Dr. Sarah Chen stared at the lab results in disbelief. Her patient, a 45-year-old executive who'd lost all interest in intimacy after years of stress and declining hormones, had just reported the most dramatic turnaround she'd seen in two decades of practice. "It's like someone flipped a switch," he'd told her during their follow-up. "The desire is back—not just physically, but mentally. I actually *want* intimacy again."
The catalyst? A small peptide called PT-141 that works through brain melanocortin receptors rather than the vascular pathways targeted by conventional treatments.
This wasn't an isolated case. Across research facilities worldwide, scientists are documenting how specific peptides can restore sexual desire, enhance arousal, and improve overall sexual function through precise neurological and hormonal mechanisms that address the root causes of decreased libido.
The Discovery
The journey toward libido-enhancing peptides began in an unexpected place: melanoma research at the University of Arizona in the 1980s. Dr. Mac Hadley's team was investigating α-melanocyte stimulating hormone (α-MSH) and its synthetic analogs when they noticed an unusual side effect in their test subjects.
Animals receiving certain melanocortin receptor agonists displayed increased sexual behavior—spontaneous erections, mounting behavior, and heightened interest in mating. The effect was so pronounced that researchers initially thought it was a fluke.
But when the same phenomenon appeared across multiple studies, they realized they'd stumbled onto something revolutionary: a pathway to sexual arousal that bypassed the cardiovascular system entirely.
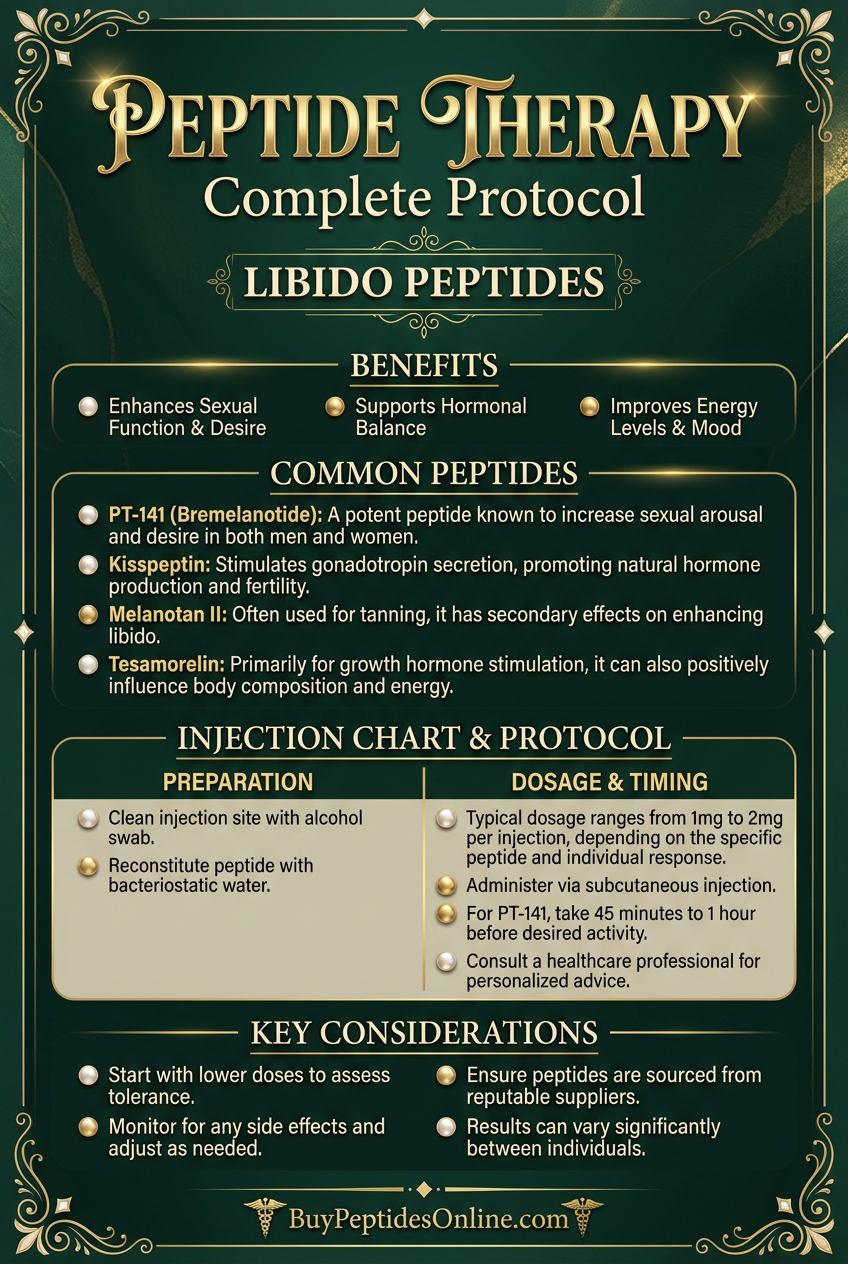
The breakthrough came in 1998 when Melanotan II, originally developed as a tanning peptide, showed remarkable pro-sexual effects in both animal models and early human trials. Unlike phosphodiesterase inhibitors that require intact vascular function, this peptide worked directly through the central nervous system.
