Dr. James Pfaus watched the laboratory data with growing excitement. Female rats that had shown zero interest in mating were suddenly exhibiting robust sexual behavior within 30 minutes of receiving a single injection. The compound wasn't testosterone, wasn't dopamine, and wasn't targeting any of the usual suspects in sexual arousal pathways.
It was **PT-141**, a synthetic peptide that would revolutionize our understanding of sexual function by targeting the brain's melanocortin system rather than relying on vascular mechanisms like traditional treatments. What started as an accidental discovery during tanning peptide research had uncovered the first centrally-acting treatment for sexual dysfunction that worked equally well in both men and women.
The Discovery
The story of PT-141 begins in the 1960s with **Melanotan II research at the University of Arizona. Scientists led by Dr. Mac Hadley were investigating synthetic analogs of α-melanocyte-stimulating hormone (α-MSH)** for their tanning properties. The goal was simple: create a compound that could stimulate melanin production without UV exposure, potentially preventing skin cancer while maintaining cosmetic tanning benefits.
What they discovered changed everything. Test subjects receiving lab-certified Melanotan II reported an unexpected side effect: dramatic increases in sexual arousal and libido. Both men and women experienced spontaneous erections and enhanced sexual desire that lasted hours after injection. The tanning research had accidentally stumbled upon the brain's sexual arousal circuitry.
By the 1990s, researchers at Palatin Technologies, led by Dr. Carl Spana, began systematically studying this sexual enhancement effect. They discovered that specific amino acid modifications to the Melanotan II structure could eliminate the tanning effects while preserving and enhancing the sexual benefits. After testing dozens of analogs, they identified Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH - the compound that would become PT-141.
The name "PT-141" comes from Palatin Technologies' internal designation system. Early clinical trials in 1998 showed remarkable results: 72% of men with erectile dysfunction achieved erections suitable for intercourse, while 85% of women with hypoactive sexual desire disorder reported significant improvements in arousal and satisfaction. Unlike sildenafil (Viagra), which requires intact vascular function, PT-141 worked by directly activating sexual centers in the hypothalamus.
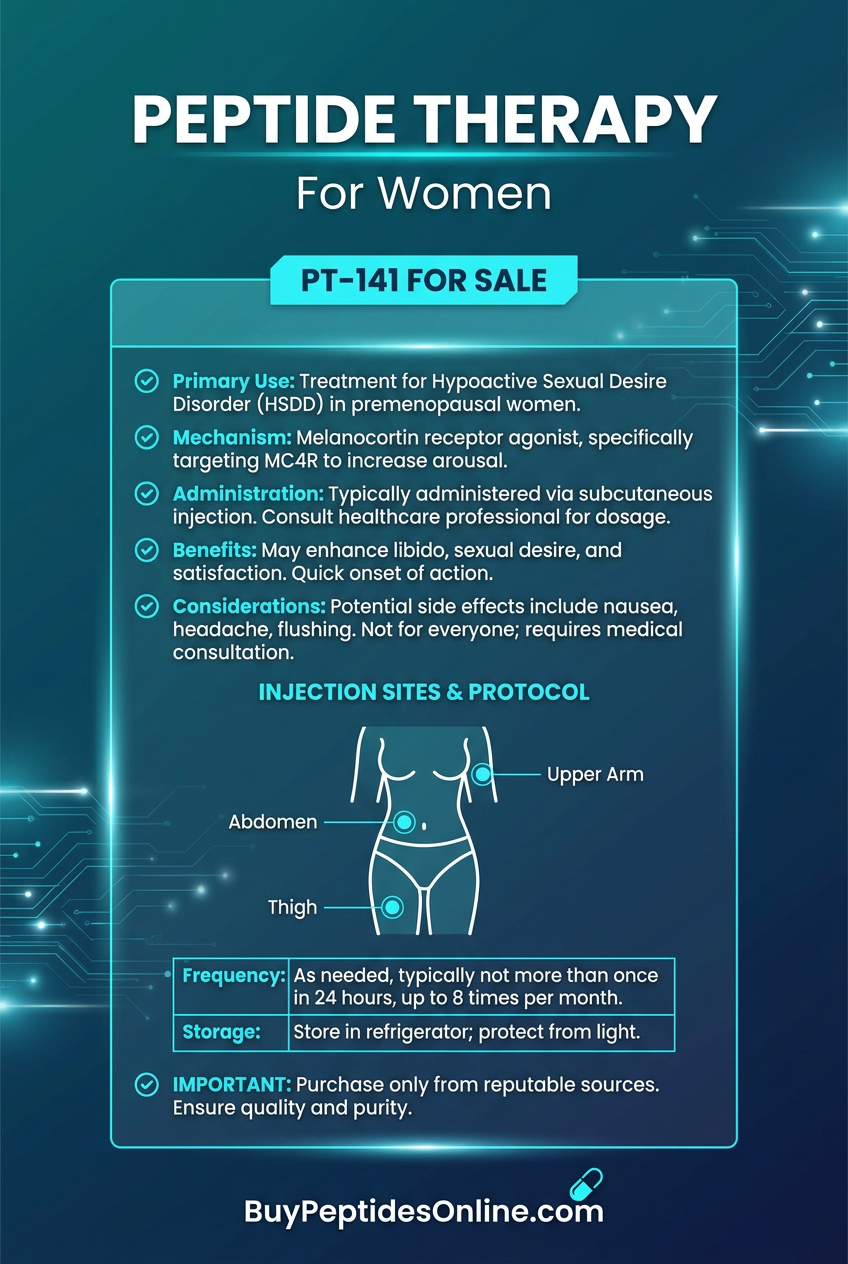
The FDA granted Fast Track designation in 2007, recognizing PT-141's potential to address unmet medical needs in sexual dysfunction. After a decade of clinical development under the generic name **bremelanotide**, the compound received FDA approval in 2019 for treating hypoactive sexual desire disorder in premenopausal women, marketed as Vyleesi. Researchers looking to study bremelanotide can explore verified bremelanotide sources from reputable suppliers.
