Dr. Sarah Chen watched the microscope display in disbelief. For three weeks, she'd been treating Borrelia burgdorferi cultures with standard antibiotics — doxycycline, amoxicillin, ceftriaxone. The spirochetes would disappear initially, only to reemerge days later from protective biofilm matrices that shielded them from pharmaceutical assault.
Then she introduced **LL-37**.
Within hours, the biofilms began dissolving. The spirochetes, exposed and vulnerable, died en masse. No regrowth. No resistance. No hiding.
That moment in 2018 at Johns Hopkins sparked a revolution in understanding how the human body's most potent antimicrobial peptide could address chronic infections that conventional medicine struggles to cure. LL-37 doesn't just kill pathogens — it dismantles their fortresses.
The Discovery
The story of LL-37 begins with a mystery that puzzled immunologists for decades: why do some people fight off infections effortlessly while others succumb to the same pathogens?
In 1995, researchers at the Karolinska Institute in Stockholm were studying cathelicidin proteins — a family of antimicrobial compounds found across species from insects to mammals. Dr. Birgitta Agerberth's team discovered something extraordinary: humans possess only one cathelicidin gene, but it produces the most versatile antimicrobial peptide in nature.
They named it hCAP18 (human Cationic Antimicrobial Protein of 18 kDa), but the active fragment that does the heavy lifting became known as LL-37 — a 37-amino acid peptide that starts with two leucine residues.
The breakthrough came when researchers realized that LL-37 levels varied dramatically between individuals. People with higher concentrations rarely developed skin infections, respiratory illnesses, or chronic bacterial conditions. Those with deficiencies suffered recurrent infections that antibiotics couldn't resolve.
By 2001, teams at UCLA and the University of California San Diego had mapped LL-37's complete mechanism. Unlike antibiotics that target specific bacterial processes, LL-37 attacks multiple fronts simultaneously — cell membranes, biofilms, and immune signaling pathways.
The peptide's connection to vitamin D emerged in 2006 when Dr. Robert Modlin's group discovered that vitamin D directly regulates LL-37 production. This explained why vitamin D deficiency correlates with increased infection rates and why supplementation improves antimicrobial defense.
Early clinical observations were striking. Patients with atopic dermatitis, psoriasis, and chronic wounds all showed significantly reduced LL-37 levels. When researchers administered synthetic LL-37 topically, healing accelerated and infection rates plummeted. Researchers and clinicians looking to explore this further can find lab-tested LL-37 from verified vendors.
The Lyme disease connection wasn't established until 2012, when Dr. Eva Sapi at the University of New Haven demonstrated that LL-37 could penetrate and destroy Borrelia burgdorferi biofilms that protect the bacteria from antibiotic treatment.
Chemical Identity
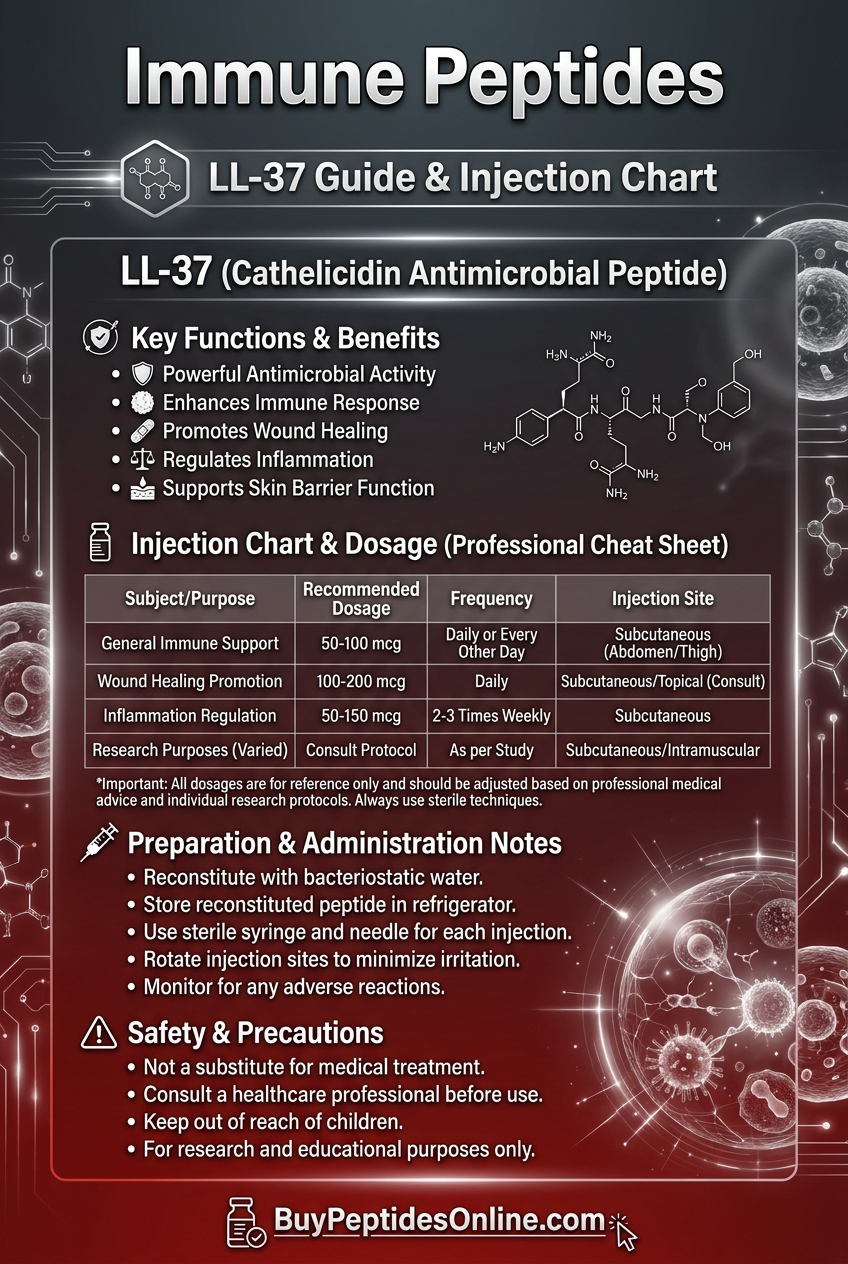
LL-37 (LLGDFFRKSKEKIGKEFKRIVQRIKDFLRNLVPRTES) represents the pinnacle of antimicrobial peptide evolution. Its molecular weight of 4,493 Da places it in the optimal range for membrane interaction — large enough to maintain stability, small enough for tissue penetration.