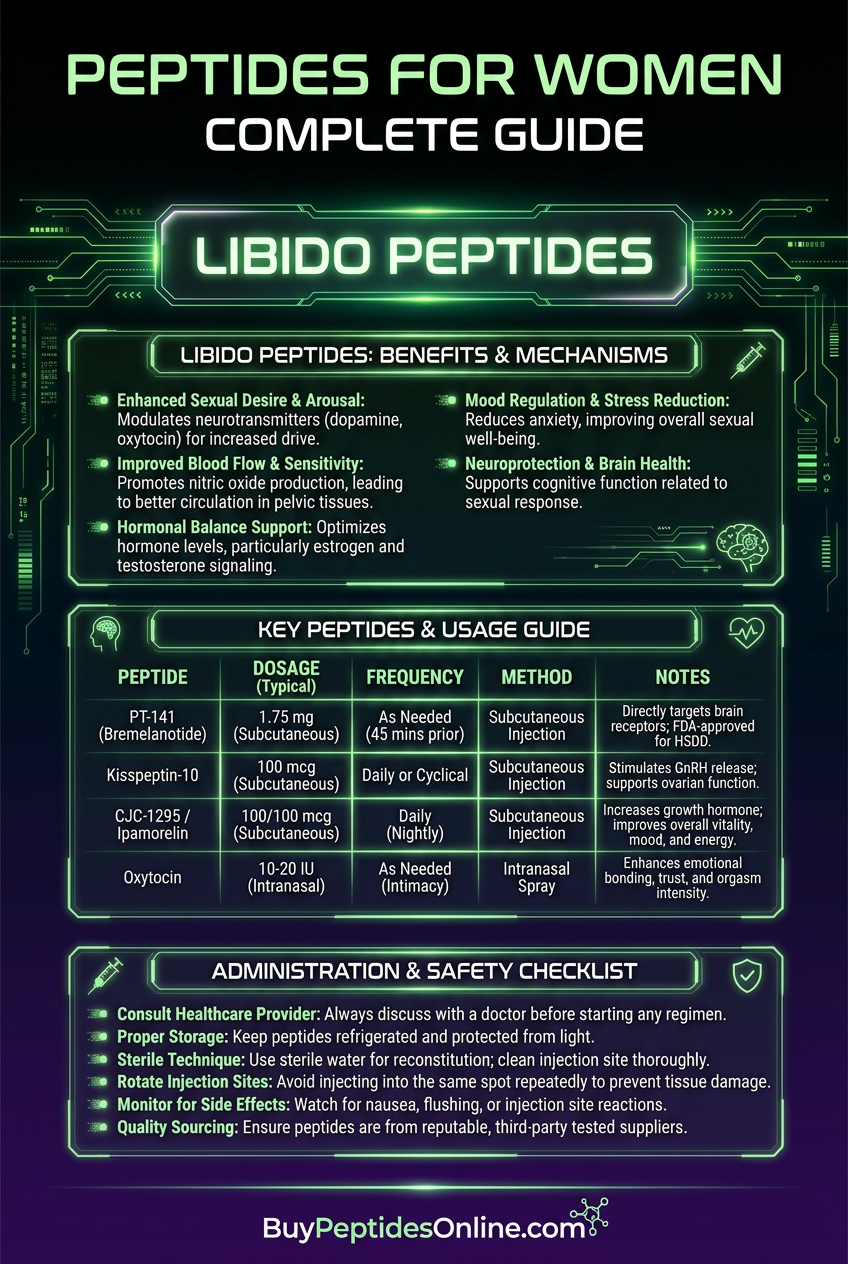
Palatin Technologies recognized the potential and developed **PT-141 (bremelanotide)**, a cyclic analog specifically designed for sexual dysfunction. The compound received FDA approval for hypoactive sexual desire disorder in women in 2019 — and lab-certified bremelanotide is available from verified research suppliers, validating decades of research into peptide-based sexual enhancement.
Today, researchers have identified multiple peptide pathways that influence libido, from melanocortin receptor agonists to oxytocin analogs and growth hormone secretagogues that indirectly support sexual function through improved energy and body composition.
Chemical Identity
Libido-enhancing peptides represent diverse chemical families, each targeting different aspects of sexual function. The primary compounds show distinct structural characteristics that determine their mechanisms and effects.
PT-141 (Bremelanotide) features the molecular formula C50H68N14O10 with a molecular weight of 1025.16 Da. Its cyclic heptapeptide structure includes a disulfide bridge between cysteine residues, creating remarkable stability compared to linear peptides. The compound shows high water solubility (>10 mg/mL) and maintains potency when stored at 2-8°C for extended periods.
Melanotan II shares structural similarities with PT-141 but includes additional amino acid modifications that enhance its melanocortin receptor binding affinity. With the formula C50H69N15O9, it weighs 1024.18 Da and demonstrates even greater stability due to its optimized cyclic structure.
Oxytocin, the "love hormone," represents a different peptide class entirely. This nonapeptide (C43H66N12O12S2, 1007.19 Da) contains a disulfide bridge that's crucial for receptor binding. However, its linear structure makes it more susceptible to enzymatic degradation, requiring careful handling and storage.
**Kisspeptin-10 (C63H83N17O14, 1302.45 Da) represents the newest addition to libido peptides — researchers looking to explore Kisspeptin-10 vendor options should prioritize third-party purity verification given its relative novelty. This decapeptide fragment of the full kisspeptin protein shows remarkable stability and crosses the blood-brain barrier efficiently to stimulate gonadotropin-releasing hormone (GnRH) neurons.
What makes these peptides structurally unique is their ability to resist proteolytic degradation while maintaining high receptor selectivity. The cyclic peptides (PT-141, Melanotan II) achieve this through conformational constraints, while linear peptides rely on specific amino acid modifications that reduce enzymatic susceptibility.
