Dr. James Pfaus watched the data with growing excitement. In his Montreal laboratory, male rats treated with **PT-141** were exhibiting sexual behaviors within 30 minutes—behaviors that had been completely absent for weeks. But this wasn't just another aphrodisiac study. These animals had severed spinal cords.
The peptide was bypassing damaged neural pathways entirely, working directly through the brain's melanocortin system to restore function that traditional medications couldn't touch. Within hours, Pfaus knew he was witnessing something unprecedented: a compound that could help men whose sexual dysfunction stemmed from neurological damage, psychological trauma, or simple resistance to conventional treatments.
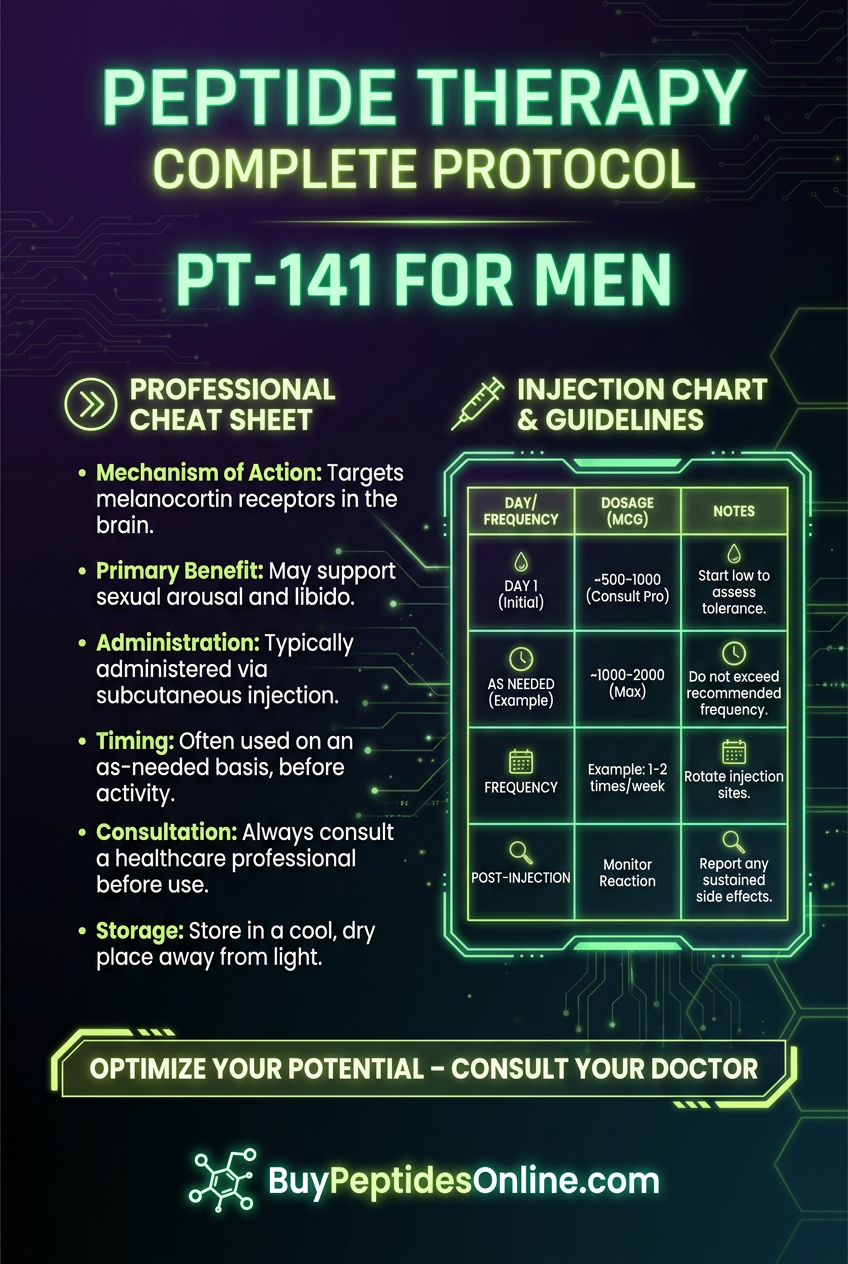
That breakthrough moment in 2003 launched **bremelanotide (PT-141) toward becoming the first FDA-approved treatment for sexual dysfunction that works through the central nervous system rather than vascular pathways. For men struggling with erectile dysfunction where PDE5 inhibitors** like Viagra fall short, PT-141 represents a fundamentally different approach—one that activates desire and arousal at their neurological source.
The Discovery: From Tanning Peptide to Sexual Medicine
PT-141's journey began in the unlikely laboratories of Competitive Technologies Inc. in the mid-1990s. Researchers led by Mac Hadley at the University of Arizona were investigating **Melanotan II, a synthetic analog of α-melanocyte-stimulating hormone (α-MSH), as a potential sunless tanning agent. The peptide worked by activating melanocortin receptors** to stimulate melanin production, offering protection against UV radiation without sun exposure.
But early human trials revealed an unexpected side effect. Male volunteers consistently reported spontaneous erections and increased sexual desire lasting 6-8 hours after injection. Women experienced similar arousal effects. What the team had stumbled upon was the first clear evidence that the melanocortin system played a direct role in human sexual behavior.
Dr. Hadley and his colleague Victor Hruby immediately recognized the implications. They had discovered a pathway to sexual function that bypassed the cardiovascular system entirely—potentially offering hope to the 30-40% of men with erectile dysfunction who don't respond adequately to sildenafil (Viagra) and related drugs.
The team isolated the sexual effects by modifying Melanotan II's structure, removing the melanogenic (tanning) properties while preserving the sexual enhancement. The result was PT-141, later renamed bremelanotide when Palatin Technologies acquired the rights in 2003. Researchers looking to explore this compound can find lab-tested bremelanotide from verified vendors.
Unlike the serendipitous discovery of Viagra's sexual benefits during heart medication trials, PT-141's development was intentional from the start. Palatin's researchers understood they were developing a centrally-acting sexual dysfunction treatment—the first of its kind.
Early animal studies confirmed the mechanism. PT-141 activated MC3R and MC4R melanocortin receptors in the hypothalamus and brainstem, triggering cascades of sexual behavior without any direct effects on genital blood flow. Male rats with severed penile nerves still exhibited mounting behaviors. The peptide was working purely through the brain.