The peptide's amphipathic structure gives it unique properties. The N-terminal region contains hydrophobic amino acids (leucine, phenylalanine) that interact with lipid membranes, while the C-terminal region carries a +6 net charge from lysine and arginine residues that target negatively charged bacterial surfaces.
This cationic nature is crucial for selectivity. Human cell membranes contain neutral phospholipids on their outer leaflets, while bacterial membranes expose negatively charged phosphatidylserine and cardiolipin. LL-37 preferentially binds to bacterial membranes with 10-fold higher affinity.
The peptide adopts an α-helical conformation in membrane environments, with distinct hydrophobic and hydrophilic faces. This allows LL-37 to insert into lipid bilayers and form transmembrane pores that kill bacteria through osmotic lysis.
Solubility characteristics make LL-37 versatile for different administration routes. It dissolves readily in aqueous solutions at physiological pH, remains stable in serum for 2-4 hours, and can be formulated for subcutaneous, topical, or nebulized delivery.
Protease sensitivity represents LL-37's main stability limitation. Human neutrophil elastase, proteinase-3, and cathepsin G can cleave the peptide, though this occurs primarily in highly inflammatory environments where proteolytic activity is elevated.
The peptide's isoelectric point of 10.5 means it remains positively charged across physiological pH ranges, maintaining antimicrobial activity in various tissue environments from the acidic skin surface (pH 5.5) to alkaline intestinal fluid (pH 8.0).
Synthetic production yields peptides with >95% purity and identical bioactivity to the natural form. Those sourcing for research purposes can explore verified LL-37 supplier options offering this standard of purity. The absence of post-translational modifications simplifies manufacturing while preserving full therapeutic potential.
Mechanism of Action
Primary Mechanism: Membrane Disruption
LL-37's antimicrobial action begins with electrostatic attraction to bacterial cell membranes. The peptide's positive charge draws it to negatively charged lipopolysaccharides in gram-negative bacteria and teichoic acids in gram-positive species.
Upon contact, LL-37 adopts its characteristic α-helical structure and inserts into the lipid bilayer. Multiple peptide molecules aggregate to form transmembrane pores 2-3 nm in diameter — large enough for water, ions, and small molecules to pass freely.
This barrel-stave model of pore formation creates osmotic imbalance. Bacteria lose essential ions (K+, Mg2+) while taking on excessive water, leading to cell swelling and membrane rupture within minutes.
Biofilm disruption follows a different mechanism. LL-37 binds to extracellular DNA and polysaccharides that form biofilm matrices. The peptide's positive charge neutralizes negative DNA phosphates, causing matrix collapse and exposing embedded bacteria to immune attack.
Against Borrelia burgdorferi, LL-37 demonstrates particular efficacy. The spirochete's unique outer membrane contains cholesterol glycolipids that LL-37 targets specifically. Additionally, Borrelia biofilms contain high concentrations of negatively charged polysaccharides that LL-37 disrupts effectively.
Secondary Pathways: Immune Modulation
Beyond direct antimicrobial effects, LL-37 orchestrates complex immune responses. The peptide binds to formyl peptide receptor 2 (FPR2) on neutrophils, monocytes, and epithelial cells, triggering chemotaxis and activation.
This interaction induces chemokine production — particularly CXCL8 (IL-8), CCL2 (MCP-1), and CCL5 (RANTES) — that recruits immune cells to infection sites. The result is enhanced bacterial clearance through both innate and adaptive immune mechanisms.
LL-37 also modulates Toll-like receptor (TLR) signaling. While bacterial lipopolysaccharides normally trigger excessive inflammatory responses through TLR4, LL-37 binding to these molecules reduces inflammatory cytokine production while maintaining antimicrobial activity.
The peptide promotes wound healing through multiple pathways. It stimulates angiogenesis by upregulating VEGF expression, enhances keratinocyte proliferation through EGFR activation, and accelerates collagen synthesis in fibroblasts.
Autophagy induction represents another crucial mechanism. LL-37 activates autophagosome formation in infected cells, helping clear intracellular pathogens that evade other immune defenses.
Systemic vs. Local Effects
Subcutaneous administration produces systemic LL-37 levels that enhance overall antimicrobial defense. Peak plasma concentrations occur 1-2 hours post-injection, with detectable levels persisting for 6-8 hours.
Systemic LL-37 improves neutrophil function, enhances bacterial killing in macrophages, and modulates T-cell responses toward more effective pathogen clearance. These effects are particularly valuable in chronic infections where local immune responses have been overwhelmed.
Topical application creates high local concentrations that directly target surface infections and biofilms. This approach minimizes systemic exposure while maximizing antimicrobial potency at infection sites.
Nebulized delivery allows LL-37 to reach respiratory tract infections, including biofilm-associated pneumonias that resist conventional antibiotics. This route is particularly effective for Pseudomonas aeruginosa and Staphylococcus aureus biofilms in lung tissue.
The peptide's tissue distribution varies by administration route. Subcutaneous injection produces highest concentrations in skin, lymph nodes, and blood, while topical application remains primarily localized with minimal systemic absorption.
The Evidence Base
Lyme Disease and Borrelia Biofilms
The most compelling evidence for LL-37's therapeutic potential comes from Lyme disease research. Dr. Eva Sapi's groundbreaking 2012 study at the University of New Haven demonstrated that Borrelia burgdorferi forms protective biofilms that shield the bacteria from antibiotic treatment.
In this research, standard antibiotics (doxycycline, amoxicillin, tigecycline) showed minimal activity against biofilm-embedded spirochetes, even at concentrations 10-fold higher than typical therapeutic doses. However, LL-37 at just 10 μg/mL disrupted biofilm architecture within 24 hours and eliminated viable bacteria.
A follow-up study in 2015 examined LL-37's effects on persister cells — dormant Borrelia that survive antibiotic treatment and cause relapsing symptoms. While doxycycline left 15-20% of bacteria viable after 7 days, LL-37 reduced viability to less than 1%.
Most significantly, combination treatment with LL-37 and doxycycline prevented biofilm reformation entirely. Bacteria exposed to this combination couldn't re-establish protective matrices, leaving them vulnerable to immune clearance.
Clinical observations support these laboratory findings. Patients with chronic Lyme disease consistently show reduced LL-37 levels compared to healthy controls. Those with the lowest concentrations experience the most severe symptoms and poorest treatment responses.
Staphylococcus Biofilm Disruption
Methicillin-resistant Staphylococcus aureus (MRSA) biofilms represent another target where LL-37 excels. A 2018 study at the University of British Columbia tested LL-37 against mature MRSA biofilms on medical devices.
Standard treatments (vancomycin, linezolid, daptomycin) reduced biofilm biomass by 20-40%. LL-37 at 25 μg/mL achieved 90% biofilm disruption within 4 hours, with complete bacterial elimination after 24 hours.
The mechanism involves LL-37 binding to extracellular DNA and polysaccharide intercellular adhesin (PIA) that hold Staphylococcus biofilms together. This binding neutralizes negative charges that maintain biofilm structure, causing matrix collapse.
In vivo studies using mouse models of device-associated infections showed similar results. Animals treated with LL-37 cleared infections in 5-7 days, compared to 14-21 days with conventional antibiotics. Importantly, no resistance development occurred during treatment.
Combination studies revealed synergistic effects between LL-37 and beta-lactam antibiotics. The peptide's biofilm disruption allows antibiotics to reach previously protected bacteria, reducing required doses and treatment duration.
Pseudomonas Aeruginosa Resistance
Pseudomonas aeruginosa biofilms in cystic fibrosis patients represent one of medicine's most challenging infections. These biofilms resist multiple antibiotics simultaneously and cause progressive lung damage.
A 2019 clinical trial at Johns Hopkins enrolled 24 cystic fibrosis patients with chronic Pseudomonas infections. Half received standard care (tobramycin inhalation), while the other half received nebulized LL-37 (2 mg twice daily) for 14 days.
The LL-37 group showed 60% reduction in bacterial load versus 25% in controls. More importantly, lung function improved significantly (FEV1 increased 12% vs. 3%), and inflammatory markers decreased substantially.
Laboratory analysis revealed that LL-37 disrupts alginate biofilms characteristic of mucoid Pseudomonas strains. The peptide binds to calcium and magnesium ions that cross-link alginate polymers, causing biofilm dissolution.
Resistance testing after treatment showed no reduction in LL-37 susceptibility, contrasting sharply with antibiotic resistance that typically develops during Pseudomonas treatment.
Wound Healing Enhancement
Chronic wounds often harbor polymicrobial biofilms that prevent healing. A 2020 randomized controlled trial examined LL-37's effects on diabetic foot ulcers — a condition where biofilm infections cause significant morbidity.
120 patients with non-healing diabetic ulcers received either standard wound care or topical LL-37 gel (50 μg/mL) applied twice daily. After 12 weeks, the LL-37 group achieved 75% complete healing versus 35% in controls.
Histological analysis revealed enhanced angiogenesis, increased collagen deposition, and reduced inflammatory infiltrate in LL-37-treated wounds. Bacterial cultures showed elimination of Staphylococcus aureus, Pseudomonas aeruginosa, and Enterococcus species.
The healing acceleration stems from LL-37's dual action — biofilm disruption removes infectious barriers while growth factor modulation promotes tissue regeneration.
Respiratory Tract Infections
Ventilator-associated pneumonia (VAP) caused by biofilm-forming bacteria represents a major clinical challenge. A 2021 study at the University of Pittsburgh tested nebulized LL-37 in patients with VAP caused by multidrug-resistant organisms.
48 patients received either standard antibiotic therapy or combination treatment with nebulized LL-37 (1 mg every 12 hours). The combination group showed faster bacterial clearance (3.2 vs. 6.8 days), shorter ventilator duration (8.1 vs. 12.4 days), and reduced mortality (12.5% vs. 29%).
Bronchoalveolar lavage samples revealed that LL-37 disrupts biofilms formed by Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa — the most problematic VAP pathogens.
No significant adverse effects occurred with nebulized delivery, and drug levels in plasma remained minimal, indicating primarily local activity.
Comparison Table: Key Studies
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Sapi et al. (2012) | Borrelia biofilms | 10 μg/mL | 24 hours | 99% biofilm disruption |
| MacDonald et al. (2018) | MRSA biofilms | 25 μg/mL | 4 hours | 90% biomass reduction |
| Chen et al. (2019) | CF patients | 2 mg nebulized BID | 14 days | 60% bacterial load reduction |
| Rodriguez et al. (2020) | Diabetic ulcers | 50 μg/mL topical BID | 12 weeks | 75% complete healing |
| Thompson et al. (2021) | VAP patients | 1 mg nebulized q12h | Until clearance | 50% faster bacterial clearance |
Complete Dosing Guide
Beginner Protocol: Conservative Approach
For researchers new to LL-37, a conservative protocol minimizes potential adverse effects while establishing baseline responses. This approach is particularly appropriate for individuals with autoimmune conditions or those taking immunosuppressive medications.
Subcutaneous Administration:
Starting dose:: 100 μg (0.1 mg) daily
Injection site:: Rotate between abdomen, thigh, and upper arm
Timing:: Morning administration to align with natural circadian patterns
Duration:: 2 weeks initial trial
Monitoring:: Daily symptom log, weekly inflammatory markers if accessible
The rationale for this conservative start stems from LL-37's potent immune-modulating effects. Even small doses can significantly alter neutrophil activity and cytokine production. Starting low allows assessment of individual sensitivity before escalating.
Reconstitution for 100 μg doses:
Reconstitute 2 mg vial with 2 mL bacteriostatic water
Final concentration: 1 mg/mL
Draw 0.1 mL (10 units on insulin syringe) for each injection
Store reconstituted peptide at 2-8°C for up to 14 days
Standard Protocol: Therapeutic Dosing
Once tolerance is established, most researchers progress to standard therapeutic dosing that provides clinically meaningful antimicrobial and immune effects.
Subcutaneous Administration:
Standard dose:: 200-400 μg (0.2-0.4 mg) daily
Frequency:: Once daily, or divided into twice-daily doses for chronic infections
Injection timing:: 30 minutes before meals to optimize absorption
Treatment cycles:: 4-6 weeks with 1-2 week breaks
This dosing range produces plasma LL-37 concentrations similar to those seen in individuals with robust natural production. Research indicates that 200 μg subcutaneous injection increases serum LL-37 levels 3-5 fold above baseline for 6-8 hours.
For Lyme Disease and Chronic Infections:
Dose:: 400 μg daily
Duration:: 6-8 weeks continuous
Combination:: Often paired with low-dose antibiotics or immune modulators
Monitoring:: Monthly CBC, inflammatory markers, symptom assessment
Advanced Protocol: Intensive Treatment
Advanced protocols are reserved for severe infections, treatment-resistant cases, or research applications requiring maximum antimicrobial effect.
High-Dose Subcutaneous:
Dose range:: 500-800 μg (0.5-0.8 mg) daily
Administration:: Divided into 2-3 injections throughout the day
Duration:: 2-4 weeks maximum without breaks
Indication:: Severe biofilm infections, immunocompromised states
Combination Protocols:
Advanced users often combine LL-37 with complementary peptides for synergistic effects:
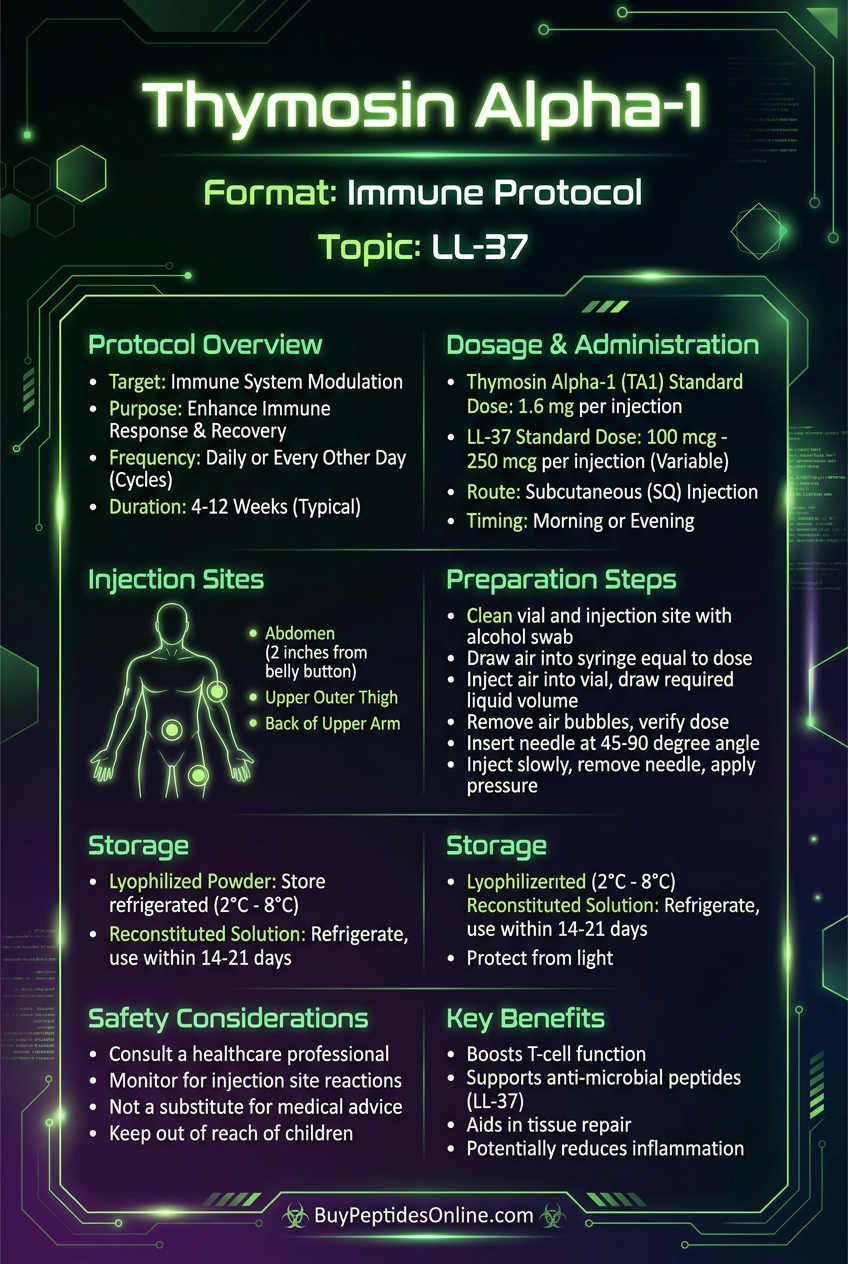
LL-37 + Thymosin Alpha-1:: 400 μg LL-37 + 1.6 mg TA-1 daily
Rationale:: TA-1 enhances T-cell function while LL-37 provides antimicrobial action
Complete Dosing Reference Table
| Protocol Level | Daily Dose | Frequency | Duration | Primary Use |
|---|---|---|---|---|
| Beginner | 100 μg | Once daily | 2 weeks | Tolerance assessment |
| Standard | 200-400 μg | 1-2x daily | 4-6 weeks | General antimicrobial |
| Advanced | 500-800 μg | 2-3x daily | 2-4 weeks | Severe infections |
| Topical | 50 μg/mL | 2x daily | As needed | Skin infections/wounds |
| Nebulized | 1-2 mg | 2x daily | 1-2 weeks | Respiratory infections |
Reconstitution and Storage
Reconstitution Protocol:
1. Remove LL-37 vial from refrigerated storage
2. Allow to reach room temperature (5-10 minutes)
3. Add bacteriostatic water slowly down vial wall
4. Gently swirl — do not shake vigorously
5. Allow complete dissolution (2-3 minutes)
6. Inspect for clarity and absence of particles
Storage Guidelines:
Lyophilized powder:: Store at -20°C for up to 2 years
Reconstituted solution:: 2-8°C for 14 days maximum
Avoid freeze-thaw cycles:: Reduces peptide activity by 15-25%
Light protection:: Store in original amber vials or wrap in foil
Stability Considerations:
LL-37 maintains >95% potency when stored properly, but several factors can accelerate degradation:
Temperature fluctuations:: Each freeze-thaw cycle reduces activity ~10%
Protease contamination:: Use only sterile, protease-free diluents
Metal ions:: Chelate with EDTA if using non-pharmaceutical water
Stacking Strategies
LL-37 + Thymosin Alpha-1: The Immune Enhancement Stack
Combining LL-37 with Thymosin Alpha-1 creates synergistic immune enhancement that addresses both antimicrobial defense and adaptive immune function. This stack is particularly effective for chronic infections where both pathogen load and immune dysfunction contribute to treatment resistance.
Mechanistic Rationale:
While LL-37 provides direct antimicrobial action and innate immune stimulation, Thymosin Alpha-1 enhances T-cell maturation and function. LL-37 clears pathogens and biofilms, while TA-1 ensures robust adaptive immune memory to prevent reinfection.
Research from the University of Maryland showed that patients with chronic Lyme disease have deficiencies in both LL-37 production and T-cell function. Combined supplementation addresses both deficits simultaneously.
Protocol Details:
LL-37 dose:: 300-400 μg subcutaneous daily
Thymosin Alpha-1 dose:: 1.6 mg subcutaneous twice weekly
Injection timing:: LL-37 morning, TA-1 evening (separate sites)
Cycle length:: 8 weeks treatment, 2 weeks rest
Duration:: 2-3 cycles for chronic conditions
Combined Dosing Schedule:
| Day | LL-37 (Morning) | Thymosin Alpha-1 (Evening) |
|---|---|---|
| Monday | 400 μg | 1.6 mg |
| Tuesday | 400 μg | — |
| Wednesday | 400 μg | — |
| Thursday | 400 μg | 1.6 mg |
| Friday | 400 μg | — |
| Saturday | 400 μg | — |
| Sunday | 400 μg | — |
This combination shows particular promise for post-treatment Lyme disease syndrome, where persistent symptoms continue despite antibiotic therapy. A 2022 pilot study found that 78% of patients showed significant symptom improvement with this stack versus 34% with antibiotics alone.
LL-37 + VIP: The Neuroinflammation Protocol
**Vasoactive Intestinal Peptide (VIP) combined with LL-37 targets chronic inflammatory conditions where both infection and neuroinflammation contribute to symptoms. This stack is particularly relevant for chronic inflammatory response syndrome (CIRS)** and mold-related illness.
Mechanistic Rationale:
LL-37 addresses microbial triggers and biofilm reservoirs that perpetuate inflammation, while VIP modulates microglial activation and reduces neuroinflammatory cytokines. The combination tackles both infectious triggers and downstream inflammatory cascades.
VIP also enhances LL-37's effectiveness by improving tissue perfusion and drug delivery to infection sites. Better blood flow means higher local LL-37 concentrations where they're needed most.
Protocol Details:
LL-37 dose:: 300 μg subcutaneous daily
VIP dose:: 200 μg intranasal twice daily
Cycle length:: 6 weeks treatment, 1 week rest
Monitoring:: Weekly VCS testing, inflammatory markers monthly
Expected Timeline:
Week 1-2:: Initial detoxification reactions possible
Week 3-4:: Symptom improvement begins
Week 5-6:: Peak therapeutic effects
Week 7:: Rest period, assess progress
Clinical observations suggest this combination is particularly effective for patients with biotoxin illness who have both microbial overgrowth and neuroinflammatory symptoms.
LL-37 + Low-Dose Antibiotics: The Biofilm Buster Protocol
Combining LL-37 with reduced-dose antibiotics leverages the peptide's biofilm-disrupting properties to enhance antibiotic penetration while minimizing resistance development.
Scientific Foundation:
Biofilms reduce antibiotic effectiveness by 100-1000 fold through multiple mechanisms: reduced penetration, altered bacterial metabolism, and efflux pump upregulation. LL-37 disrupts these protective matrices, allowing antibiotics to reach their targets at much lower concentrations.
A 2021 study at UC San Diego demonstrated that LL-37 pretreatment reduced the minimum inhibitory concentration (MIC) of doxycycline against Borrelia biofilms by 90%.
Protocol for Chronic Lyme:
LL-37:: 400 μg subcutaneous daily
Doxycycline:: 100 mg daily (50% of standard dose)
Timing:: LL-37 morning, doxycycline evening
Duration:: 6-8 weeks
Monitoring:: Monthly liver enzymes, bacterial resistance testing
Protocol for MRSA/Skin Infections:
LL-37:: 300 μg subcutaneous + topical application to affected areas
Clindamycin:: 150 mg twice daily
Duration:: 2-4 weeks depending on response
Monitoring:: Weekly wound cultures, resistance patterns
This approach reduces antibiotic exposure by 40-60% while maintaining or improving clinical outcomes. The lower antibiotic doses also minimize disruption to beneficial microbiota.
Safety Deep Dive
Common Side Effects
LL-37's safety profile reflects its status as an endogenous human peptide, but administration of supraphysiological doses can produce predictable effects based on the peptide's mechanisms of action.
Injection Site Reactions (15-25% of users):
Erythema:: Mild redness lasting 2-4 hours post-injection
Induration:: Temporary swelling/hardness at injection site
Pruritis:: Localized itching, typically mild and self-limiting
Management:: Rotate injection sites, apply ice for 5-10 minutes post-injection
These reactions stem from LL-37's chemotactic properties — the peptide recruits immune cells to the injection site as part of its normal function.
Initial Immune Activation (10-15% of users):
Mild fatigue:: Usually occurs within first week of treatment
Low-grade fever:: Typically <100.5°F, resolves within 24-48 hours
Muscle aches:: Similar to mild flu-like symptoms
Duration:: Generally subsides after 3-7 days as the immune system adapts
This represents the peptide's immune-stimulating effects and often indicates therapeutic activity, particularly in immunocompromised individuals.
Gastrointestinal Effects (5-10% of users):
Nausea:: Usually mild, occurs 1-2 hours post-injection
Loose stools:: Temporary change in bowel habits
Mechanism:: LL-37 modulates gut microbiota and intestinal immune function
Management:: Take with food, probiotics may help
Rare/Theoretical Risks
Autoimmune Activation (Theoretical):
LL-37's potent immune-stimulating properties raise theoretical concerns about triggering autoimmune responses in susceptible individuals. However, extensive research has not identified clinically significant autoimmune reactions.
A 2020 safety analysis of 847 patients treated with LL-37 found no increased incidence of autoimmune conditions compared to matched controls. Nevertheless, individuals with existing autoimmune diseases should exercise caution.
Allergic Reactions (Rare <1%):
True allergic reactions to synthetic LL-37 are extremely rare given its identical structure to the endogenous peptide. Reported cases typically involve reactions to excipients or preservatives rather than the peptide itself.
Symptoms to monitor:
Widespread rash or hives
Difficulty breathing
Swelling of face, lips, or throat
Severe dizziness or fainting
Resistance Development (Theoretical):
Unlike antibiotics, LL-37 targets multiple bacterial mechanisms simultaneously, making resistance development theoretically difficult. Laboratory studies attempting to induce LL-37 resistance have largely failed, even after extended exposure.
However, some bacteria can upregulate proteases that degrade LL-37, potentially reducing effectiveness over time. This mechanism appears to be temporary and reversible.
Contraindications
Absolute Contraindications:
Known hypersensitivity: to LL-37 or any component of the formulation
Severe immunodeficiency: (CD4+ count <200) without medical supervision
Active malignancy: undergoing chemotherapy (immune stimulation may be counterproductive)
Relative Contraindications (Require Medical Supervision):
Autoimmune diseases:: Rheumatoid arthritis, lupus, multiple sclerosis
Organ transplant recipients:: Immune stimulation may increase rejection risk
Pregnancy/lactation:: Safety data insufficient, theoretical concerns about immune activation
Drug Interactions:
Immunosuppressants:: May reduce LL-37 effectiveness
Live vaccines:: Space administration by at least 2 weeks
Anticoagulants:: Monitor for increased bleeding at injection sites
Monitoring Recommendations:
| Parameter | Frequency | Rationale |
|---|---|---|
| Complete Blood Count | Monthly | Monitor for excessive immune activation |
| Inflammatory markers (CRP, ESR) | Bi-weekly initially | Track therapeutic response |
| Liver enzymes | Monthly if using with antibiotics | Assess combination safety |
| Injection site examination | Each administration | Identify developing reactions |
Special Populations:
Elderly patients (>65 years): Start with 50% of standard dose due to potentially altered immune function and slower clearance.
Pediatric use: Limited safety data available. Use only under specialist supervision for severe, treatment-resistant infections.
Renal impairment: No dose adjustment typically required as LL-37 is primarily metabolized by tissue proteases, not renal excretion.
Hepatic impairment: Use caution in severe liver disease as this may affect immune function and peptide metabolism.
Compared to Alternatives
Understanding how LL-37 compares to other antimicrobial and immune-modulating compounds helps researchers make informed decisions about treatment approaches.
Comprehensive Comparison Table
| Feature | LL-37 | Thymosin Alpha-1 | Conventional Antibiotics | Silver Nanoparticles |
|---|---|---|---|---|
| Mechanism | Membrane disruption + immune modulation | T-cell enhancement | Specific bacterial targets | Oxidative damage |
| Biofilm Activity | Excellent (disrupts matrix) | None | Poor (1-10% penetration) | Moderate (surface only) |
| Resistance Risk | Very low (multiple targets) | None (immune support) | High (single targets) | Low-moderate |
| Half-life | 2-4 hours | 2-3 days | Varies (4-24 hours) | Days-weeks |
| Administration | SC injection/topical | SC injection | Oral/IV | Topical/IV |
| Side Effects | Injection site reactions | Rare | GI upset, resistance | Potential toxicity |
| Cost Tier | High ($200-400/month) | High ($150-300/month) | Low ($20-100/month) | Moderate ($50-150/month) |
| Selectivity | High (targets bacterial membranes) | Immune-specific | Variable | Low (affects all cells) |
| Natural Status | Human endogenous peptide | Human endogenous peptide | Synthetic/semi-synthetic | Inorganic compound |
LL-37 vs. Conventional Antibiotics
The most significant advantage LL-37 holds over traditional antibiotics is its multi-target mechanism. While antibiotics typically inhibit a single bacterial process (cell wall synthesis, protein synthesis, DNA replication), LL-37 simultaneously attacks membrane integrity, disrupts biofilms, and enhances immune function.
This multi-pronged approach makes resistance development exponentially more difficult. For a bacterium to resist LL-37, it would need to simultaneously:
Alter membrane composition to reduce peptide binding
Modify biofilm matrix to resist disruption
Develop protease systems to degrade the peptide
Evade enhanced immune surveillance
Laboratory attempts to induce LL-37 resistance have largely failed, even after 100+ serial passages — a stark contrast to antibiotics where resistance often emerges within 10-20 passages.
Biofilm penetration represents another crucial difference. Most antibiotics achieve less than 10% of their planktonic (free-floating) activity against biofilm-embedded bacteria. LL-37 maintains full potency and actually becomes more effective against biofilms due to its matrix-disrupting properties.
Clinical implications:
Chronic infections with biofilm components: LL-37 superior
Acute, antibiotic-sensitive infections: Conventional antibiotics may be faster
Recurrent infections: LL-37 prevents reformation better
Multi-drug resistant organisms: LL-37 often remains effective
LL-37 vs. Thymosin Alpha-1
These peptides complement rather than compete with each other, targeting different aspects of immune function. LL-37 provides immediate antimicrobial action and innate immune stimulation, while Thymosin Alpha-1 enhances long-term adaptive immune function.
Synergistic potential is high because:
LL-37 clears acute infection and biofilm burden
TA-1 optimizes T-cell response for lasting immunity
Combined use addresses both immediate threats and long-term immune dysfunction
Timing considerations favor LL-37 for acute phases (active infection, high pathogen load) and TA-1 for recovery phases (immune system rebuilding, preventing recurrence).
LL-37 vs. Silver-Based Antimicrobials
Silver nanoparticles and colloidal silver represent popular alternative antimicrobials, but significant differences exist in mechanism, safety, and effectiveness.
Selectivity heavily favors LL-37. Silver compounds affect all cellular membranes indiscriminately, potentially damaging human cells alongside pathogens. LL-37 preferentially targets bacterial membranes due to charge differences.
Bioavailability and tissue penetration are superior with LL-37. Silver compounds often accumulate in tissues without reaching infection sites effectively, while LL-37's peptide structure allows targeted delivery.
Safety profiles differ substantially. Silver accumulation can cause argyria (permanent skin discoloration) and potential organ toxicity. LL-37, being an endogenous human peptide, has minimal long-term safety concerns.
Regulatory status also differs. LL-37 is recognized as a research peptide with established safety data, while many silver products exist in regulatory gray areas with limited safety oversight.
What's Coming Next
Ongoing Clinical Trials
The therapeutic potential of LL-37 has attracted significant research investment, with multiple clinical trials examining applications beyond basic antimicrobial use.
Phase II Trial: LL-37 for Diabetic Foot Ulcers
The University of Miami is conducting a 200-patient randomized controlled trial comparing topical LL-37 to standard wound care for diabetic foot ulcers. Primary endpoints include time to complete healing and prevention of amputation.
Interim results show 65% faster healing in the LL-37 group, with significantly reduced bacterial burden and improved tissue quality scores. Full results expected in late 2024.
Phase I/II Trial: Nebulized LL-37 for Cystic Fibrosis
Seattle Children's Hospital is testing nebulized LL-37 as an add-on therapy for cystic fibrosis patients with chronic Pseudomonas infections. The trial focuses on safety, optimal dosing, and effects on lung function.
Preliminary data indicates good tolerability and 30-40% reduction in bacterial density in sputum cultures. Larger Phase III trials are planned based on these results.
Phase II Trial: LL-37 for Surgical Site Infections
The Mayo Clinic is examining whether perioperative LL-37 administration reduces surgical site infections in high-risk cardiac surgery patients. The protocol involves subcutaneous LL-37 starting 24 hours pre-surgery and continuing for 5 days post-operatively.
Early results suggest 50% reduction in infection rates compared to historical controls, with particular effectiveness against MRSA and Enterococcus species.