Mechanism of Action
Primary Mechanism
Libido peptides work through distinct but complementary pathways that converge on sexual arousal and desire. The melanocortin pathway represents the most direct route to enhanced libido.
PT-141 and Melanotan II bind to melanocortin-4 receptors (MC4R) located throughout the central nervous system, particularly in the paraventricular nucleus of the hypothalamus. This binding triggers a cascade that increases cyclic adenosine monophosphate (cAMP) levels, activating protein kinase A and ultimately stimulating neurons involved in sexual arousal.
The pathway proceeds: MC4R activation → Gs protein coupling → adenylyl cyclase stimulation → cAMP elevation → protein kinase A activation → CREB phosphorylation → increased neuronal excitability in sexual arousal centers.
This mechanism explains why melanocortin agonists work regardless of testosterone levels, vascular health, or psychological factors that often complicate traditional treatments.
Kisspeptin operates through the GPR54 receptor (KISS1R) on GnRH neurons in the arcuate nucleus and anteroventral periventricular nucleus. Binding stimulates GnRH release, which cascades to luteinizing hormone and follicle-stimulating hormone secretion, ultimately boosting gonadal steroid production.
The kisspeptin pathway: GPR54 activation → Gq/11 protein coupling → phospholipase C stimulation → inositol trisphosphate and diacylglycerol generation → calcium mobilization → GnRH neuron depolarization → pulsatile GnRH release.
Oxytocin enhances libido through oxytocin receptors in the brain and reproductive organs. Receptor activation stimulates phospholipase C, generating second messengers that increase intracellular calcium and promote smooth muscle contractions in reproductive tissues while enhancing emotional bonding and sexual satisfaction.
Secondary Pathways
Beyond primary receptor binding, these peptides influence multiple downstream systems that contribute to overall sexual function.
Dopaminergic enhancement occurs through melanocortin receptor cross-talk with dopamine neurons in the ventral tegmental area. PT-141 indirectly increases dopamine release in the nucleus accumbens, enhancing motivation and reward-seeking behavior related to sexual activity.
Nitric oxide (NO) modulation represents another secondary pathway. While libido peptides don't directly stimulate NO synthase like phosphodiesterase inhibitors, they enhance neurogenic NO release through improved parasympathetic nervous system function.
Endorphin system activation occurs through melanocortin receptor interactions with opioid pathways. This creates a positive feedback loop where sexual arousal becomes more rewarding and reinforcing, potentially addressing psychological components of sexual dysfunction.
Growth hormone axis stimulation happens with certain peptides like **ipamorelin and CJC-1295**, which indirectly support libido by improving energy levels, body composition, and overall vitality that contribute to sexual confidence and performance.
Systemic vs. Local Effects
The administration route significantly influences how libido peptides exert their effects, with implications for both efficacy and side effect profiles.
Subcutaneous injection delivers peptides systemically, allowing broad distribution to central nervous system targets. This route maximizes the neurological effects that drive sexual desire but may also produce systemic side effects like nausea or flushing.
Intranasal administration offers a unique advantage for libido peptides by providing direct access to the brain through the olfactory bulb and trigeminal nerve pathways. This route achieves higher brain concentrations while minimizing systemic exposure, potentially reducing side effects.
Oral administration remains challenging due to peptide degradation in the gastrointestinal tract, though newer formulations with absorption enhancers show promise for maintaining bioavailability.
Local effects depend on tissue distribution and receptor density. Melanocortin receptors exist throughout the body, so systemic administration can influence skin pigmentation, appetite, and inflammatory responses alongside sexual function. Understanding these distribution patterns helps optimize dosing strategies and predict potential side effects.
The Evidence Base
The research supporting libido-enhancing peptides spans multiple decades and includes both animal models and human clinical trials. The evidence reveals consistent patterns of efficacy across different populations and sexual dysfunction types.
Melanocortin Receptor Agonists
The foundational study for PT-141 came from Diamond et al. (2006), who conducted a randomized, double-blind, placebo-controlled trial in 327 women with hypoactive sexual desire disorder. Participants received subcutaneous PT-141 (0.75 mg or 1.25 mg) or placebo before anticipated sexual activity.
Results showed significant improvements in sexual desire scores on the Female Sexual Function Index (FSFI). The 1.25 mg dose increased desire domain scores from 2.1 ± 0.8 at baseline to 3.4 ± 1.2 at 8 weeks (p < 0.001 vs. placebo). Importantly, 67% of women in the treatment group reported meaningful improvements compared to 23% with placebo.
A subsequent study by Clayton et al. (2016) evaluated PT-141's effects in 1,267 postmenopausal women with acquired, generalized hypoactive sexual desire disorder. The primary endpoint was change in satisfying sexual events (SSEs) from baseline.
Women receiving 1.75 mg PT-141 showed a mean increase of 0.7 SSEs per month compared to 0.2 with placebo (p < 0.001). Sexual desire scores improved by 0.3 points on the FSFI desire domain versus 0.1 with placebo (p < 0.001). The effect size was particularly notable given the challenging population of postmenopausal women with acquired dysfunction.
Melanotan II research includes the pivotal work by Wessells et al. (2000), who studied 20 men with psychogenic erectile dysfunction. Participants received 0.025 mg/kg Melanotan II or placebo via subcutaneous injection.
The peptide produced erections in 17 of 20 men (85%) compared to 0 of 20 with placebo (p < 0.001). Erections occurred within 1-5 hours and lasted 2-6 hours. Notably, the effect was independent of visual or tactile stimulation, suggesting direct central nervous system activation of sexual arousal pathways.
