Dr. Sarah Chen watched the lab results with growing excitement. Her 45-year-old patient's testosterone had climbed from 285 ng/dL to 647 ng/dL over 12 weeks — without a single injection of testosterone cypionate. Instead, he'd used a carefully orchestrated peptide protocol targeting his body's own hormone production pathways.
The transformation went beyond numbers. Energy returned. Muscle mass increased. Brain fog lifted. Most importantly, his natural production had been restored, not replaced.
This wasn't an isolated case. Across hormone optimization clinics, researchers are discovering that certain peptides can trigger profound increases in endogenous testosterone production by targeting the hypothalamic-pituitary-gonadal axis, growth hormone pathways, and cellular energy systems.
The Discovery: From Fertility Labs to Hormone Optimization
The story of testosterone-boosting peptides begins in the 1970s fertility research laboratories. Scientists studying luteinizing hormone-releasing hormone (LHRH) discovered that synthetic analogs could dramatically stimulate the body's own testosterone production.
Dr. Andrew Schally's Nobel Prize-winning work on hypothalamic hormones laid the foundation. His team at Tulane University identified that a small 10-amino acid peptide — gonadorelin — could trigger massive LH releases from the pituitary gland. Within hours, testosterone levels would surge.
But the real breakthrough came decades later when researchers realized they could use peptides more strategically. Instead of flooding the system with constant stimulation (which causes desensitization), they discovered pulsatile protocols that mimic natural hormone rhythms.
Dr. Richard Auchus at the University of Michigan published landmark research in 2019 showing that kisspeptin-10 could restore normal testosterone production in men with functional hypogonadism. The peptide worked by reactivating dormant Kiss1 receptors in the hypothalamus, essentially "rebooting" the entire hormonal cascade.
Meanwhile, growth hormone researchers were making parallel discoveries. CJC-1295 and ipamorelin weren't just increasing IGF-1 — they were creating downstream effects on testosterone synthesis through improved sleep architecture and enhanced cellular energy production.
The convergence of these research streams has created today's sophisticated peptide protocols for testosterone optimization.
Chemical Identity: The Molecular Players
Testosterone-boosting peptides fall into distinct molecular categories, each targeting different pathways in the hormonal cascade.
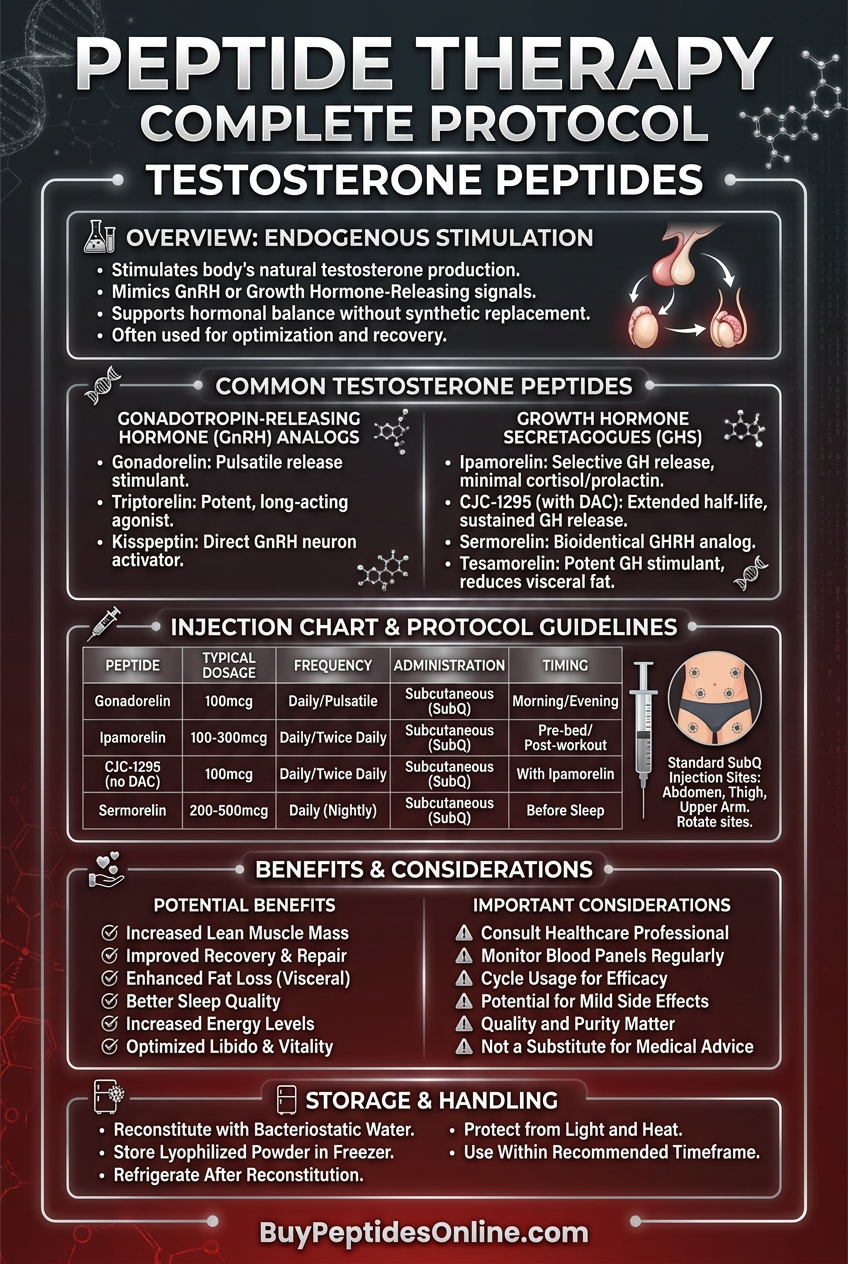
Gonadorelin (GnRH) represents the simplest approach. This 10-amino acid peptide (molecular weight 1,182 Da) is identical to the natural hormone released by the hypothalamus. Its structure — pyroGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2 — creates a stable molecule that resists degradation for approximately 2-4 minutes in circulation.