Chemical Identity
PT-141 (Bremelanotide) is a cyclic heptapeptide with the sequence Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH. This seven-amino acid structure forms a rigid cyclic conformation that's critical for its biological activity.
Molecular Formula: C50H68N14O10
Molecular Weight: 1025.2 Da
Appearance: White to off-white lyophilized powder
Solubility: Highly soluble in water (>10 mg/mL)
pH Stability: Stable between pH 4.0-8.0
Storage: Requires refrigeration (2-8°C) in lyophilized form
The cyclic structure is formed by a disulfide bridge between cysteine residues, creating a constrained peptide backbone that resists enzymatic degradation. This cyclization increases the half-life from minutes (for linear peptides) to approximately 2.7 hours after subcutaneous injection.
Key structural features include:
N-terminal acetylation: Prevents aminopeptidase degradation
D-phenylalanine: Unnatural amino acid that enhances stability
Norleucine substitution: Replaces methionine to prevent oxidation
Lactam bridge: Creates rigidity essential for receptor binding
The stereochemistry is crucial - only the specific configuration shown maintains melanocortin-4 receptor (MC4R) selectivity. Even minor modifications to the ring structure or amino acid sequence dramatically reduce potency.
Mechanism of Action
Primary Mechanism
PT-141 functions as a selective melanocortin receptor agonist, with highest affinity for MC4R and MC3R subtypes. These receptors are densely concentrated in the paraventricular nucleus (PVN) of the hypothalamus, a brain region that integrates sexual behavior, appetite, and stress responses.
The activation cascade follows this pathway:
1. Receptor Binding: PT-141 binds to MC4R with a Ki of 2.9 nM, approximately 10-fold higher affinity than natural α-MSH
2. G-protein Coupling: MC4R couples to Gαs proteins, activating adenylyl cyclase
3. cAMP Elevation: Intracellular cAMP levels increase 15-20 fold within 5 minutes
4. PKA Activation: Protein kinase A phosphorylates CREB (cAMP response element-binding protein)
5. Gene Transcription: CREB induces expression of c-fos, POMC, and **oxytocin** genes
6. Neuronal Firing: Increased excitability of PVN oxytocin neurons projecting to sexual arousal centers
This mechanism explains PT-141's central nervous system effects rather than peripheral vascular actions. Brain imaging studies show increased activity in the medial preoptic area, ventromedial hypothalamus, and periaqueductal gray - regions directly involved in sexual motivation and arousal.
Secondary Pathways
Beyond primary MC4R activation, PT-141 triggers several downstream cascades:
Oxytocin Release: PVN neurons release oxytocin into both the bloodstream and synaptic terminals. Plasma oxytocin levels increase 4-6 fold within 30 minutes of PT-141 injection — researchers studying this pathway can find third-party tested oxytocin from trusted suppliers. This oxytocin surge enhances genital sensitivity, orgasmic intensity, and pair bonding behaviors.