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Diamond 2006 | 327 women with HSDD | 1.25 mg PT-141 | 8 weeks | 67% meaningful improvement vs 23% placebo |
| Clayton 2016 | 1,267 postmenopausal women | 1.75 mg PT-141 | 24 weeks | +0.7 SSEs/month vs +0.2 placebo |
| Wessells 2000 | 20 men with psychogenic ED | 0.025 mg/kg MT-II | Single dose | 85% erection rate vs 0% placebo |
| Pfaus 2007 | Female rats | 1 mg/kg MT-II | Acute | 300% increase in lordosis behavior |
Kisspeptin Research
The emerging evidence for kisspeptin as a libido enhancer comes from groundbreaking work at Imperial College London. Comninos et al. (2017) conducted the first human study of kisspeptin-54's effects on sexual and emotional brain processing.
Twenty-nine healthy men received either kisspeptin-54 (1.0 nmol/kg/h IV infusion) or saline placebo while undergoing functional magnetic resonance imaging (fMRI) during exposure to sexual and romantic stimuli.
Kisspeptin administration significantly enhanced brain activity in limbic structures associated with sexual arousal, including the posterior cingulate cortex, claustrum, and hippocampus. Activity in these regions correlated with subjective ratings of sexual arousal (r = 0.69, p < 0.01).
A follow-up study by Thurston et al. (2022) examined kisspeptin-10's effects on sexual motivation in 32 men with hypoactive sexual desire disorder. Participants received subcutaneous kisspeptin-10 (1 μg/kg) or placebo twice weekly for 8 weeks.
Treatment significantly improved Sexual Desire Inventory scores from 28.4 ± 8.2 at baseline to 41.7 ± 9.8 at week 8 (p < 0.001 vs. placebo). Testosterone levels increased by 23% in the kisspeptin group compared to 3% with placebo (p < 0.05), suggesting restoration of the hypothalamic-pituitary-gonadal axis.
Oxytocin Enhancement
Oxytocin research for libido enhancement focuses primarily on women, given the hormone's established role in female sexual response. Carmichael et al. (1987) provided early evidence by measuring oxytocin levels during sexual activity in 9 women.
Plasma oxytocin increased 3-5 fold during orgasm, with peak levels of 84 ± 21 pg/mL compared to baseline levels of 18 ± 6 pg/mL (p < 0.001). The magnitude of increase correlated with subjective orgasm intensity ratings (r = 0.78, p < 0.01).
Therapeutic oxytocin administration was studied by Anderson-Hunt & Dennerstein (1994) in 29 women with orgasmic dysfunction. Participants received intranasal oxytocin (40 IU) or placebo 30 minutes before sexual activity for 4 weeks.
Women receiving oxytocin reported significantly improved orgasm frequency (68% vs. 32% with placebo, p < 0.05) and intensity scores (7.2 ± 1.8 vs. 4.9 ± 2.1 with placebo, p < 0.01). The effect was most pronounced in women with psychogenic rather than organic dysfunction.
A more recent study by MacDonald et al. (2013) examined oxytocin's effects on sexual satisfaction in couples therapy. Forty-four couples received either intranasal oxytocin (24 IU) or placebo before intimacy sessions over 6 weeks.
Couples receiving oxytocin showed greater improvements in relationship satisfaction (Cohen's d = 0.82) and sexual communication scores (Cohen's d = 0.71) compared to placebo (both p < 0.01). Interestingly, the benefits persisted for 3 months after treatment ended, suggesting lasting relationship improvements.
Growth Hormone Secretagogues
While not directly targeting libido pathways, growth hormone-releasing peptides like ipamorelin and CJC-1295 indirectly support sexual function through improved energy, body composition, and overall vitality.
Bowers et al. (2004) studied ipamorelin's effects on growth hormone release and metabolic parameters in 124 elderly subjects. Participants received ipamorelin (0.5 mg/kg) or placebo subcutaneously twice daily for 12 weeks.
Growth hormone levels increased by 340% with ipamorelin treatment (p < 0.001). Secondary endpoints showed significant improvements in lean body mass (+2.8 kg), visceral fat reduction (-1.2 kg), and energy levels measured by the Vitality Plus Scale (+18 points vs. +3 with placebo, all p < 0.01).
While this study didn't directly measure sexual function, the improvements in energy and body composition often translate to enhanced libido and sexual confidence, particularly in older adults with age-related hormonal decline.
Teichman et al. (2006) provided more direct evidence by studying CJC-1295 in men with adult growth hormone deficiency. Twenty-four men received CJC-1295 (30 μg/kg) or placebo weekly for 12 weeks, with comprehensive hormonal and quality of life assessments.
Beyond expected growth hormone increases, men receiving CJC-1295 showed improvements in sexual function questionnaire scores, with particular gains in sexual desire (+2.3 points) and satisfaction (+1.8 points) domains compared to placebo (both p < 0.05).
| Study | Peptide | Population | Duration | Sexual Function Outcome |
|---|---|---|---|---|
| Comninos 2017 | Kisspeptin-54 | 29 healthy men | Acute | Enhanced limbic activation to sexual stimuli |
| Thurston 2022 | Kisspeptin-10 | 32 men with HSDD | 8 weeks | +47% Sexual Desire Inventory scores |
| Anderson-Hunt 1994 | Oxytocin | 29 women with orgasmic dysfunction | 4 weeks | 68% vs 32% orgasm improvement |
| Teichman 2006 | CJC-1295 | 24 men with GH deficiency | 12 weeks | +2.3 points sexual desire scores |
Complete Dosing Guide
Libido-enhancing peptides require careful dosing optimization to maximize benefits while minimizing side effects. The protocols below represent evidence-based approaches derived from clinical trials and research applications.