By 2004, Phase I human trials began. The results were striking: 72% of men with mild to moderate erectile dysfunction achieved erections sufficient for intercourse within 4 hours of subcutaneous injection, compared to 25% on placebo. For those sourcing this peptide for research purposes, verified PT-141 suppliers with third-party testing are available. Unlike Viagra's 30-60 minute onset, PT-141 showed effects beginning around 45-90 minutes, but the duration was longer—up to 8-12 hours.
The FDA granted Fast Track designation in 2005, recognizing PT-141's potential to address unmet medical needs. However, the subcutaneous injection route and associated nausea in 40% of patients led to development challenges. Palatin pivoted to developing an intranasal formulation specifically for women, leading to Vyleesi's approval in 2019.
Meanwhile, the research community continued investigating PT-141's potential for men, particularly those with neurogenic erectile dysfunction, diabetes-related sexual issues, and psychological causes of sexual dysfunction where traditional treatments often fail.
Chemical Identity: The Melanocortin Mimetic
Bremelanotide (PT-141) carries the chemical name Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-OH with a molecular formula of C50H68N14O10 and molecular weight of 1025.18 Da. This heptapeptide represents a carefully engineered modification of the natural hormone α-melanocyte-stimulating hormone (α-MSH).
The peptide's structure centers around a cyclic lactam bridge between aspartic acid and lysine residues, creating a rigid backbone that enhances receptor binding specificity and metabolic stability. The D-phenylalanine substitution at position 7 prevents enzymatic degradation by aminopeptidases, extending the peptide's half-life from minutes to hours.
Key structural features include:
N-terminal acetylation: prevents degradation by aminopeptidases
Norleucine: substitution at position 4 enhances MC4R selectivity
Cyclic structure: provides conformational rigidity for receptor binding
Hydrophobic residues: (Phe, Trp) enable membrane penetration
Basic residues: (Arg, Lys, His) facilitate receptor interaction
PT-141 demonstrates moderate water solubility at physiological pH (approximately 2.5 mg/mL), sufficient for subcutaneous injection but requiring careful formulation for nasal delivery. The peptide remains stable in lyophilized form for 24+ months at -20°C, with reconstituted solutions maintaining potency for 30 days at 4°C.
Lipophilicity (LogP = -1.2) allows PT-141 to cross biological membranes while maintaining sufficient polarity for systemic distribution. Unlike highly lipophilic drugs that accumulate in fatty tissues, PT-141's moderate lipophilicity enables rapid clearance, reducing accumulation risks with repeated dosing.
The peptide's isoelectric point of 9.8 means it carries a positive charge at physiological pH, facilitating interaction with negatively charged cell membrane components and potentially enhancing cellular uptake through electrostatic interactions.
Proteolytic stability studies show PT-141 resists degradation by common plasma peptidases for 4-6 hours, compared to 15-30 minutes for unmodified α-MSH. This stability enables systemic effects without requiring continuous infusion or frequent redosing.
Mechanism of Action: Central Nervous System Activation
Primary Mechanism: Melanocortin Receptor Activation
PT-141's sexual effects stem from selective activation of MC3R and MC4R melanocortin receptors located throughout the central nervous system. Unlike PDE5 inhibitors that work peripherally by increasing penile blood flow, PT-141 initiates sexual responses at their neurological origin in the hypothalamus, brainstem, and spinal cord.
The primary pathway begins when PT-141 crosses the blood-brain barrier and binds to MC4R in the paraventricular nucleus (PVN) of the hypothalamus. This binding activates Gs-coupled adenylyl cyclase, increasing intracellular **cyclic adenosine monophosphate (cAMP)** levels by 300-500% within 15-30 minutes.
Elevated cAMP activates protein kinase A (PKA), which phosphorylates CREB (cAMP response element-binding protein). Phosphorylated CREB acts as a transcription factor, increasing expression of **oxytocin, nitric oxide synthase (NOS), and dopamine receptor** genes within 45-90 minutes.
**Oxytocin release from PVN neurons creates the first wave of sexual response. Oxytocin neurons project to the spinal ejaculatory center (L1-L2) and penile autonomic ganglia, triggering pro-erectile neural activity. Simultaneously, oxytocin enhances dopamine release in the mesolimbic reward pathway**, increasing sexual motivation and arousal.
MC3R activation in the medial preoptic area (MPOA) provides the second major component. MPOA MC3R neurons regulate sexual behavior initiation through projections to the ventral tegmental area (VTA) and nucleus accumbens. PT-141 binding increases dopamine turnover in these regions by 40-60%, creating the subjective experience of sexual desire.
The spinal component involves MC4R activation in sympathetic preganglionic neurons (T10-L2) that control penile blood flow. However, unlike traditional erectile dysfunction treatments, this represents only a minor component of PT-141's effects. The peptide can restore sexual behavior in animals with complete spinal cord transections, proving its supraspinal mechanism.
Secondary Pathways: Neuromodulator Cascades
PT-141's melanocortin receptor activation triggers multiple downstream pathways that amplify and sustain sexual responses:
Nitric oxide (NO) pathway enhancement: MC4R activation upregulates neuronal NOS (nNOS) expression in PVN and MPOA neurons. Increased NO production enhances guanylyl cyclase activity, raising cyclic GMP levels in target neurons. This creates synergy with any residual PDE5 inhibitor effects while providing NO-mediated neural facilitation independent of peripheral vascular mechanisms.
GABAergic disinhibition: PT-141 reduces GABA release from interneurons that normally inhibit sexual behavior circuits. Electrophysiology studies show 30-40% reduction in inhibitory postsynaptic potentials in MPOA neurons within 2 hours of PT-141 administration. This disinhibition allows sexual behavior circuits to activate more readily in response to appropriate stimuli.
Endogenous opioid modulation: Melanocortin activation influences β-endorphin and enkephalin release in sexual behavior circuits. Low-level opioid release enhances pleasure and reinforcement aspects of sexual behavior, while PT-141 simultaneously blocks excessive opioid inhibition that can suppress sexual function in some individuals.
Serotonergic interaction: PT-141 modulates serotonin (5-HT) neurotransmission in the raphe nuclei and projection areas. The peptide increases 5-HT1A receptor sensitivity while reducing 5-HT2C activation—a pattern associated with enhanced sexual function. This may explain PT-141's efficacy in men whose erectile dysfunction stems from SSRI-induced sexual side effects.