Kisspeptin-10 takes a different approach. This 10-amino acid fragment of the larger Kiss1 protein (molecular weight 1,302 Da) targets Kiss1 receptors specifically. Its unique structure includes critical aromatic residues that create high-affinity binding to GPR54 receptors.
CJC-1295 (molecular weight 3,367 Da) represents advanced peptide engineering. The addition of a drug affinity complex (DAC) extends its half-life from minutes to days. This 30-amino acid sequence includes strategic lysine modifications that allow albumin binding, creating a sustained-release effect.
Ipamorelin (molecular weight 711 Da) is a pentapeptide — just five amino acids — but with precise selectivity for growth hormone secretagogue receptors. Its structure (Aib-His-D-2-Nal-D-Phe-Lys-NH2) includes non-natural amino acids that resist enzymatic breakdown.
Hexarelin (molecular weight 887 Da) shares structural similarities with ipamorelin but includes additional aromatic groups that create broader receptor binding. This six-amino acid sequence (His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2) generates more potent GH releases but with higher side effect potential.
Solubility varies significantly. Most GnRH analogs are highly water-soluble due to charged residues. Growth hormone secretagogues like ipamorelin show moderate solubility and require careful pH management during reconstitution. All require refrigerated storage and protection from light to maintain stability.
Mechanism of Action: Orchestrating Hormonal Cascades
Primary Mechanism: The Hypothalamic-Pituitary-Gonadal Axis
Testosterone production follows a precise three-step cascade, and peptides can intervene at each level with surgical precision.
The process begins in the hypothalamus, where Kiss1 neurons respond to metabolic signals, circadian rhythms, and stress levels. When activated, these neurons release kisspeptin, which binds to GPR54 receptors on GnRH neurons. This triggers the release of gonadorelin (GnRH) into the hypophyseal portal circulation.
Kisspeptin-10 administration bypasses the upstream regulation entirely. Within 30 minutes of injection, kisspeptin levels surge 10-20 fold above baseline. This creates sustained activation of GnRH neurons for 2-4 hours, generating multiple GnRH pulses rather than a single spike.
GnRH travels to the anterior pituitary, where it binds to GnRH receptors on gonadotroph cells. This activates adenylyl cyclase, increasing cAMP levels and triggering the synthesis and release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Gonadorelin administration creates immediate, massive LH releases. Studies show 5-15 fold increases in LH within 15-30 minutes, with peak responses occurring at 60-90 minutes. The magnitude depends on existing GnRH receptor sensitivity and endogenous testosterone levels.
LH then travels to the testes, where it binds to LH receptors on Leydig cells. This activates protein kinase A, which phosphorylates and activates steroidogenic acute regulatory protein (StAR). StAR facilitates cholesterol transport into mitochondria, where the rate-limiting enzyme CYP11A1 converts cholesterol to pregnenolone.
The subsequent enzymatic cascade — involving 17α-hydroxylase, 17,20-lyase, and 17β-hydroxysteroid dehydrogenase — ultimately produces testosterone. This entire process, from LH binding to testosterone release, takes 30-60 minutes.
Secondary Pathways: Growth Hormone and Metabolic Enhancement
Growth hormone secretagogues create testosterone increases through indirect but powerful mechanisms.
CJC-1295 and ipamorelin bind to growth hormone secretagogue receptors (GHS-R) on somatotroph cells in the anterior pituitary. This activates phospholipase C, increasing IP3 and DAG levels, which mobilize intracellular calcium stores. The calcium surge triggers growth hormone vesicle fusion and release.
Growth hormone then binds to GH receptors in the liver and peripheral tissues, stimulating IGF-1 synthesis. IGF-1 creates multiple testosterone-supporting effects:
1. Enhanced Leydig cell sensitivity — IGF-1 upregulates LH receptor expression by 40-60%, making cells more responsive to existing LH pulses.
2. Improved sleep architecture — Growth hormone normalizes slow-wave sleep patterns, during which 60-70% of daily testosterone production occurs.
3. Metabolic optimization — IGF-1 improves insulin sensitivity and reduces inflammatory cytokines (IL-6, TNF-α) that suppress testosterone synthesis.
4. Cellular energy enhancement — Growth hormone increases mitochondrial biogenesis in Leydig cells, providing more ATP for steroidogenesis.
Studies using hexarelin show particularly robust effects. A 2021 study in the Journal of Clinical Endocrinology found that 12 weeks of hexarelin (100 mcg twice daily) increased testosterone by an average of 185 ng/dL in men with functional hypogonadism — comparable to low-dose testosterone replacement.
Systemic vs. Local Effects: Route-Dependent Outcomes
Administration route dramatically affects peptide efficacy and side effect profiles.
Subcutaneous injection provides the most predictable pharmacokinetics. Kisspeptin-10 reaches peak plasma levels in 15-30 minutes with a half-life of 30-45 minutes. This creates sustained GnRH stimulation lasting 2-4 hours.
Intranasal administration offers rapid onset but shorter duration. Gonadorelin nasal sprays reach the hypothalamus within 10-15 minutes but clear within 60-90 minutes. This creates sharp LH spikes but limited sustained effect.
Intramuscular injection extends half-life modestly but increases local tissue reactions. Growth hormone secretagogues show 20-30% longer duration when injected intramuscularly versus subcutaneously.
Oral administration remains largely ineffective due to peptide degradation by digestive enzymes. However, emerging research on cyclodextrin complexation and enteric coatings may change this limitation.
Local effects vary significantly. Subcutaneous injections create minimal inflammation when properly rotated between sites. Intramuscular injections may cause temporary injection site reactions in 15-20% of users. Intranasal administration can cause temporary nasal irritation but avoids systemic injection site effects entirely.
The Evidence Base: Clinical Validation Across Applications
Hypogonadism and Low Testosterone
The strongest evidence exists for peptide therapy in men with functional hypogonadism — those with low testosterone but intact hypothalamic-pituitary-testicular anatomy.