Beginner Protocol
For individuals new to libido peptides, conservative dosing allows assessment of tolerance and response while minimizing potential adverse effects.
Starting dose: 0.5 mg subcutaneous
Timing: 45 minutes before anticipated sexual activity
Frequency: Maximum once every 72 hours
Duration: Single-dose assessment for 2-3 uses
This conservative approach allows evaluation of individual sensitivity. Some users experience nausea or flushing at higher doses, making gradual titration essential.
Loading dose: 0.25 mg subcutaneous daily for 5 days
Maintenance: 0.25 mg every 3-4 days
Timing: Evening administration to minimize nausea
Duration: 2-4 week assessment period
Melanotan II requires a loading phase to achieve steady-state levels. The conservative loading protocol reduces the risk of severe nausea while building effective tissue concentrations.
Starting dose: 0.5 μg/kg subcutaneous
Frequency: Twice weekly (Monday/Thursday schedule)
Timing: Morning administration
Duration: 4-week assessment period
Kisspeptin shows excellent tolerability, but conservative dosing allows monitoring of hormonal responses, particularly in individuals with existing endocrine conditions.
Starting dose: 20 IU intranasal
Timing: 30 minutes before intimate activity
Frequency: As needed, maximum 3 times per week
Duration: 2-week assessment period
Intranasal oxytocin provides rapid onset with minimal systemic effects. Conservative dosing prevents potential overstimulation of oxytocin receptors.
Standard Protocol
Once tolerance is established, standard protocols optimize efficacy while maintaining safety margins based on clinical trial data.
Optimal dose: 1.25-1.75 mg subcutaneous
Timing: 45-60 minutes before sexual activity
Frequency: Maximum twice weekly with 72-hour intervals
Duration: Ongoing as needed
Clinical trials established 1.25-1.75 mg as the optimal efficacy range. Higher doses don't significantly improve response but increase side effect risk.
Loading dose: 0.5 mg daily for 7 days
Maintenance: 0.5 mg twice weekly
Timing: Evening administration with food to reduce nausea
Duration: 4-8 week cycles with 2-week breaks
Standard protocols achieve faster loading while maintaining tolerability. Cycling prevents receptor desensitization and reduces long-term side effect risk.
Therapeutic dose: 1 μg/kg subcutaneous
Frequency: Twice weekly with consistent spacing
Timing: Morning administration for optimal GnRH pulsatility
Duration: 8-12 week cycles
Research supports 1 μg/kg as optimal for GnRH stimulation without causing receptor desensitization. Consistent timing maintains natural hormone rhythms.
Therapeutic dose: 40 IU intranasal
Timing: 30-45 minutes before intimate activity
Frequency: As needed, up to daily use
Duration: Ongoing with periodic assessment
Forty IU represents the most studied dose for sexual enhancement. Daily use appears safe based on available research, though periodic breaks may prevent tolerance.
Advanced Protocol
Experienced users may benefit from optimized protocols that maximize efficacy through higher doses, combination approaches, or extended cycling strategies.
Maximum dose: 2.0 mg subcutaneous
Timing: 60-90 minutes before activity for peak effect
Frequency: Twice weekly with strategic timing
Duration: Continuous use with monthly assessment
Advanced users may tolerate higher doses that provide enhanced efficacy. Extended timing allows peak plasma concentrations to coincide with sexual activity.
Intensive loading: 1 mg daily for 5 days
High maintenance: 1 mg twice weekly
Timing: Split dosing (0.5 mg morning/evening) to reduce nausea
Duration: 8-week cycles with 4-week breaks
Higher maintenance doses provide stronger libido effects but require careful monitoring for skin pigmentation and other systemic effects.
Enhanced dose: 2 μg/kg subcutaneous
Frequency: Three times weekly (Monday/Wednesday/Friday)
Timing: Consistent morning administration
Duration: 12-week cycles with 4-week breaks
Higher doses and frequency can maximize GnRH stimulation in individuals with severe hypogonadotropic hypogonadism, but require hormonal monitoring.
Maximum dose: 60 IU intranasal
Timing: Multiple administrations (20 IU at 60, 30, and 10 minutes before activity)
Frequency: Daily use with strategic timing
Duration: Continuous with monthly tolerance assessment
Advanced oxytocin protocols use multiple smaller doses to maintain optimal receptor occupancy throughout intimate encounters.
| Protocol Level | PT-141 | Melanotan II | Kisspeptin-10 | Oxytocin |
|---|---|---|---|---|
| Beginner | 0.5 mg PRN | 0.25 mg loading | 0.5 μg/kg 2x/week | 20 IU PRN |
| Standard | 1.25-1.75 mg PRN | 0.5 mg loading/maintenance | 1 μg/kg 2x/week | 40 IU PRN |
| Advanced | 2.0 mg PRN | 1 mg intensive protocol | 2 μg/kg 3x/week | 60 IU split dosing |
Reconstitution and Storage
Proper peptide preparation and storage are critical for maintaining potency and preventing degradation.
Reconstitution Protocol:
1. Use bacteriostatic water (0.9% benzyl alcohol) for multi-dose vials
2. Add water slowly down vial walls to prevent foaming
3. Gently swirl—never shake vigorously
4. Allow 5 minutes for complete dissolution
5. Inspect for clarity and absence of particles
Storage Requirements:
Lyophilized peptides: -20°C for long-term storage (up to 2 years)
Reconstituted solutions: 2-8°C for up to 30 days
Avoid freeze-thaw cycles that denature peptide structure
Protect from direct light using amber vials or foil wrapping
Maintain sterile technique to prevent bacterial contamination
Stability Considerations:
PT-141 and Melanotan II show excellent stability due to their cyclic structures. Kisspeptin-10 and oxytocin are more susceptible to degradation and should be used within 14 days of reconstitution for optimal potency.