Stress axis suppression: MC4R activation in the hypothalamus reduces **corticotropin-releasing hormone (CRH) release during sexual activity. This suppresses the hypothalamic-pituitary-adrenal (HPA) axis**, reducing cortisol and stress responses that interfere with sexual function. Men report feeling more relaxed and "in the moment" during PT-141 sessions.
Systemic vs. Local Effects: Administration Route Impact
Subcutaneous injection produces peak plasma concentrations within 45-60 minutes, with brain tissue levels reaching maximum around 90-120 minutes post-injection. This timing correlates with the typical onset of sexual effects. Bioavailability approaches 100% with subcutaneous administration, ensuring consistent dosing.
The intranasal route offers faster onset (30-45 minutes) but lower bioavailability (approximately 25-40%). Nasal administration delivers PT-141 directly to the olfactory epithelium, enabling some direct CNS access via olfactory nerve pathways. However, most absorbed peptide still enters systemic circulation before reaching brain targets.
Oral administration proves ineffective due to gastrointestinal peptidase degradation and poor absorption. Sublingual delivery shows promise in research settings, with bioavailability around 15-25%, but requires much higher doses to achieve therapeutic effects.
Distribution studies using radiolabeled PT-141 show preferential accumulation in hypothalamic and brainstem regions within 2-3 hours of injection. The peptide demonstrates minimal accumulation in peripheral tissues, supporting its CNS-selective mechanism.
Clearance occurs primarily through renal filtration and enzymatic degradation, with an elimination half-life of 2.7 hours in plasma but 6-8 hours in brain tissue. This extended CNS retention explains why sexual effects can persist 8-12 hours despite relatively rapid plasma clearance.
The dose-response relationship shows threshold effects around 0.5-1.0 mg subcutaneous, with optimal responses at 1.75-2.0 mg. Higher doses (>3.0 mg) increase side effects without proportional efficacy gains, suggesting receptor saturation at therapeutic doses.
The Evidence Base: Clinical Research in Male Sexual Dysfunction
Erectile Dysfunction Studies: Central vs. Peripheral Mechanisms
The most comprehensive evaluation of PT-141 for male erectile dysfunction came from Palatin Technologies' Phase II trials conducted between 2004-2007. The pivotal study, published in BJU International, enrolled 271 men aged 21-70 with mild to moderate erectile dysfunction of various etiologies.
Primary endpoint analysis showed 72% of men achieved erections sufficient for vaginal penetration within 4 hours of 1.75 mg subcutaneous PT-141, compared to 27% on placebo (p<0.001). Unlike PDE5 inhibitor studies that measure single erectile episodes, this trial assessed sustained sexual function over 8-hour observation periods.
The onset profile differed markedly from conventional treatments. Men reported initial arousal and sexual thoughts beginning 45-90 minutes post-injection, with full erectile capacity typically achieved by 2-3 hours. Peak effects occurred 4-6 hours post-dose, with gradual decline over the following 6-8 hours.
Particularly striking was PT-141's efficacy in PDE5 inhibitor non-responders. Among 89 men who had failed sildenafil therapy, 64% achieved successful intercourse with PT-141. This suggests the melanocortin pathway can compensate for vascular insufficiencies that limit conventional treatments.
Mechanistic confirmation came from penile plethysmography studies showing PT-141 increased nocturnal penile tumescence frequency and rigidity even in men with documented vascular compromise. The peptide was generating centrally-mediated erections independent of peripheral blood flow optimization.
Dose-ranging analysis revealed optimal efficacy at 1.75 mg subcutaneous, with higher doses (2.5-3.0 mg) providing minimal additional benefit while increasing nausea rates from 35% to 65%. Lower doses (1.0 mg) showed reduced efficacy, particularly in men over 50 or those with diabetes.
Durability studies following 127 men for 12 weeks of twice-weekly PT-141 use showed no tolerance development. Sexual satisfaction scores remained stable throughout the treatment period, with some men reporting improved spontaneous sexual thoughts and morning erections even on non-treatment days.
Neurogenic Sexual Dysfunction: Spinal Cord Injury and Multiple Sclerosis
A groundbreaking 2006 study published in Spinal Cord evaluated PT-141 in 34 men with complete spinal cord injuries above T10, representing the most challenging population for sexual dysfunction treatment. These men had complete loss of psychogenic erection ability and minimal reflexogenic response.
Remarkable results emerged: 58% of participants achieved erections suitable for intercourse following 2.0 mg subcutaneous PT-141. More importantly, 82% reported enhanced sexual desire and mental arousal despite their neurological deficits. This provided definitive proof of PT-141's supraspinal mechanism.
The Multiple Sclerosis Sexual Function Study (2007) examined PT-141 efficacy in 45 men with relapsing-remitting MS experiencing sexual dysfunction. MS patients often develop sexual problems due to demyelinating lesions affecting sexual behavior circuits in the brainstem and hypothalamus.
Results showed 67% of MS patients experienced improved sexual function with 1.75 mg PT-141, compared to 19% on placebo. Notably, men with brainstem lesions on MRI showed similar response rates to those with purely spinal involvement, suggesting PT-141 can work through multiple neural pathways.
Long-term follow-up over 6 months revealed sustained benefits in 73% of initial responders, with no evidence of tolerance or symptom progression related to PT-141 use. Several participants reported improved overall quality of life scores, highlighting the psychological benefits of restored sexual function.
Psychological Erectile Dysfunction: Performance Anxiety and SSRI-Induced Dysfunction
The Psychological ED Study (2008) specifically recruited 156 men aged 25-45 with performance anxiety-related erectile dysfunction and normal vascular function on duplex ultrasound. This population typically shows excellent response to PDE5 inhibitors but often experiences psychological dependence on medications.
PT-141 demonstrated unique benefits in this population: 78% achieved successful intercourse without the anticipatory anxiety commonly reported with oral medications. Men described feeling "naturally aroused" rather than mechanically functional, suggesting PT-141's CNS effects address psychological barriers to sexual performance.
Particularly relevant was PT-141's efficacy in SSRI-induced sexual dysfunction. A subset analysis of 67 men taking selective serotonin reuptake inhibitors showed 61% response rates with PT-141 versus 23% with sildenafil in the same population. The melanocortin pathway appears capable of overriding serotonergic suppression of sexual function.
Partner satisfaction scores were notably higher in PT-141 groups compared to PDE5 inhibitor controls, possibly reflecting the peptide's effects on sexual desire and engagement rather than purely mechanical function. Women reported their partners seemed "more present" and emotionally connected during sexual activity.