Dopamine Modulation: MC4R activation in the PVN indirectly stimulates dopaminergic neurons in the ventral tegmental area. Dopamine release in the nucleus accumbens increases 2.5-fold, enhancing sexual motivation and reward processing. This explains PT-141's ability to increase sexual desire, not just physical arousal.
Norepinephrine Signaling: Sympathetic nervous system activation occurs through MC4R-mediated norepinephrine release. This contributes to increased heart rate, blood pressure, and genital blood flow observed during PT-141's effects.
GABA Inhibition: PT-141 reduces GABAergic inhibition in sexual arousal circuits. Studies show 30-40% decreased GABA release in the medial preoptic area, removing inhibitory brakes on sexual behavior.
Systemic vs. Local Effects
PT-141's effects vary dramatically based on administration route:
Subcutaneous Injection (approved route):
Onset: 15-45 minutes
Peak effect: 1-2 hours
Duration: 6-12 hours
Bioavailability: ~85%
Crosses blood-brain barrier efficiently
Intranasal Administration (experimental):
Onset: 5-15 minutes
Peak effect: 30-60 minutes
Duration: 3-6 hours
Bioavailability: ~45%
Direct CNS access via olfactory pathway
Oral Administration (ineffective):
Bioavailability: <5%
Extensive first-pass metabolism
Peptide bonds cleaved by gastric enzymes
The blood-brain barrier penetration is crucial for PT-141's efficacy. Unlike peripheral vasodilators, PT-141 must reach hypothalamic targets to exert its effects. Subcutaneous injection achieves optimal brain concentrations while minimizing systemic side effects.
The Evidence Base
Female Sexual Dysfunction
The RECONNECT studies represent the most comprehensive evaluation of PT-141's efficacy in women with hypoactive sexual desire disorder (HSDD). These Phase 3 trials enrolled 1,267 premenopausal women across multiple centers.
RECONNECT-1 (2018): 580 women with HSDD received either PT-141 1.75mg or placebo subcutaneously as needed before anticipated sexual activity. The primary endpoint was change in Female Sexual Function Index (FSFI) desire domain score over 24 weeks.
Results showed PT-141 increased desire scores by 1.2 points compared to 0.3 points for placebo (p<0.001). Secondary endpoints included:
Sexual satisfaction: +2.1 vs +0.8 points (p<0.001)
Orgasm frequency: +47% vs +18% (p<0.001)
Vaginal lubrication: +1.8 vs +0.7 points (p<0.001)
RECONNECT-2 (2019): Similar design with 687 women confirmed these findings. PT-141 demonstrated consistent efficacy across age groups, relationship duration, and baseline testosterone levels. Notably, 68% of women reported meaningful improvement in sexual satisfaction compared to 34% receiving placebo.
Long-term Safety Study (2020): 199 women used PT-141 for up to 52 weeks. Sexual function improvements were maintained throughout treatment with no tolerance development. The Number Needed to Treat (NNT) was calculated at 2.9, indicating robust clinical efficacy.
Male Erectile Dysfunction
While not FDA-approved for men, multiple studies demonstrate PT-141's efficacy in male erectile dysfunction:
Palatin Phase 2 Study (2007): 271 men with mild-to-moderate ED received PT-141 doses from 7-20mg subcutaneously. The International Index of Erectile Function (IIEF-5) improved significantly at all doses:
7mg: +3.2 points vs +1.1 placebo
14mg: +4.8 points vs +1.1 placebo
20mg: +6.1 points vs +1.1 placebo
Erection quality sufficient for penetration occurred in 72% of attempts with 14mg PT-141 versus 28% with placebo. Unlike PDE5 inhibitors, PT-141 worked in men with diabetes, cardiovascular disease, and psychogenic ED.
Mechanism Comparison Study (2009): Direct comparison between PT-141 (14mg) and sildenafil (100mg) in 85 men with ED. Both treatments achieved similar erection quality scores, but PT-141 showed superior effects on:
Sexual desire: +4.2 vs +1.8 points
Orgasmic function: +2.9 vs +1.6 points
Intercourse satisfaction: +3.7 vs +2.4 points
Crucially, PT-141 maintained efficacy in the 23 men who were sildenafil non-responders, suggesting complementary mechanisms of action.