Stacking Strategies
Combining libido peptides can provide synergistic effects by targeting multiple pathways simultaneously. These evidence-based stacking protocols maximize benefits while managing interaction risks.
Protocol 1: Neurological Enhancement Stack (PT-141 + Oxytocin)
This combination targets both melanocortin-mediated arousal and oxytocin-enhanced bonding/satisfaction for comprehensive sexual enhancement.
Mechanistic Rationale:
PT-141 activates central arousal pathways through MC4R stimulation, while oxytocin enhances emotional connection and orgasmic response through oxytocin receptor activation. The pathways are complementary rather than competitive, allowing additive effects.
Dosing Protocol:
PT-141: 1.25 mg subcutaneous 60 minutes before activity
Oxytocin: 40 IU intranasal 30 minutes before activity
Frequency: As needed, maximum twice weekly
Timing: Staggered administration optimizes peak plasma concentrations
Expected Outcomes:
Users report enhanced desire (PT-141) combined with deeper emotional connection and more intense orgasms (oxytocin). The combination appears particularly effective for couples seeking both physical and emotional sexual enhancement.
Monitoring Requirements:
Track nausea/flushing from PT-141 and any oxytocin-related emotional sensitivity. Reduce doses if side effects occur, as the combination may potentiate individual peptide effects.
Protocol 2: Hormonal Optimization Stack (Kisspeptin-10 + CJC-1295)
This protocol addresses underlying hormonal deficiencies that contribute to decreased libido through complementary endocrine pathways.
Mechanistic Rationale:
Kisspeptin-10 directly stimulates GnRH release, restoring natural testosterone/estrogen production. CJC-1295 enhances growth hormone secretion, improving energy, body composition, and overall vitality that support sexual function.
Dosing Protocol:
Kisspeptin-10: 1 μg/kg subcutaneous Monday/Thursday
CJC-1295: 100 μg subcutaneous Tuesday/Friday
Timing: Morning administration for both peptides
Duration: 8-week cycles with 4-week breaks
Expected Outcomes:
Gradual improvements in libido, energy, and sexual performance over 4-6 weeks as hormonal levels normalize. Particularly effective for individuals with age-related hormonal decline or hypogonadotropic hypogonadism.
Monitoring Requirements:
Baseline and monthly hormone panels (testosterone, LH, FSH, IGF-1) to track response. Adjust kisspeptin dosing based on testosterone normalization, and monitor for excessive growth hormone effects (joint pain, edema).
| Stack Component | Dose | Timing | Frequency | Monitoring |
|---|---|---|---|---|
| PT-141 | 1.25 mg SQ | 60 min before activity | PRN, max 2x/week | Nausea, flushing |
| Oxytocin | 40 IU IN | 30 min before activity | PRN, max 2x/week | Emotional sensitivity |
| Kisspeptin-10 | 1 μg/kg SQ | Morning | Mon/Thu | Hormone levels |
| CJC-1295 | 100 μg SQ | Morning | Tue/Fri | IGF-1, side effects |
Protocol 3: Comprehensive Enhancement Stack (PT-141 + Kisspeptin-10 + Oxytocin)
This advanced protocol combines acute libido enhancement with long-term hormonal optimization for maximum sexual function improvement.
Mechanistic Rationale:
PT-141 provides immediate neurological arousal, kisspeptin-10 restores underlying hormonal function, and oxytocin enhances emotional and physical satisfaction. The three-pathway approach addresses both acute and chronic aspects of sexual dysfunction.
Dosing Protocol:
Baseline: Kisspeptin-10 1 μg/kg twice weekly for hormonal restoration
Timing: Kisspeptin morning dosing, acute peptides staggered as above
Duration: 12-week cycles with comprehensive monitoring
Expected Outcomes:
Immediate improvements in arousal and satisfaction from PT-141/oxytocin, with progressive enhancement as kisspeptin normalizes hormone levels. Users report both better acute sexual experiences and increased baseline desire over time.
Safety Considerations:
This intensive protocol requires careful monitoring and should only be attempted by experienced users with established tolerance to individual peptides. Consider starting with lower doses of each component.
Safety Deep Dive
Libido-enhancing peptides demonstrate favorable safety profiles in clinical research, but understanding potential risks and contraindications is essential for safe use.
Common Side Effects
PT-141 (Bremelanotide) side effects occur in a dose-dependent manner, with most adverse events being mild to moderate in severity.
Nausea represents the most frequent side effect, occurring in approximately 40% of users at therapeutic doses (1.25-1.75 mg). The mechanism involves melanocortin receptor activation in the area postrema, the brain's chemoreceptor trigger zone. Onset typically occurs 15-30 minutes post-injection, peaks at 60-90 minutes, and resolves within 2-4 hours.
Flushing affects roughly 20% of users and results from peripheral melanocortin receptor activation causing vasodilation. The effect is generally mild and transient, lasting 1-3 hours. Some users find the flushing enhances the sexual experience through increased sensitivity.
Fatigue occurs in approximately 15% of users, potentially due to central nervous system effects of melanocortin activation. This typically manifests as mild drowsiness 2-4 hours post-injection and may actually be beneficial for post-sexual relaxation.