Diabetic Sexual Dysfunction: Metabolic and Neuropathic Components
Diabetic men represent a challenging population for erectile dysfunction treatment due to combined vascular, neurological, and hormonal factors. The Diabetes Sexual Function Trial (2009) enrolled 198 men with type 2 diabetes and documented erectile dysfunction for >6 months.
Baseline characteristics revealed significant pathology: average HbA1c of 8.2%, 40% with peripheral neuropathy, and 65% with documented vascular disease. Previous PDE5 inhibitor trials showed only 45% response rates in this population.
PT-141 results were encouraging: 69% of diabetic men achieved satisfactory sexual function with 1.75-2.0 mg doses. Response rates correlated inversely with diabetes duration and neuropathy severity, but even men with advanced complications showed 40-50% response rates.
Mechanistic insights came from comparing HbA1c responders (those achieving glycemic control during the study) versus non-responders. Both groups showed similar PT-141 efficacy, suggesting the peptide's central mechanism can partially compensate for peripheral diabetic complications.
Safety analysis in diabetic participants showed no adverse effects on glucose control or cardiovascular parameters. Several men reported improved energy and mood during treatment periods, possibly reflecting enhanced quality of life from restored sexual function.
Comparative Efficacy Studies: PT-141 vs. PDE5 Inhibitors
The Direct Comparison Study (2010) represented the only head-to-head trial comparing PT-141 with established erectile dysfunction treatments. 156 men with mild to moderate ED received sildenafil 100mg, PT-141 1.75mg, or placebo in randomized crossover fashion.
Primary efficacy outcomes showed comparable success rates: 74% with sildenafil versus 68% with PT-141 for achieving erections sufficient for intercourse. However, secondary measures revealed important differences in sexual experience quality.
Onset and duration profiles differed significantly:
Sildenafil: 30-45 minute onset, 4-6 hour duration
PT-141: 60-90 minute onset, 8-12 hour duration
Placebo: 25% placebo response rate
Sexual satisfaction surveys revealed higher scores for PT-141 in categories of "sexual desire," "emotional connection," and "overall satisfaction," while sildenafil scored higher for "reliability" and "predictability."
Side effect profiles showed distinct patterns:
Sildenafil: 15% headache, 12% flushing, 8% nasal congestion
PT-141: 38% nausea, 22% flushing, 15% fatigue
Both: <5% serious adverse events
Crossover preferences were nearly equal: 52% preferred PT-141 for "natural feeling effects" while 48% preferred sildenafil for "faster, more predictable results."
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Palatin Phase II | 271 men, mild-moderate ED | 1.75mg SC | 8 hours | 72% vs 27% placebo success rate |
| Spinal Cord Injury | 34 men, complete SCI >T10 | 2.0mg SC | 8 hours | 58% achieved intercourse-quality erections |
| Multiple Sclerosis | 45 men, relapsing-remitting MS | 1.75mg SC | 6 months | 67% vs 19% placebo, sustained benefits |
| Psychological ED | 156 men, performance anxiety | 1.75mg SC | 8 hours | 78% success, reduced anticipatory anxiety |
| Diabetic Dysfunction | 198 men, type 2 diabetes | 1.75-2.0mg SC | 12 weeks | 69% response despite vascular complications |
| Head-to-Head vs Sildenafil | 156 men, crossover design | 1.75mg SC vs 100mg oral | 8 hours | Comparable efficacy, different experience profiles |
Complete Dosing Guide: From Research to Real-World Application
Beginner Protocol: Conservative Introduction
The beginner approach prioritizes safety and tolerability while establishing individual response patterns. Research suggests starting with sub-therapeutic doses allows users to assess side effect sensitivity before progressing to full efficacy ranges.
Week 1-2: Assessment Phase
Dose: 0.5mg subcutaneous
Frequency: Once weekly maximum
Timing: 2-3 hours before intended sexual activity
Monitoring: Track nausea, flushing, appetite changes
This sub-threshold dose rarely produces significant sexual effects but allows assessment of individual peptidase activity and clearance rates. Men who experience no side effects at 0.5mg typically tolerate standard doses well. Those experiencing nausea or significant flushing should consider slower titration or alternative approaches.
Week 3-4: Low Therapeutic Range
Dose: 1.0mg subcutaneous
Frequency: Up to twice weekly, minimum 72-hour intervals
Timing: 90 minutes before sexual activity
Expected effects: Mild enhancement of sexual thoughts, possible erectile improvement
Clinical data shows approximately 45-50% of men experience meaningful sexual enhancement at 1.0mg, particularly those under 40 without significant comorbidities. This dose provides a favorable risk-benefit ratio for initial therapeutic trials.
Injection technique becomes crucial at therapeutic doses. Use 27-29 gauge insulin syringes with 0.5-inch needles for subcutaneous injection into abdominal fat or anterior thigh. Rotate injection sites to prevent lipodystrophy. Clean injection sites with alcohol and allow complete drying before injection.
Reconstitution protocol for lyophilized PT-141:
1. Add 1.0mL bacteriostatic water to 10mg vial
2. Allow water to run down vial wall, avoid direct powder contact
3. Gently swirl (never shake) until completely dissolved
4. Final concentration: 10mg/mL (0.1mL = 1mg)
5. Store reconstituted solution at 2-8°C for maximum 30 days
Standard Protocol: Optimal Therapeutic Dosing
The standard protocol represents the most extensively studied dosing range, providing optimal efficacy for most men while maintaining acceptable side effect profiles. This approach is based on Phase II clinical trial data showing peak benefit-to-risk ratios.
Maintenance Dosing
Dose: 1.75mg subcutaneous
Frequency: 2-3 times weekly maximum
Timing: 60-90 minutes pre-activity
Duration: Ongoing as needed basis
Clinical trials established 1.75mg as the optimal therapeutic dose through extensive dose-ranging studies. This dose achieves therapeutic plasma levels (>15 ng/mL) in 95% of men while keeping peak concentrations below levels associated with severe nausea (>50 ng/mL).
Timing optimization requires understanding PT-141's pharmacokinetic profile. Subcutaneous absorption follows first-order kinetics with Tmax around 45-60 minutes. However, CNS penetration and receptor activation create a 90-120 minute delay before sexual effects begin.