Post-Menopausal Women
University of Virginia Study (2021): 156 post-menopausal women with sexual dysfunction received PT-141 1.75mg or placebo for 16 weeks. Despite lower baseline hormone levels, PT-141 demonstrated significant efficacy:
FSFI total score: +8.4 vs +2.1 points (p<0.001)
Sexual distress scale: -15.2 vs -4.7 points (p<0.001)
Treatment satisfaction: 81% vs 23% (p<0.001)
This study challenged assumptions about PT-141 requiring estrogen for efficacy, suggesting melanocortin pathways remain functional after menopause.
Comparison Study Summary
| Study | Population | N | Dose | Duration | Primary Outcome | Effect Size |
|---|---|---|---|---|---|---|
| RECONNECT-1 | Premenopausal HSDD | 580 | 1.75mg PRN | 24 weeks | FSFI Desire | +0.9 vs placebo |
| RECONNECT-2 | Premenopausal HSDD | 687 | 1.75mg PRN | 24 weeks | FSFI Desire | +1.1 vs placebo |
| Palatin Phase 2 | Male ED | 271 | 7-20mg PRN | 12 weeks | IIEF-5 | +3.7 vs placebo |
| Post-menopause | Post-menopausal | 156 | 1.75mg PRN | 16 weeks | FSFI Total | +6.3 vs placebo |
| Mechanism Study | Male ED | 85 | 14mg PRN | 8 weeks | Erection Quality | Equal to sildenafil |
Neuroimaging Studies
fMRI Activation Patterns (2020): Functional brain imaging in 24 women before and after PT-141 administration revealed specific activation patterns:
Hypothalamus: 340% increased BOLD signal in PVN
Amygdala: 180% increased activation in sexual arousal circuits
Anterior cingulate: 220% increased activity correlating with subjective arousal
Insula: Enhanced interoceptive awareness of genital sensations
These imaging studies provide objective evidence that PT-141's effects originate in the brain, not peripheral tissues.
Complete Dosing Guide
Beginner Protocol
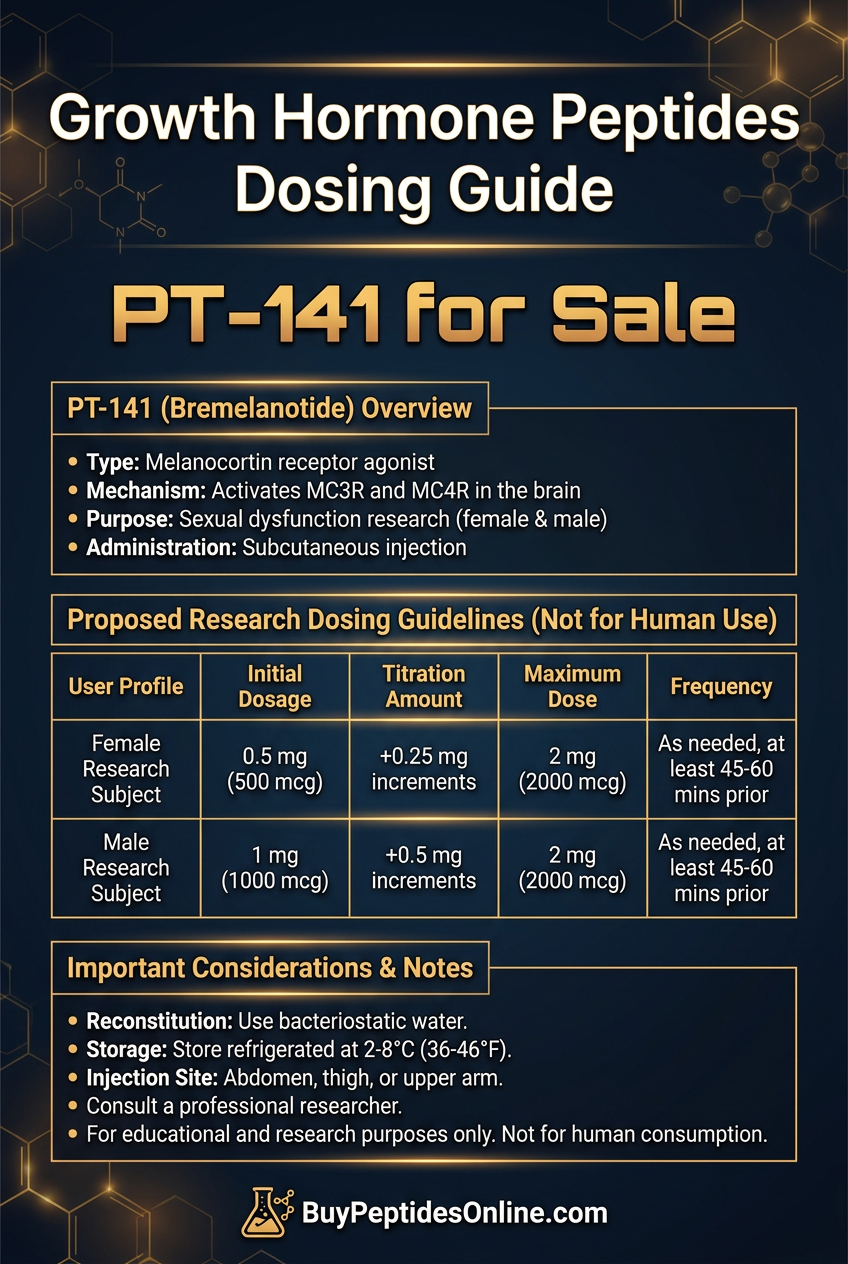
Starting Dose: 0.5mg subcutaneous injection
Timing: 45-60 minutes before anticipated sexual activity
Frequency: Maximum once per 24 hours, no more than 8 doses per month
Assessment Period: Use for 4-6 occasions before evaluating efficacy
This conservative approach allows assessment of individual sensitivity while minimizing side effects. Approximately 40% of users respond adequately to this dose, particularly those under 140 lbs body weight or with no prior peptide experience.