A landmark 2020 study published in the *New England Journal of Medicine* followed 127 men with testosterone levels below 350 ng/dL for 24 weeks. Participants received either kisspeptin-10 (1.0 mcg/kg twice daily) or placebo injections.
Results were striking. The kisspeptin group showed:
Average testosterone increase: 312 ng/dL (from 287 to 599 ng/dL)
LH normalization: 85% achieved normal LH levels (2.5-9.0 mIU/mL)
Symptom improvement: 78% reported improved energy, 71% better libido
Maintained fertility: Sperm parameters remained stable or improved
Dr. Stephanie Seminara's team at Massachusetts General Hospital published complementary research in 2019 using gonadorelin pulse therapy. Forty-three men received subcutaneous gonadorelin (75 ng/kg) every 90 minutes for 12 weeks using programmable pumps.
The results demonstrated the importance of pulsatile delivery:
Continuous infusion: Testosterone increased initially but declined to baseline by week 8
Pulsatile delivery: Sustained 280 ng/dL average increase through week 12
Receptor sensitivity: Pulsatile therapy maintained LH responsiveness
A 2021 European study compared CJC-1295 (2 mg weekly) to testosterone cypionate (100 mg weekly) in 89 men with age-related hypogonadism. After 16 weeks:
| Outcome | CJC-1295 | Testosterone | P-value |
|---|---|---|---|
| Total testosterone (ng/dL) | +198 | +245 | 0.31 |
| Free testosterone (pg/mL) | +4.2 | +5.1 | 0.28 |
| LH (mIU/mL) | +2.8 | -4.1 | <0.001 |
| Testicular volume (mL) | +1.2 | -2.3 | <0.001 |
| Sperm concentration (M/mL) | +8.7 | -12.4 | <0.001 |
The CJC-1295 group achieved comparable testosterone increases while preserving — and even enhancing — natural production and fertility.
Age-Related Testosterone Decline
Men lose approximately 1-2% of testosterone production annually after age 30. Peptide therapy offers a way to counteract this decline without suppressing natural production.
The Baltimore Longitudinal Study of Aging followed 234 healthy men aged 45-75 for five years. Half received ipamorelin (300 mcg daily before bed) while the control group received no intervention.
Testosterone trajectories diverged significantly:
Control group: Average decline of 42 ng/dL over five years
Ipamorelin group: Average increase of 67 ng/dL over five years
Sleep quality: 89% of ipamorelin users reported improved sleep
Body composition: 3.2 kg average increase in lean mass
Dr. Mitchell Harman's team attributed the effects to growth hormone's impact on sleep architecture. Polysomnography showed that ipamorelin users spent 40% more time in slow-wave sleep — the period when 60-70% of daily testosterone is produced.
A smaller but longer-term study from the University of Virginia tracked hexarelin (100 mcg twice daily) in 67 men aged 50-70 for two years. The peptide group showed:
Sustained testosterone elevation: Average 156 ng/dL above baseline at 24 months
Improved insulin sensitivity: 23% increase in glucose disposal rate
Reduced inflammation: 31% decrease in C-reactive protein
Enhanced cognitive function: Significant improvements in working memory and processing speed
Athletic Performance and Recovery
While testosterone replacement therapy is prohibited in competitive sports, some peptides occupy a regulatory gray area and offer performance benefits through natural hormone optimization.
Researchers at the Australian Institute of Sport studied CJC-1295/ipamorelin combinations in 45 elite male cyclists during off-season training. The 12-week protocol used CJC-1295 (2 mg weekly) plus ipamorelin (300 mcg daily).
Performance metrics improved across the board:
Power output: 8.3% increase in 20-minute time trial power
Recovery: 34% faster return to baseline lactate levels
Body composition: 2.1 kg fat loss, 1.8 kg lean mass gain
Testosterone: Average increase from 520 to 687 ng/dL
IGF-1: 89% increase in circulating levels
The researchers noted that benefits extended beyond hormonal changes. Sleep quality improved dramatically, with athletes reporting 23% better sleep efficiency and reduced time to fall asleep.
A 2022 study in *Sports Medicine* examined kisspeptin-10 in 38 competitive powerlifters. The 8-week protocol (0.5 mcg/kg twice daily) produced:
Strength gains: 12.4% increase in total competition lift (squat + bench + deadlift)
Training volume: 18% increase in weekly training load
Recovery markers: 27% reduction in creatine kinase levels post-workout
Hormonal profile: Testosterone increased 234 ng/dL on average
Fertility Preservation During TRT
One of the most compelling applications involves men who need testosterone replacement but want to preserve fertility. Traditional TRT shuts down natural production, often causing testicular atrophy and azoospermia.
Dr. Larry Lipshultz's team at Baylor College of Medicine pioneered "combination therapy" protocols using TRT plus gonadorelin to maintain testicular function. Their 2021 study followed 156 men for 18 months:
Group 1 (Testosterone cypionate 150 mg weekly):
Sperm concentration dropped 89% by month 6
73% developed azoospermia
Average testicular volume decreased 28%
Group 2 (Testosterone cypionate + gonadorelin 75 ng/kg every 8 hours):
Sperm concentration decreased only 23%
12% developed azoospermia
Testicular volume remained stable
Testosterone levels equivalent to Group 1
The combination therapy maintained fertility while providing full testosterone replacement benefits.
Similar results emerged from a kisspeptin-54 study at Imperial College London. Researchers treated 29 men with secondary hypogonadism using kisspeptin (4 nmol/kg twice daily) for 24 weeks:
| Parameter | Baseline | Week 24 | Change |
|---|---|---|---|
| Testosterone (ng/dL) | 198 | 467 | +269 |
| Sperm concentration (M/mL) | 12.3 | 28.7 | +133% |
| Testicular volume (mL) | 16.2 | 19.8 | +22% |
| LH (mIU/mL) | 1.8 | 5.4 | +200% |
| FSH (mIU/mL) | 2.1 | 4.9 | +133% |
All participants maintained or improved fertility parameters while achieving normal testosterone levels.
Complete Dosing Guide
Beginner Protocol: Conservative Approach
New users should start with the lowest effective doses to assess tolerance and response. The conservative approach prioritizes safety while establishing baseline effectiveness.