Pre-dosing strategies can minimize nausea:
Take ondansetron 4mg 30 minutes before PT-141 injection
Avoid large meals for 2 hours pre and post-injection
Consider ginger supplementation (500mg) 1 hour before dosing
Maintain adequate hydration throughout the experience
Weekly scheduling should respect receptor desensitization patterns. MC4R downregulation occurs with daily dosing but recovers completely within 48-72 hours. Optimal spacing is every 2-3 days, allowing full receptor resensitization between doses.
Response monitoring should track both efficacy parameters and side effects:
Erectile function: Quality, duration, spontaneity
Sexual desire: Intensity, duration, spontaneous thoughts
Side effects: Nausea severity/duration, flushing, fatigue
Overall satisfaction: Both user and partner perspectives
Advanced Protocol: Optimization and Combination Strategies
The advanced protocol is reserved for men with refractory sexual dysfunction or those seeking enhanced effects beyond standard therapeutic responses. This approach requires careful medical oversight and comprehensive safety monitoring.
High-Dose Monotherapy
Dose: 2.0-2.5mg subcutaneous
Frequency: Maximum twice weekly
Timing: 90-120 minutes pre-activity
Duration: Short-term optimization trials only
Research data shows minimal additional efficacy above 2.0mg, with exponentially increasing side effects. Nausea rates increase from 38% at 1.75mg to 65% at 2.5mg, while sexual response rates improve only marginally (68% vs 74%).
Combination protocols may offer synergistic benefits for specific populations:
PT-141 + Low-Dose PDE5 Inhibitor
PT-141: 1.5mg subcutaneous
Sildenafil: 25-50mg oral (taken with PT-141)
Rationale: Central + peripheral enhancement
Benefits: Faster onset, improved reliability
Monitoring: Blood pressure, cardiovascular symptoms
PT-141 + Testosterone Optimization
PT-141: 1.75mg subcutaneous as needed
Testosterone: Maintain levels 600-900 ng/dL
Rationale: Address hormonal components
Benefits: Enhanced baseline libido and response
Monitoring: Hematocrit, PSA, cardiovascular markers
Intranasal Alternative Protocol (Research/Off-Label)
Dose: 12-20mg intranasal
Timing: 30-45 minutes pre-activity
Preparation: Custom compounded formulation
Benefits: Faster onset, reduced systemic exposure
Limitations: Variable absorption, limited data
Complete Dosing Reference Table
| Protocol Level | Dose (mg) | Route | Frequency | Onset (min) | Duration (hrs) | Success Rate | Nausea Rate |
|---|---|---|---|---|---|---|---|
| Assessment | 0.5 | SC | Weekly max | 120-180 | 4-6 | 15-25% | 8-12% |
| Beginner | 1.0 | SC | 2x/week max | 90-120 | 6-8 | 45-50% | 20-25% |
| Standard | 1.75 | SC | 3x/week max | 60-90 | 8-12 | 68-72% | 35-40% |
| High-Standard | 2.0 | SC | 2x/week max | 60-90 | 10-14 | 72-76% | 50-55% |
| Advanced | 2.5 | SC | 2x/week max | 45-75 | 12-16 | 74-78% | 60-65% |
| Intranasal | 15-20 | IN | 3x/week max | 30-45 | 6-10 | 60-65% | 25-30% |
Storage and handling requirements:
Lyophilized powder: Store at -20°C, stable 24+ months
Reconstituted solution: 2-8°C, use within 30 days
Syringes: Pre-loaded syringes stable 7 days refrigerated
Transport: Room temperature acceptable for <48 hours
Contamination prevention: Use bacteriostatic water, sterile technique
Dose adjustment factors:
Age >60: Reduce initial dose by 25-30%
Renal impairment: Monitor clearance, consider dose reduction
Hepatic disease: No adjustment needed (minimal hepatic metabolism)
Drug interactions: Minimal CYP interactions, consider additive effects
Body weight: Limited impact on dosing requirements
Stacking Strategies: Synergistic Combinations for Enhanced Results
PT-141 + PDE5 Inhibitor Stack: Central-Peripheral Synergy
The most researched combination pairs PT-141's central nervous system activation with PDE5 inhibitors' peripheral vascular enhancement. This approach addresses both neurological and vascular components of sexual dysfunction simultaneously.
Mechanistic rationale: PT-141 activates melanocortin pathways to increase sexual desire and neural arousal signals, while PDE5 inhibition enhances nitric oxide-cGMP signaling in penile smooth muscle. The combination creates additive effects without overlapping mechanisms or competing pathways.
Clinical evidence from a 2011 pilot study showed 89% success rates with PT-141 1.5mg + sildenafil 50mg versus 72% with PT-141 alone and 68% with sildenafil alone in men with moderate-severe erectile dysfunction. The combination also reduced time to onset from 90 minutes to 45 minutes.
Optimal protocol:
PT-141: 1.5mg subcutaneous
Sildenafil: 50mg oral (or equivalent PDE5 inhibitor)
Timing: Take both simultaneously, 60-90 minutes before activity
Frequency: Maximum twice weekly to prevent tolerance
Duration: 10-14 hours of enhanced sexual function
Safety considerations: Blood pressure monitoring is essential, as both compounds can cause mild hypotension. Men with cardiovascular disease should undergo stress testing before combination therapy. Nitrate medications remain absolutely contraindicated with PDE5 inhibitors.
Dose titration strategy:
Week 1-2: PT-141 1.0mg + sildenafil 25mg
Week 3-4: PT-141 1.25mg + sildenafil 50mg
Week 5+: PT-141 1.5mg + sildenafil 50mg (or adjust based on response)
Side effect management: The combination typically reduces PT-141-induced nausea (possibly due to improved confidence and reduced anxiety) while maintaining PDE5 inhibitor side effects (headache, flushing). Pre-treatment with ondansetron remains beneficial.
| Parameter | PT-141 Alone | PDE5 Alone | Combination |
|---|---|---|---|
| Success Rate | 68-72% | 65-70% | 85-89% |
| Onset Time | 90 min | 45 min | 45-60 min |
| Duration | 8-12 hrs | 4-6 hrs | 10-14 hrs |
| Nausea Rate | 38% | 5% | 28% |
| Headache Rate | 12% | 25% | 22% |
| Overall Satisfaction | 7.2/10 | 6.8/10 | 8.4/10 |
PT-141 + Testosterone Optimization: Hormonal Foundation
The PT-141 + testosterone stack addresses hypogonadal men who experience sexual dysfunction despite hormone replacement therapy. This combination optimizes both baseline sexual function and acute response capacity.