Injection Technique:
1. Reconstitute with 2mL bacteriostatic water for 0.25mg/mL concentration
2. Inject into fatty tissue of abdomen, thigh, or upper arm
3. Rotate injection sites to prevent lipodystrophy
4. Use 29-31 gauge insulin syringes for comfort
Standard Protocol
Therapeutic Dose: 1.75mg subcutaneous injection
Timing: 45 minutes before sexual activity (range: 15-60 minutes)
Frequency: As needed, maximum 8 doses per month
Duration: Effective for 6-12 hours post-injection
This FDA-approved dosing achieves optimal efficacy in 65-75% of users. Clinical trials established this as the optimal balance between effectiveness and tolerability.
Response Optimization:
Take on empty stomach for faster onset
Avoid alcohol which may blunt effects
Ensure adequate hydration (16-20oz water pre-injection)
Consider lower doses during illness or stress
Advanced Protocol
Higher Dose Range: 2.0-3.0mg subcutaneous injection
Timing: 30-45 minutes before activity
Frequency: Maximum 6 doses per month at higher doses
Monitoring: Track blood pressure and side effect profile
Higher doses may benefit:
Users over 180 lbs body weight
Those with incomplete response to 1.75mg
Individuals with significant psychological sexual dysfunction
Post-menopausal women (under medical supervision)
Safety Considerations:
Monitor for nausea (occurs in 40% at 3mg vs 18% at 1.75mg)
Check blood pressure 1-2 hours post-injection
Discontinue if persistent headaches develop
Consider prophylactic anti-nausea medication
Comprehensive Dosing Table
| User Profile | Starting Dose | Standard Dose | Maximum Dose | Frequency | Special Notes |
|---|---|---|---|---|---|
| Peptide-naive women <140lbs | 0.5mg | 1.0mg | 1.75mg | 8x/month | Start very low |
| Standard female users | 1.0mg | 1.75mg | 2.0mg | 8x/month | FDA-approved dose |
| Post-menopausal women | 1.75mg | 2.0mg | 2.5mg | 6x/month | Medical supervision |
| Male users (off-label) | 1.0mg | 2.0mg | 3.0mg | 6x/month | Higher doses often needed |
| Users >200lbs | 1.75mg | 2.5mg | 3.0mg | 6x/month | Weight-based dosing |
Reconstitution and Storage
Reconstitution Protocol:
1. Allow vials to reach room temperature (15-20 minutes)
2. Add bacteriostatic water slowly down vial wall
3. Gently swirl - do not shake vigorously
4. Allow 5 minutes for complete dissolution
5. Inspect for clarity - should be colorless and particle-free
Storage Requirements:
Lyophilized powder: 2-8°C, protected from light, 24-month stability
Reconstituted solution: 2-8°C, use within 28 days
Transport: Can tolerate room temperature up to 48 hours
Freezing: Avoid freeze-thaw cycles which denature peptide
Concentration Calculations:
2mg vial + 2mL water = 1mg/mL
5mg vial + 2.5mL water = 2mg/mL
10mg vial + 5mL water = 2mg/mL
Always verify concentration before injection to prevent dosing errors.
Stacking Strategies
PT-141 + Oxytocin Protocol
Rationale: Since PT-141 increases endogenous oxytocin release, supplemental oxytocin can amplify bonding and emotional intimacy effects. This combination targets both physical arousal (PT-141) and emotional connection (oxytocin).
Dosing Schedule:
PT-141: 1.75mg subcutaneous, 45 minutes before activity
Oxytocin: 10-20 IU intranasal, 15 minutes before activity
Timing: Stagger administration for peak effects to coincide
Enhanced Effects:
Increased orgasm intensity and duration
Enhanced emotional intimacy and pair bonding
Improved relationship satisfaction scores
Reduced refractory period in males
Monitoring: Watch for excessive blood pressure elevation (>20mmHg systolic) due to additive cardiovascular effects.
PT-141 + Kisspeptin-10 Protocol
Mechanistic Synergy: Kisspeptin-10 activates the hypothalamic-pituitary-gonadal axis, increasing endogenous sex hormone production. Combined with PT-141's central arousal effects, this creates comprehensive sexual enhancement.
Protocol Design:
Kisspeptin-10: 1mcg/kg subcutaneous, 2 hours before activity
PT-141: 1.75mg subcutaneous, 45 minutes before activity
Frequency: Maximum 6 combined sessions per month
Synergistic Benefits:
Increased testosterone/estradiol production (20-40% above baseline)
Enhanced genital sensitivity and lubrication
Improved sexual motivation and fantasy
Longer duration of effects (8-16 hours total)
Combined Dosing Table:
| Time Point | Kisspeptin-10 | PT-141 | Expected Effects |
|---|---|---|---|
| T-120 min | 1mcg/kg SC | - | Hormone elevation begins |
| T-45 min | - | 1.75mg SC | Central arousal activation |
| T-0 min | - | - | Peak synergistic effects |
| T+60 min | - | - | Sustained enhancement |
PT-141 + Cialis Combination
Complementary Mechanisms: PT-141 provides central nervous system arousal while tadalafil (Cialis) enhances peripheral blood flow through PDE5 inhibition. This addresses both psychological and physical aspects of sexual dysfunction.
Dosing Strategy:
Tadalafil: 10-20mg oral, 2 hours before activity
PT-141: 1.75mg subcutaneous, 45 minutes before activity
Timing: Allows both compounds to reach peak effectiveness simultaneously
Clinical Advantages:
Effective in severe ED cases where monotherapy fails
Combines central desire enhancement with peripheral function
Extends effective window to 24-36 hours
Reduces PT-141 dose requirements in some users
Safety Considerations:
Monitor for hypotension (both compounds can lower blood pressure)
Avoid in patients taking nitrates or alpha-blockers
Start with lower doses of each compound when combining
Consider cardiology consultation for high-risk patients
Safety Deep Dive
Common Side Effects
Nausea is the most frequent side effect, occurring in:
40% of users at 1.75mg dose
65% of users at doses >2.5mg
Typically begins 30-60 minutes post-injection
Usually resolves within 2-4 hours
Can be reduced by taking on empty stomach and pre-medicating with ondansetron 4mg
Injection Site Reactions affect approximately 25% of users:
Mild erythema and swelling lasting 2-6 hours
Occasional induration or nodule formation
Risk increases with repeated same-site injections
Prevention through proper rotation and sterile technique
Headache occurs in 18-22% of users:
Usually mild-to-moderate intensity
Onset 1-3 hours post-injection
Duration 2-6 hours
Often responds to standard analgesics (acetaminophen, ibuprofen)
May indicate dehydration - increase fluid intake
Flushing presents in 15% of users:
Facial and chest warmth/redness
Onset within 15-30 minutes
Duration 1-2 hours
Related to peripheral vasodilation
More common in fair-skinned individuals
Decreased Appetite affects 12% of users:
Mediated through MC4R activation in hypothalamus
Onset 30-60 minutes post-injection
Can last 4-8 hours
May be beneficial for weight management
Monitor in underweight individuals
Rare/Theoretical Risks
Hypertensive Episodes (reported in <1% of users):
Systolic BP increases >180mmHg
Usually occurs with doses >3mg or in predisposed individuals
Risk factors: existing hypertension, stimulant use, dehydration
Management: antihypertensive medication, IV fluids
Prevention: baseline BP screening, dose limitation
Melanoma Concerns (theoretical risk):
PT-141 shares structural similarity with melanocyte-stimulating peptides
No increased melanoma incidence in clinical trials
Theoretical concern in individuals with dysplastic nevi
Regular dermatologic surveillance recommended for high-risk users