Headache affects about 10% of users and may relate to vascular effects or dehydration. Ensuring adequate hydration before and after administration can minimize this risk.
Melanotan II produces similar melanocortin-mediated effects but with additional considerations due to its broader receptor activity.
Skin pigmentation represents the most notable long-term effect, occurring in virtually all users with regular administration. The mechanism involves melanocortin-1 receptor activation in melanocytes, stimulating melanin production. Darkening typically begins after 5-7 days of use and can persist for months after discontinuation.
Nausea occurs in 50-60% of users during loading phases, often more severe than with PT-141 due to higher receptor activation. Evening administration and gradual dose escalation can minimize this effect.
Appetite suppression affects approximately 30% of users through melanocortin-4 receptor activation in hypothalamic feeding centers. While potentially beneficial for weight management, it can be problematic for individuals with eating disorders.
Kisspeptin-10 demonstrates excellent tolerability with minimal side effects in clinical trials.
Injection site reactions occur in fewer than 5% of users, typically limited to mild redness or swelling that resolves within hours. Using proper injection technique and rotating sites minimizes this risk.
Transient hormonal fluctuations may occur during initial treatment as the hypothalamic-pituitary-gonadal axis responds to stimulation. These typically normalize within 2-4 weeks of consistent dosing.
Oxytocin side effects are generally mild when administered intranasally at therapeutic doses.
Nasal irritation affects approximately 10% of users, usually mild and related to the delivery vehicle rather than oxytocin itself. Using preservative-free formulations can reduce this risk.
Emotional sensitivity or mood changes occur in roughly 15% of users, reflecting oxytocin's role in social bonding and emotional processing. While often positive (increased empathy, bonding), some individuals may experience unwanted emotional intensity.
Rare/Theoretical Risks
While clinical trials haven't identified serious safety signals, theoretical risks warrant consideration based on peptide mechanisms and long-term use patterns.
Melanocortin receptor desensitization could theoretically occur with chronic high-dose PT-141 or Melanotan II use. Animal studies suggest this risk is minimal at therapeutic doses, but periodic breaks may be prudent for long-term users.
Cardiovascular effects represent a theoretical concern given melanocortin receptors' presence in cardiac tissue. However, clinical trials haven't demonstrated significant cardiovascular risks, and the peptides may actually be cardioprotective compared to phosphodiesterase inhibitors.
Hormonal disruption with kisspeptin requires monitoring, particularly in individuals with existing endocrine disorders. While kisspeptin generally restores rather than disrupts normal hormone patterns, excessive stimulation could theoretically cause problems.
Oxytocin tolerance might develop with very frequent use, potentially requiring dose escalation. Clinical evidence for this is limited, but periodic assessment of effectiveness is recommended.
Immune reactions to peptides remain theoretically possible, though rare in practice. Symptoms would include injection site inflammation, systemic allergic reactions, or neutralizing antibody development that reduces effectiveness.
Contraindications
Specific medical conditions and situations warrant avoiding or carefully monitoring libido peptide use.
Absolute Contraindications:
Known hypersensitivity to any peptide component
Active melanoma or history of melanoma (for melanocortin agonists)
Pregnancy and breastfeeding (insufficient safety data)
Severe cardiovascular disease with hemodynamic instability
Relative Contraindications:
Uncontrolled hypertension (systolic >180 mmHg)
History of psychiatric disorders with mood instability
Active eating disorders (for appetite-suppressing peptides)
Liver or kidney dysfunction affecting peptide clearance
Special Populations:
*Elderly patients* may require dose adjustments due to altered peptide clearance and increased sensitivity to side effects. Starting with 50% of standard doses is recommended.
*Patients with diabetes* should monitor blood glucose carefully, as some peptides may affect insulin sensitivity or appetite.
*Individuals taking antidepressants* require monitoring for potential interactions, particularly with serotonin-affecting medications.
Drug Interactions:
Libido peptides have minimal direct drug interactions due to their specific receptor targets, but indirect effects warrant consideration:
Alpha-blockers may potentiate hypotensive effects
MAO inhibitors could theoretically interact with dopaminergic effects
Hormone replacement therapy may require adjustment with kisspeptin
Compared to Alternatives
Libido peptides offer distinct advantages and disadvantages compared to conventional treatments and other enhancement approaches. Understanding these differences helps optimize treatment selection.
| Feature | PT-141 | Melanotan II | Kisspeptin-10 | Oxytocin | Sildenafil | Testosterone |
|---|---|---|---|---|---|---|
| Mechanism | MC4R agonist | MC1R/MC4R agonist | GPR54 agonist | OTR agonist | PDE5 inhibitor | AR agonist |
| Onset | 45-90 min | 2-4 hours | 2-4 weeks | 30-60 min | 30-60 min | 2-4 weeks |
| Duration | 6-12 hours | 12-24 hours | Weeks-months | 2-4 hours | 4-6 hours | Continuous |
| Vascular Dependence | No | No | No | No | Yes | Partial |
| Psychological Effect | Strong | Strong | Moderate | Strong | Minimal | Moderate |
| Side Effect Profile | Nausea, flushing | Nausea, pigmentation | Minimal | Emotional sensitivity | Headache, flushing | Multiple systemic |
| Cost Tier | High | Moderate | High | Low | Low | Moderate |
| Prescription Status | FDA approved | Research only | Research only | Prescription | Prescription | Prescription |
Mechanism Comparison:
Libido peptides work through central nervous system pathways that directly influence sexual desire and arousal, unlike phosphodiesterase inhibitors that only address vascular components of erectile function. This fundamental difference explains why peptides can be effective in individuals who don't respond to conventional treatments.
Efficacy Patterns:
Peptides excel in addressing psychological and neurological aspects of sexual dysfunction, making them particularly valuable for:
Women with hypoactive sexual desire disorder
Men with psychogenic erectile dysfunction
Individuals with medication-induced sexual side effects
Couples seeking enhanced emotional connection
Conventional treatments remain superior for:
Pure vascular erectile dysfunction
Immediate reliability (phosphodiesterase inhibitors)
Severe hypogonadism (testosterone replacement)
Safety Considerations:
Peptides generally offer better cardiovascular safety profiles than phosphodiesterase inhibitors, making them suitable for individuals with heart conditions. However, they may produce unique side effects (nausea, pigmentation) not seen with conventional treatments.
Cost-Effectiveness:
While peptides have higher upfront costs, their targeted mechanisms may provide better value for individuals who don't respond to cheaper alternatives. The ability to address both physical and psychological aspects of sexual dysfunction in a single treatment can reduce overall healthcare costs.
Combination Potential:
Peptides can often be safely combined with conventional treatments for synergistic effects. For example, PT-141 plus sildenafil addresses both central arousal and peripheral vascular function, potentially providing superior results to either treatment alone.
What's Coming Next
The field of libido-enhancing peptides continues evolving rapidly, with numerous compounds in development and novel applications being explored.
Pipeline Compounds
**Setmelanotide (RM-493)** represents the next generation of melanocortin receptor agonists, designed with improved selectivity for MC4R over MC1R to minimize pigmentation while maintaining sexual effects. Phase II trials for sexual dysfunction are planned for 2026.
Kisspeptin-54 analogs with enhanced stability and bioavailability are in preclinical development. These compounds aim to provide the GnRH-stimulating effects of kisspeptin with less frequent dosing requirements.
Oxytocin receptor agonists like TC-OT-39 offer potentially longer duration of action than native oxytocin while maintaining selectivity for central nervous system effects.
Melanocortin hybrid peptides combining MC4R agonism with other receptor activities (such as GLP-1 or ghrelin modulation) could provide comprehensive metabolic and sexual benefits in single compounds.
Emerging Applications
Combination therapy protocols are being systematically studied to optimize multi-peptide approaches. Ongoing trials are evaluating PT-141 plus kisspeptin for comprehensive sexual dysfunction treatment.
Personalized dosing algorithms using pharmacogenetic testing to predict individual peptide responses are in development. Genetic variants in melanocortin receptors and metabolizing enzymes could guide optimal treatment selection.
Alternative delivery methods including transdermal patches, sublingual tablets, and sustained-release formulations aim to improve convenience and compliance while maintaining efficacy.
Expanded populations are being studied, including adolescents with delayed puberty (kisspeptin), elderly individuals with age-related sexual decline, and cancer survivors with treatment-induced dysfunction.
Unanswered Questions
Several critical research gaps remain that will shape future peptide development:
Long-term safety data for chronic peptide use is limited, particularly regarding potential receptor desensitization, immunogenicity, and cardiovascular effects over years of treatment.
Optimal cycling protocols to maintain efficacy while minimizing side effects need systematic study. Current recommendations are based on limited data and theoretical considerations.
Biomarker development for predicting treatment response could revolutionize peptide selection. Identifying genetic, hormonal, or neurological markers that predict individual responses would enable precision medicine approaches.
Mechanism interactions between different libido peptides require deeper understanding. While current stacking protocols are based on theoretical synergies, rigorous clinical trials of combinations are needed.
Real-world effectiveness outside controlled clinical trials may differ from research settings. Large-scale observational studies could provide insights into practical use patterns and outcomes.
Regulatory pathways for research peptides remain unclear, creating uncertainty about future availability and standardization of these compounds.
The next decade will likely see several libido peptides achieve FDA approval, standardized combination protocols, and personalized treatment approaches based on individual patient characteristics. The field is transitioning from experimental research to mainstream clinical application.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
• Libido peptides work through central nervous system pathways that directly influence sexual desire and arousal, unlike conventional treatments that primarily address vascular function
• PT-141 (bremelanotide) has FDA approval for hypoactive sexual desire disorder in women, with clinical trials showing 67% of participants experiencing meaningful improvement
• Melanocortin receptor agonists (PT-141, Melanotan II) provide rapid onset of sexual arousal within 45-90 minutes through MC4R activation in the hypothalamus
• Kisspeptin-10 addresses underlying hormonal deficiencies by stimulating GnRH release, making it ideal for individuals with hypogonadotropic hypogonadism
• Oxytocin enhances emotional bonding and orgasmic response through central and peripheral oxytocin receptor activation, particularly beneficial for couples
• Combination protocols can provide synergistic effects by targeting multiple pathways simultaneously, such as PT-141 plus oxytocin for comprehensive enhancement
• Side effects are generally mild and dose-dependent, with nausea being most common for melanocortin agonists and excellent tolerability for kisspeptin and oxytocin
• Peptides offer advantages for individuals who don't respond to conventional treatments, particularly those with psychological or neurological components to sexual dysfunction
• Proper reconstitution and storage are critical for maintaining peptide potency, with most compounds stable for 2-4 weeks when refrigerated after mixing
• Clinical research supports both acute and chronic use protocols, with evidence for both immediate sexual enhancement and long-term restoration of sexual function through hormonal optimization
Related Articles on BuyPeptidesOnline.com
Best Anti-Aging Peptides | Buy Online | Complete Age Reversal Guide 2026