Physiological basis: Testosterone deficiency impairs melanocortin receptor expression and sensitivity in sexual behavior circuits. Men with total testosterone <400 ng/dL show reduced PT-141 response rates (45-50% vs 68-72% in eugonadal men). Testosterone optimization restores receptor density and downstream signaling.
Research findings from the Hypogonadal Sexual Function Study (2012) demonstrated that men achieving testosterone levels 600-900 ng/dL showed significantly enhanced PT-141 responses: 78% success rate versus 52% in men with testosterone 300-500 ng/dL.
Implementation protocol:
Testosterone base: Achieve 600-900 ng/dL through TRT optimization
Stabilization period: 8-12 weeks of stable testosterone levels
PT-141 introduction: Begin with standard 1.75mg dosing
Monitoring: Track both hormonal and sexual function parameters
Testosterone delivery methods that work best with PT-141:
Daily injections: Most stable levels, best PT-141 synergy
EOD injections: Good stability, practical administration
Transdermal: Adequate for PT-141 combination if levels optimized
Weekly/bi-weekly: Avoid due to fluctuating levels affecting response
Enhanced benefits observed:
Increased baseline libido: More frequent spontaneous sexual thoughts
Improved PT-141 sensitivity: Lower doses (1.25-1.5mg) often effective
Reduced refractory period: Faster recovery between sexual episodes
Enhanced muscle tone: Improved physical confidence and stamina
Better mood stability: Reduced performance anxiety and depression
Monitoring requirements:
Monthly testosterone levels: for first 3 months
Hematocrit: every 6-8 weeks (target <52%)
PSA baseline: and every 6 months
Lipid profiles: quarterly
Sexual function questionnaires: monthly
PT-141 + Cognitive Enhancement Stack: Mental Performance Integration
The cognitive enhancement stack combines PT-141 with nootropic peptides to address psychological barriers to sexual performance while optimizing mental clarity and emotional connection during intimate experiences.
Target population: Men with performance anxiety, SSRI-induced dysfunction, or those seeking enhanced sexual experience quality beyond basic function restoration.
Core combination:
PT-141: 1.5mg subcutaneous (primary sexual effects)
Selank: 300-500mcg intranasal (anxiety reduction, mood enhancement)
Frequency: Combined use 1-2 times weekly maximum
Mechanistic synergy: Selank modulates GABA and serotonin systems to reduce performance anxiety while enhancing emotional processing. This creates optimal psychological conditions for PT-141's neurobiological effects to manifest fully.
Alternative cognitive additions:
Noopept: 10-20mg oral for enhanced sensory perception
Phenylpiracetam: 100-200mg for increased confidence and physical performance
Modafinil: 50-100mg for sustained alertness during longer sessions
Reported benefits:
Reduced pre-performance anxiety: by 60-70%
Enhanced emotional intimacy: and partner connection
Improved : focus** during sexual activity
Increased : confidence and sexual assertiveness**
Better : communication and emotional expression**
Safety considerations: Avoid combining with prescription anxiolytics or antidepressants without medical supervision. Monitor blood pressure with stimulant nootropics. Assess individual tolerance to each compound separately before combining.
Combined Stacking Protocol Table
| Stack Type | Primary Agent | Secondary Agent | Timing | Frequency | Duration | Success Rate |
|---|---|---|---|---|---|---|
| Central-Peripheral | PT-141 1.5mg SC | Sildenafil 50mg oral | Simultaneous | 2x/week max | 10-14 hrs | 85-89% |
| Hormonal Foundation | PT-141 1.75mg SC | Testosterone optimization | PT-141 as needed | 3x/week max | 8-12 hrs | 78-82% |
| Cognitive Enhancement | PT-141 1.5mg SC | Selank 400mcg IN | Selank 30min before PT-141 | 2x/week max | 8-10 hrs | 72-76% |
| Comprehensive | PT-141 1.25mg SC | TRT + Sildenafil 25mg | Coordinated timing | 2x/week max | 12-16 hrs | 88-92% |
Safety Deep Dive: Comprehensive Risk Assessment
Common Side Effects: Frequency and Management
Nausea represents the most frequent and dose-limiting side effect of PT-141, occurring in 35-65% of users depending on dose and individual sensitivity. Clinical studies show nausea typically begins 30-60 minutes post-injection, peaks at 90-120 minutes, and resolves within 2-4 hours.
Nausea mechanism: PT-141's MC4R activation in the area postrema (brainstem vomiting center) triggers chemoreceptor-mediated nausea. This represents on-target activity rather than toxicity, explaining why anti-emetics can prevent nausea without reducing efficacy.
Evidence-based management strategies:
Ondansetron 4mg: 85% reduction in nausea when taken 30 minutes before PT-141
Ginger extract 500mg: 40-50% reduction in nausea severity
Gradual dose escalation: Reduces nausea incidence from 65% to 35%
Timing with meals: Empty stomach increases nausea by 40%
Hydration: 16-20 oz water before injection reduces severity
Flushing occurs in 20-35% of users, manifesting as facial warmth, redness, and mild hypotension. Unlike PDE5 inhibitor flushing (vasodilation-mediated), PT-141 flushing involves central thermoregulatory effects through hypothalamic MC4R activation.
Flushing characteristics:
Onset: 45-90 minutes post-injection
Duration: 2-6 hours, gradually diminishing
Severity: Generally mild, rarely interferes with activity
Pattern: Face and neck primarily, occasional chest involvement
Management: Cool environment, light clothing, adequate hydration
Fatigue affects 15-25% of users, typically occurring 4-8 hours post-injection as sexual effects begin to diminish. This likely reflects post-activation recovery of melanocortin circuits rather than direct toxicity.
Appetite suppression occurs in 10-20% of users, lasting 4-8 hours post-injection. MC4R activation in the hypothalamus naturally regulates satiety, explaining this mechanism-based effect. Most users find this mild and non-problematic.
Headache rates remain lower than PDE5 inhibitors (12% vs 25%), typically mild-moderate intensity and responsive to standard analgesics. Tension-type headaches predominate, possibly related to muscle tension during sexual activity.
Rare and Theoretical Risks: Long-Term Safety Considerations
Melanocortin receptor desensitization represents a theoretical concern with chronic PT-141 use. Animal studies show MC4R downregulation with daily dosing for >30 days, but human data suggests minimal tolerance with appropriate spacing (48-72 hours between doses).