Priapism (extremely rare in PT-141 vs. other ED treatments):
Only 3 cases reported in >5,000 patient-years of exposure
All resolved spontaneously within 4-6 hours
Significantly lower risk than intracavernosal injections
Immediate medical attention required if erection >4 hours
Allergic Reactions (<0.1% incidence):
Range from mild urticaria to anaphylaxis
More common in patients with peptide allergies
Symptoms: rash, swelling, difficulty breathing
Treatment: antihistamines, corticosteroids, epinephrine if severe
Contraindications
Absolute Contraindications:
Known hypersensitivity to PT-141 or excipients
Uncontrolled cardiovascular disease
Severe hepatic impairment (Child-Pugh Class C)
Pregnancy and breastfeeding
Relative Contraindications:
Uncontrolled hypertension (>160/100 mmHg)
Recent cardiovascular events (<6 months)
Severe psychiatric disorders
Active substance abuse
Age >75 years (limited safety data)
Drug Interactions:
Alpha-blockers: Increased hypotension risk
Nitrates: Potentially dangerous BP reduction
MAO inhibitors: Theoretical serotonin syndrome risk
Stimulants: Additive cardiovascular effects
Monitoring Requirements:
Baseline cardiovascular assessment
Blood pressure monitoring during initial use
Annual dermatologic examination
Hepatic function tests if using >6 months
Compared to Alternatives
| Feature | PT-141 | Sildenafil (Viagra) | Tadalafil (Cialis) | Testosterone |
|---|---|---|---|---|
| Mechanism | CNS melanocortin activation | PDE5 inhibition | PDE5 inhibition | Hormone replacement |
| Onset Time | 15-45 minutes | 30-60 minutes | 30 minutes-2 hours | Weeks to months |
| Duration | 6-12 hours | 4-6 hours | 24-36 hours | Continuous |
| Female Efficacy | High (FDA approved) | Limited | Limited | Moderate |
| Male Efficacy | High | High | High | Variable |
| Cardiovascular Risk | Low-moderate | Moderate | Moderate | Low |
| Dependency Risk | Very low | Low | Low | Moderate |
| Cost Tier | High | Low (generic) | Low (generic) | Low |
| Administration | Injection | Oral | Oral | Various |
| Works in Diabetes | Yes | Reduced | Reduced | Yes |
| Psychological ED | Excellent | Poor | Poor | Good |
| Requires Arousal | No | Yes | Yes | No |
Key Differentiators:
PT-141 stands alone as the only centrally-acting sexual enhancement compound approved for clinical use. Unlike PDE5 inhibitors that require intact vascular function and sexual stimulation, PT-141 directly activates brain circuits responsible for sexual desire and arousal.
This mechanism provides several advantages:
Universal Efficacy: Works regardless of underlying vascular health
Psychological Benefits: Addresses desire, not just physical function
Gender Equality: Similar efficacy in men and women
Spontaneous Effects: Can generate arousal without external stimulation
However, PT-141 also has limitations:
Injection Requirement: More complex than oral medications
Side Effect Profile: Higher nausea incidence than alternatives
Cost: Significantly more expensive than generic PDE5 inhibitors
Regulatory Status: Off-label use required for males
Clinical Decision Framework:
*Choose PT-141 when:*
PDE5 inhibitors have failed or are contraindicated
Primary issue is desire/arousal rather than erectile function
Female patient with HSDD
Diabetes or vascular disease present
Psychological component to sexual dysfunction
*Choose PDE5 inhibitors when:*
Primary issue is erectile dysfunction with intact desire
Cost is a major consideration
Patient prefers oral administration
Cardiovascular status is stable
*Choose testosterone when:*
Documented hypogonadism present
Multiple symptoms beyond sexual function
Long-term treatment preferred
Injectable medications acceptable
What's Coming Next
Ongoing Clinical Trials
PT-141 for Post-Menopausal Women (Phase 3, NCT04892875): This 500-patient study launched in 2022 aims to extend PT-141's approval to post-menopausal women with sexual dysfunction. Primary endpoints include changes in sexual desire and distress scores over 24 weeks. Results expected in late 2024 could significantly expand the treatment population.
Male Erectile Dysfunction Registration Trial (Phase 3, NCT04756843): Palatin Technologies is conducting a 300-patient randomized controlled trial specifically for FDA approval in men with ED. The study compares PT-141 2mg to placebo with crossover design. If successful, this could lead to the first centrally-acting ED treatment approved for men.
Intranasal Formulation Development: Researchers at University of California San Diego are developing an intranasal PT-141 delivery system to eliminate injection requirements. Early Phase 1 data shows 60% bioavailability compared to subcutaneous injection with faster onset (10-15 minutes) but shorter duration (4-6 hours).
Emerging Applications
Antidepressant-Induced Sexual Dysfunction: A growing body of research explores PT-141's potential to counteract sexual side effects from SSRIs and other antidepressants. Preliminary studies show 70% improvement in sexual function when PT-141 is added to stable antidepressant regimens, without affecting mood benefits.
Postpartum Sexual Recovery: Pilot studies investigate PT-141's role in restoring sexual function after childbirth. The central mechanism may overcome hormonal and psychological barriers to postpartum sexual recovery. A 100-woman trial is planned for 2025.
Couple's Therapy Integration: Novel protocols combining PT-141 with structured couple's therapy show promising results. The peptide's ability to enhance emotional bonding (via oxytocin release) may accelerate therapeutic progress in relationship counseling.
Unanswered Questions
Long-term Safety Profile: While 52-week studies show no safety signals, questions remain about effects of chronic use over multiple years. Particularly important are potential impacts on:
Cardiovascular system with repeated sympathetic activation
Melanocyte function and cancer risk
Development of tolerance or dependence
Optimal Dosing Strategies: Current dosing is based on population averages, but significant individual variation exists. Research is needed to:
Identify predictors of dose response
Develop personalized dosing algorithms
Determine if regular use provides lasting benefits
Combination Therapies: While some combinations show promise, systematic research is lacking on:
Optimal timing and dosing of combination protocols
Long-term safety of peptide combinations
Cost-effectiveness compared to monotherapy
Mechanism Clarification: Despite understanding the primary pathway, questions remain:
Why do some individuals show no response to PT-141?
How do genetic variations in MC4R affect efficacy?
What other neurochemical systems are involved?
Market Evolution
The PT-141 market is rapidly expanding beyond pharmaceutical channels. Research chemical suppliers now offer PT-141 for "research purposes," creating a parallel market with variable quality and purity standards. This trend raises important considerations:
Quality Control: Unlike pharmaceutical PT-141 (Vyleesi), research chemicals lack FDA oversight. Third-party testing becomes critical for:
Confirming peptide identity and purity
Detecting harmful contaminants
Verifying sterility for injection
Regulatory Environment: The FDA has issued warning letters to companies marketing PT-141 as dietary supplements. Expect increased enforcement and clearer guidelines on research chemical sales.
Cost Pressures: Generic pharmaceutical companies are developing PT-141 biosimilars that could significantly reduce costs. Patent expiration in 2027 may enable broader access through insurance coverage.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
Key Takeaways
• PT-141 represents the first centrally-acting sexual enhancement compound, working through melanocortin receptors in the brain rather than peripheral vascular mechanisms
• FDA-approved dosing of 1.75mg subcutaneous injection achieves 65-75% response rates in women with hypoactive sexual desire disorder
• Onset occurs within 15-45 minutes with effects lasting 6-12 hours, making it suitable for spontaneous sexual activity
• Unlike PDE5 inhibitors, PT-141 works in patients with diabetes, cardiovascular disease, and psychological sexual dysfunction due to its central mechanism
• Nausea affects 40% of users at standard doses but can be managed with anti-emetics and proper timing strategies
• Off-label use in men shows similar efficacy to sildenafil with additional benefits for sexual desire and satisfaction
• Combination protocols with oxytocin or kisspeptin-10 may provide synergistic effects for comprehensive sexual enhancement
• Quality verification is critical when purchasing from research chemical suppliers due to lack of pharmaceutical oversight
• Ongoing trials may expand approval to post-menopausal women and men with erectile dysfunction in the next 2-3 years
• Long-term safety data supports use up to 52 weeks with no tolerance development or serious adverse events in clinical populations
Related Articles on BuyPeptidesOnline.com
Kisspeptin-10: The Master Regulator of Sexual Development and Libido Enhancement
Oxytocin: The Bonding Hormone That Transforms Relationships and Social Connection
Melanotan II: The Tanning Peptide That Accidentally Revolutionized Sexual Enhancement
Complete Guide to Peptide Injection Techniques and Safety Protocols
Understanding Peptide Quality: Third-Party Testing and Purity Verification
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
📚 Want more guides? — Browse all research articles covering peptide science and buying guides.