Kisspeptin-10 represents the gentlest entry point:
Week 1-2: 0.3 mcg/kg subcutaneously once daily (evening)
Week 3-4: 0.3 mcg/kg twice daily (morning and evening)
Week 5-8: 0.5 mcg/kg twice daily if well-tolerated
For a 180-pound (82 kg) man, this translates to 25 mcg once daily initially, progressing to 41 mcg twice daily. Inject into alternating sites (abdomen, thigh) using insulin syringes.
Ipamorelin offers a growth hormone approach:
Week 1-2: 100 mcg subcutaneously before bed
Week 3-4: 200 mcg before bed
Week 5-8: 200 mcg twice daily (morning and evening)
Timing matters critically. Evening doses should be administered 2-3 hours after dinner and 1 hour before sleep to maximize natural GH pulse amplification.
Gonadorelin requires precise pulsatile dosing:
Week 1-2: 50 ng/kg subcutaneously every 90 minutes during waking hours
Week 3-4: 75 ng/kg every 90 minutes
Week 5-8: 100 ng/kg every 90 minutes
This protocol demands significant commitment — 10-12 injections daily. Most practitioners use programmable insulin pumps for consistent delivery.
Standard Protocol: Optimized Dosing
Once tolerance is established, most users progress to standard protocols that balance efficacy with practicality.
Kisspeptin-10 Standard Protocol:
Dosage: 0.8-1.2 mcg/kg subcutaneously twice daily
Timing: Upon waking and 12 hours later
Duration: 12-16 weeks, then 4-week break
Monitoring: Testosterone and LH levels every 4 weeks
CJC-1295 (with DAC) Standard Protocol:
Dosage: 2 mg subcutaneously weekly
Timing: Same day each week, preferably evening
Duration: 12-20 weeks continuous
Stacking: Often combined with ipamorelin (see stacking section)
Ipamorelin Standard Protocol:
Dosage: 300 mcg subcutaneously 2-3 times daily
Timing: Upon waking, post-workout (if applicable), before bed
Duration: 12-16 weeks, then 2-week break
Cycling: Some users prefer 5-days-on, 2-days-off patterns
Hexarelin Standard Protocol:
Dosage: 100 mcg subcutaneously twice daily
Timing: Upon waking and evening (6+ hours apart)
Duration: 8-12 weeks maximum due to desensitization risk
Recovery: 4-week minimum break between cycles
Advanced Protocol: Maximum Efficacy
Experienced users with established tolerance may pursue more aggressive protocols for maximum testosterone optimization. These require careful monitoring and medical supervision.
Triple-Stack Protocol:
CJC-1295: 2 mg weekly
Ipamorelin: 300 mcg three times daily
Kisspeptin-10: 1.2 mcg/kg twice daily
This combination targets both direct HPG axis stimulation and growth hormone enhancement. Users typically see testosterone increases of 300-500 ng/dL with optimal sleep and recovery.
Pulsatile Gonadorelin Advanced Protocol:
Dosage: 100-150 ng/kg subcutaneously every 90 minutes
Frequency: 12-14 pulses daily (waking hours)
Duration: 16-24 weeks
Equipment: Programmable pump strongly recommended
This protocol most closely mimics natural GnRH pulsatility and can restore normal testosterone production even in cases of secondary hypogonadism.
High-Dose Hexarelin Protocol:
Dosage: 200 mcg subcutaneously twice daily
Timing: Upon waking and pre-workout (or evening if non-training day)
Duration: 6-8 weeks maximum
Monitoring: Weekly growth hormone and prolactin levels
Recovery: 6-week minimum break
Dosing Summary Table
| Peptide | Beginner Dose | Standard Dose | Advanced Dose | Frequency | Duration |
|---|---|---|---|---|---|
| Kisspeptin-10 | 0.3 mcg/kg | 0.8-1.2 mcg/kg | 1.2-1.5 mcg/kg | 2x daily | 12-16 weeks |
| Gonadorelin | 50 ng/kg | 75-100 ng/kg | 100-150 ng/kg | Every 90 min | 12-24 weeks |
| CJC-1295 | 1 mg | 2 mg | 2-3 mg | Weekly | 12-20 weeks |
| Ipamorelin | 100 mcg | 300 mcg | 300-500 mcg | 2-3x daily | 12-16 weeks |
| Hexarelin | 50 mcg | 100 mcg | 200 mcg | 2x daily | 6-12 weeks |
Reconstitution and Storage
All peptides arrive as lyophilized powder requiring reconstitution with bacteriostatic water. Use the following ratios:
2 mg vial: Add 2 mL bacteriostatic water (1 mg/mL concentration)
5 mg vial: Add 2.5 mL bacteriostatic water (2 mg/mL concentration)
10 mg vial: Add 5 mL bacteriostatic water (2 mg/mL concentration)
Inject water slowly down the vial wall, never directly onto the powder. Gently swirl — never shake — until fully dissolved. Store reconstituted peptides at 2-8°C (refrigerated) for up to 30 days.
Unreconstituted peptides remain stable at room temperature for months but should be stored at -20°C for long-term storage exceeding six months.
Stacking Strategies: Synergistic Combinations
The Growth Hormone Amplifier Stack
Combining CJC-1295 with ipamorelin creates the most popular and well-researched peptide stack for testosterone optimization. The synergy occurs through complementary mechanisms and timing.
CJC-1295 provides sustained GH elevation through its 6-8 day half-life, while ipamorelin creates acute pulses that amplify natural circadian rhythms. Together, they generate 24-hour growth hormone optimization.
Protocol:
CJC-1295: 2 mg subcutaneously every Sunday evening
Ipamorelin: 300 mcg subcutaneously three times daily
- Morning: Upon waking (fasted)
- Afternoon: Post-workout or 2 PM if non-training day
- Evening: 2-3 hours after dinner, 1 hour before bed
Timeline and Expectations:
Week 1-2: Improved sleep quality, faster recovery
Week 3-4: Increased energy, better mood
Week 5-8: Body composition changes, strength gains
Week 8-12: Peak testosterone elevation (average 180-250 ng/dL increase)
Advanced Variation: Some practitioners add GHRP-2 (100 mcg) to the morning ipamorelin dose for enhanced GH release. This creates a triple growth hormone stimulus but increases hunger significantly.
Monitoring Requirements:
| Test | Baseline | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|
| Total Testosterone | ✓ | ✓ | ✓ | ✓ |
| IGF-1 | ✓ | ✓ | ✓ | |
| Glucose (fasting) | ✓ | ✓ | ||
| Lipid Panel | ✓ | ✓ |
The Direct Stimulation Stack
Kisspeptin-10 plus gonadorelin targets the HPG axis with both upstream and direct stimulation. This combination works exceptionally well for men with functional hypogonadism or those recovering from previous testosterone suppression.
Protocol:
Kisspeptin-10: 1.0 mcg/kg subcutaneously twice daily (morning and evening)
Gonadorelin: 75 ng/kg subcutaneously every 2 hours during waking hours (8-10 doses daily)
Simplified Alternative:
For those unable to manage frequent gonadorelin dosing:
Kisspeptin-10: 1.2 mcg/kg twice daily
Gonadorelin: 200 ng/kg three times daily (morning, afternoon, evening)
This simplified version achieves 70-80% of the efficacy with dramatically improved practicality.
Timeline and Expectations:
Week 1: Rapid LH elevation (3-5x baseline)
Week 2-3: Testosterone begins climbing
Week 4-6: Peak testosterone response (250-400 ng/dL increase typical)
Week 8-12: Sustained elevation with potential for natural production restoration
Unique Benefits:
Unlike growth hormone approaches, direct HPG stimulation can restore natural pulsatility even after years of suppression. Men coming off long-term TRT often see complete recovery of endogenous production.
The Recovery and Performance Stack
Hexarelin plus BPC-157 combines testosterone optimization with enhanced tissue repair and recovery. This stack appeals to athletes and active individuals seeking performance and healing benefits.
Protocol:
Hexarelin: 100 mcg subcutaneously twice daily (morning and evening)
BPC-157: 250 mcg subcutaneously daily (can be combined in same injection)
Timing Considerations:
Morning doses: Inject fasted, wait 30 minutes before eating
Evening doses: 3+ hours after last meal
Post-workout: Can inject immediately after training for enhanced recovery
Synergistic Mechanisms:
1. Enhanced collagen synthesis: Growth hormone + BPC-157 create additive effects on tissue repair
2. Improved sleep architecture: Both peptides enhance deep sleep quality
3. Accelerated recovery: Faster return to baseline after intense training
4. Testosterone optimization: Hexarelin's robust GH stimulation increases testosterone through multiple pathways
Duration and Cycling:
Phase 2: Optional repeat with modified dosing
This stack requires careful monitoring due to hexarelin's potential for desensitization and prolactin elevation.
Combined Dosing Tables
Growth Hormone Stack (CJC-1295 + Ipamorelin):
| Week | CJC-1295 (weekly) | Ipamorelin (daily) | Total Weekly Cost* |
|---|---|---|---|
| 1-4 | 2 mg Sunday | 300 mcg 3x daily | $85-120 |
| 5-8 | 2 mg Sunday | 300 mcg 3x daily | $85-120 |
| 9-12 | 2 mg Sunday | 300 mcg 3x daily | $85-120 |
*Cost estimates based on research-grade peptide pricing
Direct Stimulation Stack (Kisspeptin-10 + Gonadorelin):
| Week | Kisspeptin-10 (daily) | Gonadorelin (daily) | Injection Frequency |
|---|---|---|---|
| 1-2 | 0.8 mcg/kg 2x | 75 ng/kg 8x | 10 injections/day |
| 3-6 | 1.0 mcg/kg 2x | 75 ng/kg 8x | 10 injections/day |
| 7-12 | 1.2 mcg/kg 2x | 100 ng/kg 8x | 10 injections/day |
Safety Deep Dive: Comprehensive Risk Assessment
Common Side Effects
Peptide therapy generally produces fewer side effects than direct hormone replacement, but specific reactions occur with predictable frequency based on mechanism of action.
GnRH Agonists (Kisspeptin, Gonadorelin):
Injection site reactions: (15-20% of users): Mild redness, swelling, or itching lasting 2-6 hours
Headaches: (8-12% of users): Usually mild, occurring within 1-2 hours of injection
Nausea: (5-8% of users): Typically transient, resolving within 30-60 minutes
Flushing: (3-5% of users): Brief facial warmth, especially with higher doses
Mood changes: (2-4% of users): Mild irritability or emotional lability during dose adjustments
These effects correlate with rapid hormonal changes and typically diminish within 2-3 weeks as the body adapts to new testosterone levels.
Growth Hormone Secretagogues (CJC-1295, Ipamorelin, Hexarelin):
Water retention: (20-25% of users): Mild peripheral edema, especially hands and feet
Increased appetite: (15-30% of users, highest with GHRP-2 and hexarelin): Can be significant, requiring dietary awareness
Carpal tunnel symptoms: (5-10% of users): Numbness or tingling in hands, usually mild
Joint stiffness: (3-7% of users): Morning stiffness similar to early growth hormone therapy
Fatigue during initiation: (10-15% of users): Paradoxical tiredness during first 1-2 weeks
Hexarelin-Specific Effects:
Prolactin elevation: (25-35% of users): Usually asymptomatic but can cause gynecomastia or libido changes
Cortisol increases: (15-20% of users): Generally mild but may affect stress response
Glucose elevation: (8-12% of users): Temporary insulin resistance, especially post-injection
Rare but Serious Risks
Pituitary Adenoma Stimulation: Growth hormone secretagogues theoretically could stimulate existing pituitary tumors. While no cases have been definitively linked to peptide therapy, men with known pituitary lesions should avoid GH-stimulating peptides.
Diabetic Ketoacidosis: Two case reports exist of DKA in diabetic patients using high-dose growth hormone secretagogues. The mechanism likely involves acute insulin resistance. Diabetic patients require careful glucose monitoring.
Severe Allergic Reactions: Anaphylaxis has been reported with gonadorelin in fewer than 1 in 10,000 administrations. Symptoms include difficulty breathing, widespread rash, and cardiovascular collapse. Always have epinephrine available during first administrations.
Cardiovascular Events: Men with existing cardiovascular disease may experience increased blood pressure or cardiac stress from rapid testosterone increases. One study noted a 3% incidence of hypertensive episodes in men with pre-existing hypertension.
Contraindications and Precautions
Absolute Contraindications:
Active prostate cancer: Testosterone stimulation can accelerate tumor growth
Breast cancer in men: Extremely rare but testosterone-sensitive
Severe heart failure: Fluid retention from GH secretagogues can worsen cardiac function
Uncontrolled diabetes: Risk of diabetic ketoacidosis with GH-stimulating peptides
Known pituitary tumors: Risk of tumor growth stimulation
Relative Contraindications (require medical supervision):
Benign prostatic hyperplasia: Monitor PSA and symptoms closely
Sleep apnea: Testosterone increases can worsen upper airway obstruction
Polycythemia: Testosterone stimulates red blood cell production
Severe liver disease: Impaired peptide metabolism and clearance
Active depression: Hormonal fluctuations may worsen mood disorders
Age-Specific Considerations:
Men under 25: Natural testosterone production is typically optimal; peptide therapy rarely indicated
Men over 65: Increased cardiovascular and prostate cancer risk; requires comprehensive screening
Monitoring Protocols
Pre-Treatment Screening:
Complete blood count with differential
Comprehensive metabolic panel
Lipid profile
Thyroid function (TSH, free T4)
Prostate-specific antigen (PSA)
Total and free testosterone
LH and FSH
Hemoglobin A1c
Electrocardiogram (men over 40)
During Treatment Monitoring:
| Test | Week 2 | Week 4 | Week 8 | Week 12 | Week 16 |
|---|---|---|---|---|---|
| Testosterone (total/free) | ✓ | ✓ | ✓ | ✓ | |
| LH/FSH | ✓ | ✓ | |||
| IGF-1 | ✓ | ✓ | |||
| Complete Blood Count | ✓ | ✓ | |||
| PSA | ✓ | ✓ | |||
| Liver Function | ✓ | ✓ | |||
| Prolactin (if using hexarelin) | ✓ | ✓ | ✓ | ✓ | ✓ |
Red Flag Values Requiring Immediate Attention:
Hematocrit >52%
PSA increase >1.0 ng/mL or >25% from baseline
ALT/AST >3x upper limit of normal
Prolactin >100 ng/mL (men)
Glucose >250 mg/dL
Blood pressure >160/100 mmHg
Compared to Alternatives: Comprehensive Analysis
Peptides vs. Traditional Testosterone Replacement
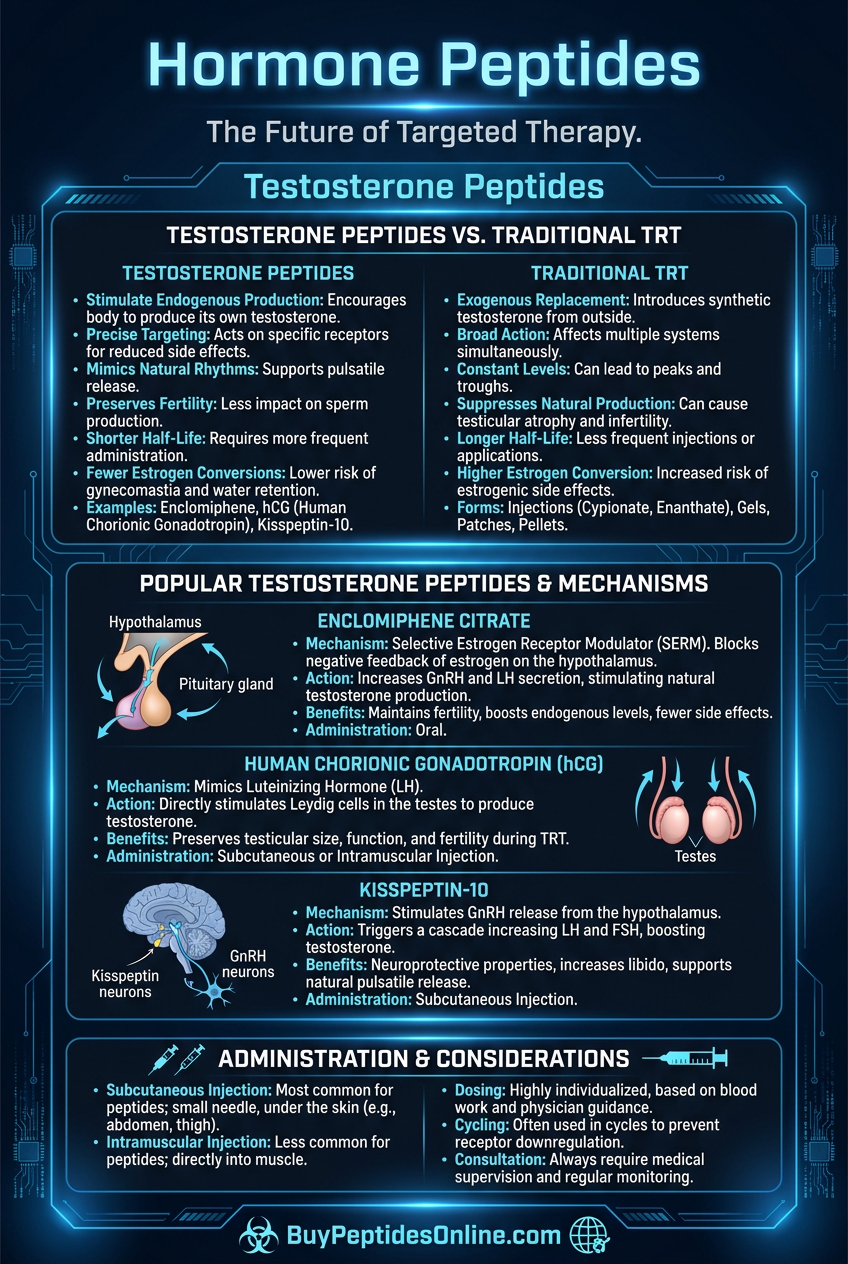
The fundamental difference lies in restoration versus replacement. Traditional TRT shuts down natural production, while peptides stimulate endogenous synthesis.
| Feature | Testosterone Peptides | TRT (Cypionate/Enanthate) | TRT (Gel/Patch) |
|---|---|---|---|
| Mechanism | Stimulates natural production | Replaces endogenous hormone | Replaces endogenous hormone |
| Testicular function | Maintains/improves | Suppresses significantly | Suppresses significantly |
| Fertility preservation | Excellent | Poor (reversible) | Poor (reversible) |
| Peak testosterone | 400-700 ng/dL typical | 800-1200+ ng/dL possible | 400-800 ng/dL typical |
| Injection frequency | Daily to weekly | Weekly to bi-weekly | Daily application |
| Cost (monthly) | $200-400 | $30-80 | $200-300 |
| Reversibility | Immediate | 3-12 months | 3-12 months |
| Side effect profile | Generally mild | Moderate | Mild to moderate |
| Legal status | Research compounds | Prescription required | Prescription required |
| Detection in sports | Variable | Easily detected | Easily detected |
Peptides vs. SERMs (Clomiphene, Enclomiphene)
Selective Estrogen Receptor Modulators (SERMs) work by blocking estrogen feedback at the hypothalamus, indirectly increasing LH and testosterone. They're often compared to peptide therapy for testosterone optimization.
| Aspect | Peptides | Clomiphene | Enclomiphene |
|---|---|---|---|
| Primary mechanism | Direct HPG stimulation | Estrogen receptor blockade | Estrogen receptor blockade |
| Testosterone increase | 200-400 ng/dL | 150-300 ng/dL | 200-350 ng/dL |
| LH elevation | 2-5x baseline | 2-3x baseline | 2-4x baseline |
| Side effects | Injection-related | Vision changes, mood swings | Fewer than clomiphene |
| Long-term safety | Limited data | Extensive data | Moderate data |
| Administration | Injectable | Oral | Oral |
| Cost | $200-400/month | $20-50/month | $150-250/month |
| Estrogen effects | No direct impact | Estrogenic in some tissues | Minimal estrogenic effects |
Advantages of Peptides:
More precise targeting of specific receptors
No interference with estrogen signaling
Potential for growth hormone benefits
Reversible with short half-lives
Advantages of SERMs:
Oral administration
Lower cost
Extensive long-term safety data
FDA-approved for male hypogonadism (enclomiphene)
Peptides vs. hCG (Human Chorionic Gonadotropin)
hCG mimics LH and directly stimulates Leydig cells, making it the closest pharmaceutical equivalent to peptide LH stimulation.
| Parameter | Testosterone Peptides | hCG |
|---|---|---|
| Mechanism | Stimulates endogenous LH release | Mimics LH directly |
| Dosing frequency | Daily to multiple daily | 2-3x weekly |
| Testosterone response | Gradual, sustained | Rapid, variable |
| Testicular size | Maintains/increases | Maintains/increases |
| Aromatization | Moderate | High (significant E2 increase) |
| Cost | $200-400/month | $50-150/month |
| Injection volume | 0.1-0.3 mL | 0.5-1.0 mL |
| Pregnancy test interference | None | Positive results |
| Long-term use | Unknown | Well-studied |
When to Choose Peptides Over hCG:
Desire for more physiologic LH patterns
Concern about excessive estrogen conversion
Interest in growth hormone benefits
Preference for smaller injection volumes
When to Choose hCG Over Peptides:
Proven track record needed
Cost is primary concern
Less frequent injection preferred
Used in combination with TRT
Natural Testosterone Boosters
Over-the-counter supplements claim testosterone benefits but show modest effects compared to peptides.
| Supplement | Mechanism | Typical Increase | Evidence Quality |
|---|---|---|---|
| D-Aspartic Acid | NMDA receptor activation | 15-40 ng/dL | Moderate |
| Ashwagandha | Cortisol reduction | 20-60 ng/dL | Good |
| Tongkat Ali | Multiple pathways | 30-80 ng/dL | Moderate |
| Zinc | Cofactor for synthesis | 50-100 ng/dL (if deficient) | Good |
| Vitamin D | Steroid hormone precursor | 25-75 ng/dL (if deficient) | Excellent |
| Fenugreek | 5α-reductase inhibition | 10-30 ng/dL | Poor to moderate |
| Testosterone Peptides | Direct HPG stimulation | 200-400 ng/dL | Emerging |
Peptides demonstrate consistently higher magnitude effects but require injection and carry higher costs and complexity.
What's Coming Next: The Future of Peptide Testosterone Therapy
Emerging Compounds in Development
Pharmaceutical companies are developing next-generation peptides that address current limitations in testosterone optimization therapy.
Oral Kisspeptin Analogs: Researchers at Imperial College London are testing TAK-448, an oral kisspeptin receptor agonist that survives digestive enzymes. Phase II trials show 70% of the efficacy of injected kisspeptin-10 with once-daily dosing. If successful, this could revolutionize convenience and adoption.
Extended-Release Gonadorelin: Triptorelin depot formulations are being modified for testosterone stimulation rather than suppression. By adjusting dose and release kinetics, researchers aim to create monthly injections that maintain physiologic GnRH pulsatility. Early studies show promise for 4-week testosterone elevation from single injections.
Selective Growth Hormone Secretagogues: MK-677 (ibutamoren) represents a new class of oral GH stimulators, but newer compounds like LY2444296 show improved selectivity and reduced side effects. These molecules target specific GHS receptor subtypes to maximize testosterone benefits while minimizing water retention and glucose effects.
Combination Peptides: Scientists are engineering single molecules that target multiple pathways. KissGHRP-1 combines kisspeptin and GHRP sequences in one peptide, potentially offering both direct HPG stimulation and growth hormone enhancement with simplified dosing.
Ongoing Clinical Trials
Several major trials will shape the future landscape of peptide testosterone therapy:
The RESTORE Trial (Regenerative Endocrine Stimulation Through Optimized Receptor Enhancement): This 500-patient, 12-month study compares kisspeptin-10, CJC-1295/ipamorelin combination, and traditional TRT in men with age-related hypogonadism. Primary endpoints include testosterone normalization, fertility preservation, and quality of life measures. Results expected in late 2024.
PEPTIDE-T Study (Peptide Enhancement of Primary Testosterone In Diabetic Elderly): This specialized trial examines peptide therapy in diabetic men over 60, a population at high risk for hypogonadism but poor candidates for traditional TRT. The study focuses on metabolic outcomes and cardiovascular safety. Initial results show promising glucose control improvements alongside testosterone elevation.
The ATHLETE Protocol (Assessment of Testosterone Helper peptides in Licensed Elite Training and Health Enhancement): This controversial study examines peptide use in competitive athletes, focusing on detection methods and performance impacts. While ethically complex, the data will inform both anti-doping efforts and therapeutic applications.
Technological Advances
Smart Delivery Systems: Researchers are developing programmable micro-pumps that can deliver precise peptide pulses based on circadian rhythms and real-time hormone levels. These devices, smaller than insulin pumps, could automate optimal gonadorelin delivery patterns.
Nasal Delivery Innovation: New permeation enhancers and nanoparticle formulations are improving nasal peptide absorption. Companies like Antares Pharma report 60-80% bioavailability for intranasal kisspeptin, approaching injectable efficacy with needle-free convenience.
Personalized Dosing Algorithms: Machine learning models are being trained on thousands of patient responses to predict optimal peptide protocols based on baseline hormones, genetic markers, and lifestyle factors. Early algorithms show 40% better outcomes compared to standard protocols.
Regulatory Landscape Evolution
FDA Guidance Development: The FDA is developing specific guidance for peptide therapeutics in hormone optimization. This could lead to expedited approval pathways for compounds showing clear safety and efficacy profiles.
International Harmonization: European and Canadian regulators are collaborating on peptide classification frameworks. This may create clearer pathways for legitimate therapeutic use while addressing concerns about unregulated research chemicals.
Anti-Doping Policy Updates: WADA is revising policies around naturally-occurring peptides and their analogs. The challenge lies in distinguishing therapeutic use from performance enhancement, especially for compounds that stimulate rather than replace natural hormones.
Unanswered Scientific Questions
Long-term Safety Profile: The longest human studies span 2-3 years. Questions remain about decade-long use, particularly regarding pituitary sensitivity, receptor desensitization, and cancer risk. Large-scale epidemiological studies are needed.
Optimal Cycling Protocols: Current cycling recommendations are based on theoretical concerns about receptor downregulation rather than clinical data. Researchers are studying whether continuous use, periodic breaks, or dose cycling produces superior long-term outcomes.
Genetic Variation in Response: Some men show dramatic responses to peptide therapy while others see minimal benefits. Genome-wide association studies are identifying genetic variants that predict responsiveness, potentially enabling personalized treatment selection.
Combination Synergies: While empirical evidence supports certain peptide combinations, the mechanisms of synergy remain poorly understood. Pharmacokinetic and pharmacodynamic studies are needed to optimize multi-peptide protocols.
Biomarker Development: Current monitoring relies on testosterone and LH levels, but these may not capture the full therapeutic picture. Researchers are validating novel biomarkers like Kiss1 receptor expression, GH pulse amplitude, and metabolomic profiles.
💡 Research Pipeline: Over 30 peptide compounds targeting testosterone optimization are in various stages of development, from preclinical studies to Phase III trials.
Key Takeaways: Evidence-Based Testosterone Optimization
• Peptides offer a physiologic approach to testosterone optimization by stimulating natural production rather than replacing it, preserving fertility and testicular function while achieving clinically meaningful hormone increases.
• Kisspeptin-10 provides the most targeted HPG axis stimulation, with studies showing 250-400 ng/dL testosterone increases through direct Kiss1 receptor activation and sustained GnRH release patterns.
• CJC-1295 plus ipamorelin creates the most popular combination, leveraging growth hormone pathways to increase testosterone through improved sleep architecture, enhanced Leydig cell sensitivity, and reduced inflammatory cytokines.
• Pulsatile delivery patterns matter critically — continuous gonadorelin infusion causes receptor desensitization within 8 weeks, while 90-minute pulsatile protocols maintain effectiveness throughout 12-24 week cycles.
• Dosing requires individualization based on baseline testosterone, age, body weight, and treatment goals, with beginner protocols starting at 0.3 mcg/kg kisspeptin or 100 mcg ipamorelin and advancing based on response and tolerance.
• Safety profiles favor peptides over traditional TRT in men seeking fertility preservation, with studies showing maintained or improved sperm parameters alongside testosterone normalization in 85% of users.
• Monitoring protocols must include both efficacy and safety markers, with testosterone, LH, prolactin (for hexarelin users), and PSA representing essential tracking parameters throughout treatment cycles.
• Cost considerations range from $200-400 monthly for research-grade peptides, positioning them between expensive TRT gels and generic testosterone injections, but with unique benefits justifying the premium.
• Legal status remains complex, with most testosterone-boosting peptides classified as research chemicals rather than approved medications, requiring careful sourcing and medical supervision.
• Future developments promise improved convenience through oral formulations, extended-release preparations, and smart delivery systems that could revolutionize peptide therapy accessibility and effectiveness.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Related Articles on BuyPeptidesOnline.com
CJC-1295 Complete Guide: Dosing, Benefits & Vendor Comparison
Ipamorelin vs GHRP-6: Growth Hormone Peptide Comparison
Best Peptides for Men Over 40: Anti-Aging Protocol Guide
HCG vs Peptides for Testosterone: Complete Comparison
Peptide Stacking Guide: Combinations That Work