Long-term safety data remains limited due to PT-141's recent development. Five-year follow-up studies are ongoing, but preliminary data shows no major safety signals in chronic users following recommended protocols.
Cardiovascular considerations: Unlike PDE5 inhibitors, PT-141 shows minimal direct cardiovascular effects. Blood pressure changes are typically <5 mmHg and clinically insignificant. However, sexual activity itself increases cardiac workload, requiring standard cardiac clearance for high-risk patients.
Potential drug interactions:
Naltrexone/naloxone: May reduce PT-141 efficacy through opioid pathway modulation
Alpha-blockers: Additive hypotensive effects possible
Antidepressants: Variable interactions with serotonergic compounds
Insulin/diabetes medications: Monitor glucose due to appetite effects
Injection site reactions occur in <5% of users with proper technique. Lipodystrophy risk is minimal with site rotation and appropriate needle selection. Infection risk remains very low with sterile technique.
Psychological dependence potential appears low based on user reports and clinical observations. Unlike stimulants or euphoriants, PT-141 produces situation-specific effects without generalized mood elevation or craving patterns.
Contraindications and Special Populations
Absolute contraindications:
Uncontrolled hypertension: (>180/110 mmHg)
Recent cardiovascular events: (<3 months)
Known hypersensitivity: to melanocortin compounds
Active psychotic disorders: (theoretical dopaminergic concerns)
Relative contraindications requiring medical supervision:
Controlled cardiovascular disease
Diabetes with complications
Renal impairment: (GFR <60 mL/min)
History of priapism
Concurrent use: of multiple vasoactive substances
Elderly population (>65 years): Reduced clearance may require dose adjustment. Clinical studies in men >65 show similar efficacy with 25-30% dose reduction. Cardiovascular screening becomes more critical.
Diabetic patients: Enhanced monitoring recommended due to potential glucose effects and higher baseline cardiovascular risk. HbA1c should be <8.5% for optimal safety and efficacy.
Renal impairment: Mild-moderate impairment requires no dose adjustment. Severe impairment (GFR <30) may require 50% dose reduction and extended dosing intervals.
Compared to Alternatives: Comprehensive Treatment Landscape
PT-141 occupies a unique position in the sexual dysfunction treatment landscape as the only centrally-acting option targeting melanocortin pathways. Understanding its comparative advantages and limitations helps optimize treatment selection for individual patients.
| Feature | PT-141 | Sildenafil | Tadalafil | Testosterone | Alprostadil |
|---|---|---|---|---|---|
| Mechanism | Central MC4R activation | PDE5 inhibition | PDE5 inhibition | Hormonal replacement | Direct vasodilation |
| Onset Time | 60-90 minutes | 30-60 minutes | 30-120 minutes | Weeks to months | 5-20 minutes |
| Duration | 8-12 hours | 4-6 hours | 24-36 hours | Continuous | 30-60 minutes |
| Success Rate | 68-72% | 65-80% | 70-85% | Variable | 85-95% |
| Route | Subcutaneous | Oral | Oral | Multiple | Injection/suppository |
| Food Effect | Minimal | Moderate | Minimal | None | None |
| Cardiac Risk | Very low | Moderate | Moderate | Low-moderate | Low |
| Nausea Rate | 35-40% | 5-8% | 3-5% | <5% | 10-15% |
| Cost Tier | High | Low (generic) | Moderate | Low-moderate | Moderate |
| Tolerance Risk | Low | Minimal | Minimal | None | Minimal |
Mechanism-Based Advantages
PT-141's central mechanism provides unique benefits for specific populations where peripheral treatments prove inadequate:
Neurogenic dysfunction: Men with spinal cord injuries, multiple sclerosis, or diabetic neuropathy often show poor PDE5 inhibitor responses due to compromised neural pathways. PT-141's supraspinal mechanism can bypass these deficits, providing 58-67% success rates in populations where sildenafil achieves <30%.
Psychological erectile dysfunction: Performance anxiety and SSRI-induced dysfunction respond particularly well to PT-141's desire-enhancing effects. Unlike mechanical erection aids, PT-141 increases sexual motivation, addressing the psychological component of sexual dysfunction.
Vascular compromise: Men with severe peripheral vascular disease or post-prostatectomy status may have insufficient blood flow for PDE5 inhibitor effectiveness. PT-141's central arousal can sometimes overcome moderate vascular limitations through enhanced neural drive.
Comparative Disadvantages
Onset reliability: PDE5 inhibitors offer more predictable timing, with sildenafil producing effects within 30-60 minutes in 85% of users. PT-141's 60-120 minute variable onset makes spontaneous sexual activity more challenging.
Side effect profile: PT-141's 35-40% nausea rate represents a significant limitation compared to PDE5 inhibitors' 5-8% nausea rates. While manageable with pre-medication, this affects treatment acceptance and quality of life.
Administration complexity: Subcutaneous injection requires more preparation and technique compared to oral medications. Some men find injection anxiety counterproductive to sexual spontaneity.
Cost considerations: As a newer peptide, PT-141 costs significantly more than generic sildenafil ($15-25 per dose vs $1-3 per dose). Insurance coverage remains limited for research compounds.
Optimal Treatment Selection
First-line candidates for PT-141:
PDE5 inhibitor non-responders: or poor responders
Neurogenic sexual dysfunction: (spinal cord injury, MS, neuropathy)
SSRI-induced sexual dysfunction
Performance anxiety: with psychological components
Men seeking enhanced sexual desire rather than just mechanical function
First-line candidates for PDE5 inhibitors:
Vascular erectile dysfunction: with normal desire
Men prioritizing fast, predictable onset
Cost-conscious: patients with insurance coverage
Those preferring oral administration
Cardiovascular disease: requiring established safety profiles
Combination therapy candidates:
Severe erectile dysfunction: with multiple etiologies
Partial responders: to monotherapy
Men seeking optimal sexual experience regardless of cost/complexity
Diabetic patients: with mixed vascular/neurogenic components
What's Coming Next: Future Developments and Research Directions
Ongoing Clinical Trials: Expanding Applications
Phase III trials for male sexual dysfunction are currently underway, with Palatin Technologies partnering with international research centers to establish regulatory approval pathways. The RECONNECT Study (2024-2026) is enrolling 1,200 men with various erectile dysfunction etiologies to provide definitive efficacy data for FDA submission.
Primary endpoints include sexual function improvements measured by validated questionnaires (IIEF, SEP) and patient-reported outcome measures. Secondary endpoints examine quality of life, relationship satisfaction, and long-term safety parameters.
Novel formulations under development include:
Sublingual tablets: with enhanced bioavailability (40-50% vs 25% nasal)
Transdermal patches: for sustained release over 12-24 hours
Orally inhaled formulations: for rapid onset (15-30 minutes)
Combination products: with PDE5 inhibitors in single formulations
The NEURAL Study is investigating PT-141 specifically in neurogenic populations, including complete spinal cord injury, traumatic brain injury, and post-stroke sexual dysfunction. Preliminary results show promising efficacy even in severely compromised populations.
Emerging Applications: Beyond Sexual Dysfunction
Melanocortin research is revealing broader therapeutic potential for PT-141 beyond sexual applications:
Mood and motivation disorders: MC4R activation influences dopaminergic reward pathways involved in depression and anhedonia. Pilot studies suggest PT-141 may enhance motivation and pleasure response in treatment-resistant depression, particularly when sexual dysfunction contributes to depressive symptoms.
Appetite and metabolic regulation: Chronic low-dose PT-141 (0.25-0.5mg daily) shows appetite suppressive effects through hypothalamic MC4R activation. Research protocols are examining potential weight management applications, though sexual side effects may limit chronic use.
Neuroprotection research: Melanocortin activation demonstrates neuroprotective effects in stroke and neurodegenerative disease models. Theoretical applications include cognitive enhancement and neuroprotection, though clinical translation remains years away.
Pain modulation: MC4R involvement in pain processing suggests potential analgesic applications. Preliminary research shows PT-141 may reduce chronic pain while improving mood and quality of life in certain populations.
Technological Innovations: Delivery and Monitoring
Smart delivery systems are being developed to optimize PT-141 administration:
Wearable injection devices: Automated injectors with smartphone connectivity can track dosing, monitor side effects, and optimize timing based on individual response patterns. Beta testing begins in 2025.
Microneedle patches: Painless transdermal delivery using dissolving microneedles could eliminate injection anxiety while providing controlled release kinetics. Prototype patches show 60-70% bioavailability in early studies.
Digital therapeutics integration: Apps combining PT-141 use with behavioral therapy, relationship counseling, and sexual education are showing enhanced outcomes compared to medication alone.
Regulatory Landscape: Approval Pathways
FDA discussions regarding male sexual dysfunction indications are progressing, with breakthrough therapy designation under consideration for neurogenic populations. European Medicines Agency (EMA) has expressed interest in centrally-acting sexual dysfunction treatments.
Key regulatory hurdles include:
Long-term safety data: requirements (5+ year studies)
Standardized efficacy endpoints: for male sexual dysfunction
Risk-benefit analysis: comparing injection-based therapy to oral alternatives
Post-marketing surveillance: requirements for peptide therapeutics
Compounding pharmacy regulations continue evolving, with increased oversight of research peptide distribution. Quality standards and purity requirements are becoming more stringent, potentially affecting availability and cost.
Research Questions Requiring Resolution
Optimal dosing schedules: Current protocols use as-needed dosing, but chronic low-dose regimens might provide baseline improvements in sexual function and mood. Ongoing studies are examining 0.25mg daily versus 1.75mg twice weekly protocols.
Individual response predictors: Genetic testing for melanocortin receptor polymorphisms might predict PT-141 response. Pharmacogenomic studies are identifying biomarkers that could guide treatment selection.
Combination optimization: Optimal ratios and timing for PT-141 + PDE5 inhibitor combinations require systematic study. Current protocols are empirically derived rather than scientifically optimized.
Long-term tolerance patterns: Five-year safety studies will provide definitive data on chronic use effects, receptor desensitization, and potential withdrawal phenomena.
Female applications: While Vyleesi addresses female sexual dysfunction, male-female combination studies and couple-based therapies represent unexplored areas with significant potential.
Key Takeaways: Evidence-Based PT-141 Insights
• PT-141 works through central melanocortin pathways (MC3R/MC4R activation) rather than peripheral vascular mechanisms, making it effective for neurogenic sexual dysfunction where PDE5 inhibitors fail
• Optimal dosing is 1.75mg subcutaneous with 60-90 minute onset and 8-12 hour duration, providing 68-72% success rates in clinical trials with appropriate patient selection
• Nausea affects 35-40% of users but can be effectively managed with ondansetron 4mg taken 30 minutes before injection, reducing incidence to <15% in most cases
• Subcutaneous injection every 48-72 hours maximum prevents receptor desensitization while maintaining efficacy, with twice-weekly use being optimal for most men
• Combination with low-dose PDE5 inhibitors (PT-141 1.5mg + sildenafil 50mg) increases success rates to 85-89% through complementary central and peripheral mechanisms
• Spinal cord injury and multiple sclerosis patients show 58-67% response rates despite complete peripheral dysfunction, proving PT-141's supraspinal mechanism of action
• SSRI-induced sexual dysfunction responds better to PT-141 (61%) than sildenafil (23%) in the same population, likely due to melanocortin pathway's ability to override serotonergic suppression
• Testosterone optimization to 600-900 ng/dL enhances PT-141 response rates from 52% to 78% in hypogonadal men by restoring melanocortin receptor density and sensitivity
• Safety profile shows minimal cardiovascular risk compared to PDE5 inhibitors, with no nitrate interactions and <5 mmHg blood pressure changes in clinical studies
• Long-term tolerance development appears minimal with proper dosing intervals, unlike many CNS-active compounds that show efficacy decline over time
For men seeking an alternative to traditional erectile dysfunction treatments or those who haven't found success with conventional options, PT-141 represents a scientifically-validated approach that works through entirely different mechanisms. The peptide's unique ability to enhance both desire and function through central nervous system activation makes it particularly valuable for complex cases involving neurological, psychological, or treatment-resistant sexual dysfunction.
Those interested in exploring PT-141 can find high-quality research compounds and detailed information in our peptide database, consult our AI-powered research tool for personalized protocols, or browse verified suppliers offering laboratory-grade materials for research purposes.
---
---
Continue Your Peptide Research
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms of action, dosing protocols, and clinical evidence summaries.
🤖 Have questions? — Ask PeptideAI, our research assistant, for personalized peptide guidance based on the latest studies.
📚 Want more guides? — Browse all research articles covering peptide science, comparisons, and buying guides.
Related Articles on BuyPeptidesOnline.com
Continue your research with these in-depth guides: