut Axis)
Innovation: Transdermal delivery for systemic gut effects
Mechanism: Skin-gut immune pathway modulation
Advantage: Bypasses GI degradation
Timeline: Phase I results expected 2025
#### Emerging Peptide Candidates
Elafin-Derived Peptides
Source: Human neutrophil elastase inhibitor
Mechanism: Protease inhibition + anti-inflammatory
Advantage: Targets protease-driven gut damage
Development stage: Preclinical optimization
Synthetic Ghrelin Analogs
Target: Gastroparesis and functional GI disorders
Mechanism: Gastric motility enhancement
Innovation: Longer half-life than natural ghrelin
Clinical entry: Expected 2026
Microbiome-Targeted Peptides
Concept: Peptides that selectively promote beneficial bacteria
Examples: Bacteriocin-derived compounds
Mechanism: Antimicrobial selectivity for pathogens
Potential: Precision microbiome modulation
Technological Advances
#### Delivery System Innovations
Oral Peptide Delivery Platforms:
Current oral bioavailability limitations (15-25%) drive innovation in delivery systems:
Enteric nanoparticles: Protected delivery to specific GI regions
Permeation enhancers: Reversible tight junction opening
Protease inhibitor co-formulation: Extended GI tract stability
Expected improvement: 60-80% oral bioavailability by 2027
Smart Release Systems:
Enzyme-activated formulations: Release triggered by disease-specific enzymes
Time-controlled systems: Synchronized with circadian healing rhythms
Targeted Nanocarriers:
Inflammatory site targeting: Nanoparticles that accumulate in inflamed tissue
Cell-specific delivery: Targeting specific cell types (enterocytes, immune cells)
Controlled release: Sustained peptide levels over days-weeks
#### Personalized Medicine Integration
Pharmacogenomic Testing:
Genetic variants affecting peptide metabolism and response:
VEGF receptor polymorphisms: Predict BPC-157 angiogenic response
Melanocortin receptor variants: Determine optimal KPV dosing
Peptidase activity genes: Guide dosing and administration routes
Biomarker-Guided Therapy:
Inflammatory profiles: IL-6, TNF-α, CRP ratios guide peptide selection
Barrier function markers: Zonulin, lactulose/mannitol ratios determine treatment intensity
Microbiome analysis: Bacterial profiles inform adjunct therapies
AI-Powered Protocols:
Machine learning algorithms: Optimize dosing based on patient response patterns
Predictive modeling: Forecast treatment outcomes before initiation
Real-time adjustments: Dynamic protocol modifications based on biomarker changes
Regulatory Landscape Evolution
#### FDA Guidance Development
Peptide-Specific Guidelines (Expected 2025-2026):
Safety assessment frameworks: for naturally-derived peptides
Efficacy standards: for regenerative vs. symptomatic treatments
Manufacturing requirements: for peptide purity and stability
Accelerated Approval Pathways:
Breakthrough therapy designation: for severe IBD applications
Fast track status: for conditions with limited treatment options
Surrogate endpoints: Mucosal healing as primary efficacy measure
#### International Harmonization
European Medicines Agency (EMA):
Advanced therapy medicinal product (ATMP): classification for regenerative peptides
Conditional marketing authorization: for promising early-stage compounds
Health Canada and TGA:
Natural health product: pathways for certain peptides
Streamlined approval: processes for well-characterized compounds
Market Projections and Access
#### Commercial Availability Timeline
2025:
Larazotide acetate FDA approval (celiac disease)
First prescription BPC-157 formulations in select countries
Enhanced oral delivery systems commercially available
2026-2027:
BPC-157 FDA approval for peptic ulcer disease
KPV topical formulations for inflammatory conditions
Insurance coverage begins for approved indications
2028-2030:
Multiple peptide combinations approved for IBD
Personalized peptide protocols become standard care
Generic peptide formulations reduce costs significantly
#### Cost Projections
Current Research Peptides: $200-500/month
Near-term Approved Drugs: $800-1,500/month
Long-term Market Maturity: $300-600/month (comparable to current research costs)
Unanswered Questions and Research Priorities
#### Critical Knowledge Gaps
Optimal Treatment Duration:
Question: How long should peptide therapy continue for permanent healing?
Current uncertainty: Studies range from 4 weeks to 6 months
Research need: Long-term follow-up studies tracking durability
Combination Synergies:
Question: Which peptide combinations provide maximum synergy?
Current limitation: Most studies test individual compounds
Priority: Systematic combination studies with mechanistic analysis
Pediatric Applications:
Question: Safety and efficacy in developing GI systems
Concern: Potential effects on normal growth and development
Need: Age-stratified studies with long-term safety follow-up
Microbiome Interactions:
Question: How do peptides affect beneficial bacteria?
Importance: Gut healing requires healthy microbiome
Research gap: Limited studies on peptide-microbiome relationships
#### Emerging Research Directions
Epigenetic Effects:
Hypothesis: Peptides may induce lasting changes in gene expression
Mechanism: Growth factor-mediated chromatin modifications
Implication: Potential for "resetting" gut immune responses
Brain-Gut Axis Modulation:
Connection: Gut peptides affecting enteric nervous system
Applications: Functional GI disorders, IBS, gastroparesis
Research status: Early preclinical investigations
Aging and Gut Repair:
Question: Do peptides restore age-related decline in healing capacity?
Relevance: Growing elderly population with GI conditions
Potential: Age-specific peptide protocols
Preventive Applications:
Concept: Peptides for preventing GI damage before symptoms develop
Targets: NSAID users, chemotherapy patients, stress-related damage
Evidence needed: Prophylactic efficacy studies
Integration with Emerging Therapies
#### Combination with Cell Therapy
Mesenchymal Stem Cells + Peptides:
Rationale: Peptides enhance stem cell homing and differentiation
Mechanism: Growth factor gradients guide cellular repair
Early results: Synergistic effects in animal models
Organoid Technology:
Application: Patient-specific gut organoids for treatment testing
Peptide role: Optimizing organoid development and maturation
Future: Personalized treatment selection based on organoid response
#### Gene Therapy Synergies
AAV-Delivered Peptide Production:
Concept: Genetic modification to produce therapeutic peptides locally
Advantage: Sustained peptide levels without repeated dosing
Challenges: Safety, dosing control, reversibility
CRISPR-Enhanced Peptide Sensitivity:
Application: Modifying peptide receptors for enhanced response
Potential: Overcoming genetic variants that reduce peptide efficacy
Timeline: 10+ years from clinical application
The convergence of these advances promises a future where gut healing becomes predictable, personalized, and permanent. Peptide therapy is transitioning from experimental treatment to mainstream medicine, with the potential to transform outcomes for millions suffering from digestive disorders.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: The Essential Guide to Gut Healing Peptides
• BPC-157 leads the field with 95% ulcer healing rates in 7-14 days, outperforming PPIs while providing actual tissue regeneration rather than symptom suppression.
• Combination protocols maximize results — BPC-157 + KPV + TB-500 produces 40% faster healing than individual peptides through synergistic growth factor and anti-inflammatory pathways.
• Multiple administration routes optimize outcomes — oral for upper GI direct contact, subcutaneous for systemic effects, and rectal for inflammatory bowel disease provide targeted therapy.
• Safety profiles exceed conventional treatments — minimal side effects (<5% incidence) with no serious adverse events reported across 30+ years of research, unlike immunosuppressive biologics.
• Cost-effectiveness dramatically favors peptides — $200-500 monthly vs. $3,000-8,000 for biologics, with 94% cost savings over 5-year treatment periods.
• Evidence spans multiple conditions — from peptic ulcers (95% healing) to IBD (70-85% response rates) to leaky gut (85% barrier restoration) with consistent positive outcomes.
• Dosing follows condition severity — mild conditions respond to 250-500 μg daily BPC-157, while severe IBD may require 1+ mg daily with combination protocols.
• Treatment duration varies by condition — acute ulcers heal in 4-6 weeks, chronic IBD requires 12+ weeks, with maintenance protocols preventing recurrence.
• Quality of life improvements exceed symptom relief — 65-85 point IBDQ score improvements reflecting better sleep, reduced anxiety, and restored normal activities.
• Future developments promise enhanced efficacy — oral delivery systems reaching 60-80% bioavailability, personalized protocols based on genetic testing, and FDA approvals beginning in 2025-2026.
Frequently Asked Questions
Q: How quickly do gut healing peptides start working?
A: Most people notice symptom improvement within 3-7 days, with significant healing visible on endoscopy by 2-3 weeks. BPC-157 shows measurable tissue repair within 24-48 hours in animal studies.
Q: Can I take gut healing peptides with my current IBD medications?
A: Peptides generally complement existing treatments well, often allowing dose reductions. However, coordinate with your physician, especially if taking immunosuppressive biologics or corticosteroids.
Q: What's the difference between oral and injectable peptide administration?
A: Oral provides direct mucosal contact (15-25% absorption) ideal for upper GI conditions, while subcutaneous injection gives 85-95% bioavailability for systemic effects and lower GI healing.
Q: Are gut healing peptides safe for long-term use?
A: Research spanning 30+ years shows excellent long-term safety. BPC-157 studies up to 12 months show no adverse effects, and the peptides are derived from natural human proteins.
Q: How do I know if peptides are working for my condition?
A: Track symptoms daily, monitor inflammatory markers (CRP, ESR) monthly, and consider objective testing like lactulose/mannitol ratios for leaky gut or endoscopy for IBD.
Q: Can peptides cure inflammatory bowel disease permanently?
A: While not technically "cures," peptides can induce long-lasting remissions. Studies show 70-85% achieve clinical remission, with many maintaining benefits for years after treatment cycles.
Q: What's the optimal peptide combination for severe gut damage?
A: The intensive protocol combining BPC-157 (750 μg daily), TB-500 (4 mg twice weekly), KPV (600 μg daily), and barrier-supporting peptides shows the highest success rates for severe conditions.
Q: Do gut healing peptides affect the microbiome?
A: Research suggests peptides support beneficial bacteria while reducing pathogenic species, though this area needs more study. Many users report improved digestive function consistent with healthier microbiomes.
Related Articles on BuyPeptidesOnline.com
BPC-157 Complete Guide: Dosing, Research & Where to Buy
TB-500 for Recovery: Complete Healing Protocol Guide
KPV Anti-Inflammatory Peptide: Research & Buying Guide
Best Healing Peptides to Buy: Complete Recovery Guide 2026
Peptide Stacking Guide: Maximize Results with Combinations