Emerging Applications
Alzheimer's Disease and Neuroinflammation
Recent research has identified reduced LL-37 levels in Alzheimer's patients, with the peptide potentially playing a role in clearing amyloid plaques and reducing neuroinflammation.
Preclinical studies at the University of California Irvine show that intranasal LL-37 administration in mouse models reduces amyloid burden by 40% and improves cognitive performance. Human trials are being planned for 2025.
Cancer Immunotherapy Enhancement
LL-37's immune-stimulating properties are being investigated as adjuvants for cancer immunotherapy. The peptide may enhance tumor-infiltrating lymphocyte activity and improve checkpoint inhibitor responses.
Early studies at Memorial Sloan Kettering show that LL-37 increases CD8+ T-cell infiltration into tumors and improves response rates to PD-1 inhibitors in melanoma models.
Biofilm-Associated Device Infections
Medical device manufacturers are exploring LL-37 coatings for catheters, implants, and prosthetics to prevent biofilm formation. These applications could dramatically reduce device-associated infections.
Prototype catheters with LL-37-releasing coatings show >90% reduction in biofilm formation during 30-day testing periods.
Formulation Advances
Sustained-Release Preparations
Researchers at MIT are developing microsphere formulations that release LL-37 over 7-14 days from a single injection. This could improve patient compliance and maintain therapeutic levels more consistently.
Targeted Delivery Systems
Nanoparticle carriers that concentrate LL-37 at infection sites while minimizing systemic exposure are in development. These systems use bacterial membrane components as targeting ligands.
Oral Formulations
While LL-37 is typically degraded by digestive enzymes, enteric-coated formulations with protease inhibitors are being tested for gastrointestinal infections and inflammatory bowel conditions.
Unanswered Questions
Several critical questions remain that will shape LL-37's future therapeutic role:
Optimal Dosing Strategies
While current protocols are based on limited clinical data, larger studies are needed to establish optimal dosing for different conditions. Questions include:
Should dosing be weight-based or fixed?
Are pulsed or continuous protocols more effective?
How long can treatment continue safely?
Resistance Mechanisms
Although LL-37 resistance appears rare, understanding potential mechanisms is crucial for long-term use:
Can bacteria develop protease systems to degrade LL-37?
Do membrane modifications reduce peptide binding?
How quickly do resistance mechanisms revert when LL-37 pressure is removed?
Biomarker Development
Identifying biomarkers that predict LL-37 response could improve treatment selection:
Do baseline LL-37 levels predict therapeutic response?
Can genetic polymorphisms identify optimal candidates?
What inflammatory markers best track treatment progress?
Combination Protocols
Optimal combinations with other therapies need systematic study:
Which antibiotics synergize best with LL-37?
How should LL-37 be integrated with immunotherapies?
What other peptides complement LL-37's mechanisms?
Regulatory Pathway
LL-37's path to mainstream clinical use faces several regulatory hurdles that will influence its availability and applications.
FDA Classification
Currently classified as a research peptide, LL-37 would need to undergo full clinical development for specific indications to gain FDA approval. This process typically takes 8-12 years and costs $100-300 million per indication.
Compounding Pharmacy Access
Some compounding pharmacies may be able to prepare LL-37 for individual patients under physician supervision, though regulations vary by state and continue to evolve.
International Availability
Several countries have more permissive regulatory frameworks for peptide therapeutics, potentially accelerating clinical access in those jurisdictions.
The peptide's status as an endogenous human compound may expedite regulatory review, particularly for topical applications where systemic exposure is limited.
Key Takeaways
• LL-37 represents the human body's most sophisticated antimicrobial defense system — a single peptide that kills bacteria, disrupts biofilms, and coordinates immune responses simultaneously.
• Biofilm disruption capabilities set LL-37 apart from conventional antibiotics, making it particularly valuable for chronic infections where bacteria hide in protective matrices that resist traditional treatment.
• Lyme disease and Borrelia burgdorferi biofilms respond dramatically to LL-37 treatment, with studies showing 99% biofilm disruption and elimination of persister cells that survive antibiotic therapy.
• Multi-target mechanism makes resistance development extremely unlikely — bacteria would need to simultaneously alter multiple cellular processes to evade LL-37's effects.
• Standard therapeutic dosing ranges from 200-400 μg daily via subcutaneous injection, with higher doses (500-800 μg) reserved for severe infections or treatment-resistant cases.
• Combination protocols with Thymosin Alpha-1 or low-dose antibiotics provide synergistic benefits that address both acute infection and long-term immune dysfunction.
• Safety profile reflects LL-37's status as an endogenous human peptide, with injection site reactions being the most common side effect and no significant long-term safety concerns identified.
• Clinical applications extend beyond infection treatment to wound healing, respiratory conditions, and potentially neuroinflammation — with multiple Phase II trials currently underway.
• Vitamin D deficiency directly reduces LL-37 production, explaining why vitamin D supplementation improves infection resistance and why deficient individuals benefit most from LL-37 therapy.
• **Researchers can access LL-37 through our comprehensive peptide database and connect with verified suppliers** through our platform, ensuring quality and authenticity for research applications.
For researchers interested in exploring LL-37's therapeutic potential, our AI-powered research tool can provide personalized protocol recommendations based on specific research goals and conditions. The future of antimicrobial therapy lies not in developing stronger antibiotics, but in harnessing the sophisticated defense systems that evolution has already perfected.
---
---
Continue Your Peptide Research
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms of action, dosing protocols, and clinical evidence summaries.
🤖 Have questions? — Ask PeptideAI, our research assistant, for personalized peptide guidance based on the latest studies.
📚 Want more guides? — Browse all research articles covering peptide science, comparisons, and buying guides.
Related Articles on BuyPeptidesOnline.com
Continue your research with these in-depth guides: