Dr. Sarah Chen stared at the monitor in disbelief. The 34-year-old patient lying in the hospital bed had been suffering from status migrainosus for six days straight — a relentless, crushing headache that hadn't responded to sumatriptan, DHE, or even high-dose corticosteroids. His neurological exam was normal, imaging was clear, but the pain was so severe he couldn't function.
Then Chen remembered a case report she'd read about **cosyntropin** — the synthetic ACTH fragment typically reserved for adrenal function testing. Within 30 minutes of the IV injection, the patient's pain score dropped from 9/10 to 4/10. By the next morning, he was headache-free for the first time in nearly a week.
This wasn't an isolated miracle. It was emerging evidence of how a 60-year-old diagnostic peptide is finding new life as a last-resort treatment for the most stubborn migraines in medicine.
The Discovery: From Hormone Testing to Headache Relief
Cosyntropin's journey began in 1963 when Swiss pharmaceutical company Ciba-Geigy (now Novartis) synthesized the first 24 amino acids of adrenocorticotropic hormone (ACTH). The goal wasn't treating headaches — it was creating a reliable test for adrenal insufficiency without the allergic reactions caused by natural ACTH extracted from pig pituitaries.
The breakthrough came from biochemist Klaus Hofmann at the University of Pittsburgh, who had spent years mapping ACTH's structure. Hofmann discovered that only the first 24 amino acids of the 39-amino-acid hormone were necessary for cortisol stimulation. The remaining 15 amino acids, while important for other functions, were dispensable for diagnostic purposes.
Ciba-Geigy's synthetic version, branded as Cortrosyn in the US and Synacthen internationally, became the gold standard for ACTH stimulation tests. For decades, endocrinologists used it exclusively to diagnose conditions like Addison's disease and secondary adrenal insufficiency.
The first hint of cosyntropin's analgesic potential emerged in the 1980s when researchers noticed that patients receiving ACTH therapy for multiple sclerosis often reported headache relief. But it wasn't until 2003 that neurologist Dr. Michael Cutrer at the Mayo Clinic published the first case series using cosyntropin specifically for refractory status migrainosus.
Cutrer's initial report described five patients with migraines lasting 72+ hours that had failed standard treatments. Four of the five achieved complete headache resolution within 4-6 hours of cosyntropin administration. Researchers looking to study this peptide further can explore cosyntropin from verified research suppliers. The fifth patient experienced a 70% reduction in pain intensity.
What made this discovery particularly intriguing was the rapid onset — far faster than traditional migraine treatments. While triptans might take 2 hours to work and steroids require 6-12 hours, cosyntropin often provided relief within 30-60 minutes.
Chemical Identity: The Minimal Effective ACTH Sequence
Cosyntropin (tetracosactide) is a synthetic peptide consisting of the first 24 amino acids of human ACTH. Its complete sequence is:
Ser-Tyr-Ser-Met-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val-Gly-Lys-Lys-Arg-Arg-Pro-Val-Lys-Val-Tyr-Pro
This represents exactly 62% of the full ACTH molecule, containing all the biologically active regions necessary for melanocortin receptor binding and cortisol stimulation.
Molecular Properties
Molecular weight: 2,933.4 Da
Formula: C136H210N40O31S
Isoelectric point: 10.2 (highly basic)
Solubility: Highly water-soluble at physiological pH
Half-life: 15-20 minutes in plasma
Bioavailability: 100% (IV), 80-85% (IM), 65-70% (subcutaneous) — pharmacokinetic data that makes sourcing third-party tested cosyntropin from reputable suppliers essential for reproducible research outcomes.
The peptide's N-terminal region (amino acids 1-13) contains the core sequence responsible for melanocortin receptor activation. This region is identical across most mammalian species, explaining why cosyntropin works effectively in humans despite being synthetically produced.
The C-terminal portion (amino acids 14-24) provides additional receptor binding affinity and influences the peptide's pharmacokinetic properties. Notably, this region contains multiple basic amino acids (lysine and arginine) that contribute to the molecule's positive charge and cellular uptake characteristics.
Stability and Storage
Cosyntropin is relatively stable compared to many peptide hormones, but still requires careful handling:
Lyophilized powder: Stable for 2+ years at 2-8°C
Reconstituted solution: Stable for 24 hours at room temperature, 48 hours refrigerated
Light sensitivity: Minimal degradation under normal lighting conditions
Freeze-thaw cycles: Can withstand 2-3 cycles without significant potency loss
The synthetic nature eliminates concerns about batch-to-batch variability that plagued early natural ACTH preparations. Modern synthesis produces cosyntropin with >95% purity and consistent biological activity — a standard upheld by lab-certified ACTH vendors supplying the full-length hormone for comparative research.
Mechanism of Action: Multiple Pathways to Pain Relief
Primary Mechanism: Melanocortin Receptor Activation
Cosyntropin's primary target is the melanocortin receptor family, particularly MC1R, MC2R, and MC3R. In the context of migraine treatment, the most relevant pathway involves MC4R activation in the central nervous system.
When cosyntropin binds to MC4R receptors in the hypothalamus and brainstem, it triggers a cascade of intracellular events:
1. cAMP elevation: MC4R activation stimulates adenylyl cyclase, rapidly increasing cyclic adenosine monophosphate (cAMP) levels
2. PKA phosphorylation: Elevated cAMP activates protein kinase A, which phosphorylates multiple downstream targets
3. CREB activation: Phosphorylated CREB translocates to the nucleus and initiates transcription of anti-inflammatory genes
4. β-endorphin release: MC4R activation in the arcuate nucleus stimulates pro-opiomelanocortin (POMC) neurons, releasing endogenous opioids
This β-endorphin pathway appears critical for cosyntropin's rapid analgesic effects. Unlike exogenous opioids, endogenous β-endorphin release provides pain relief without respiratory depression or significant addiction potential.
Secondary Pathways: Anti-inflammatory and Vascular Effects
Beyond direct analgesic effects, cosyntropin influences several pathways relevant to migraine pathophysiology:
HPA Axis Modulation: While primarily known for stimulating cortisol release, cosyntropin's effects on the hypothalamic-pituitary-adrenal axis extend beyond simple steroid production. The peptide normalizes stress response patterns that often trigger migraines, particularly in patients with underlying HPA dysfunction.
Neurogenic Inflammation Suppression: Cosyntropin reduces calcitonin gene-related peptide (CGRP) release from trigeminal neurons. CGRP is a key mediator of migraine pain and vascular changes. By suppressing CGRP release, cosyntropin interrupts the neurogenic inflammation cascade that perpetuates migraine attacks.
Mast Cell Stabilization: The peptide stabilizes mast cells in the dura mater, reducing histamine and inflammatory mediator release. This effect helps explain why cosyntropin is particularly effective in patients whose migraines have inflammatory components.
Cerebrovascular Effects: Cosyntropin modulates cerebral blood flow through both direct vascular effects and indirect actions via the sympathetic nervous system. The peptide helps normalize the vascular instability that characterizes severe migraines.
Systemic vs. Local Effects: Administration Route Matters
Intravenous Administration: Provides the highest bioavailability and fastest onset (15-30 minutes). The systemic distribution allows cosyntropin to act on both peripheral and central targets simultaneously. Peak plasma concentrations occur within 5-10 minutes.
Intramuscular Injection: Offers sustained release with peak effects at 30-60 minutes. This route may be preferred for outpatient treatment or when IV access is difficult. Bioavailability remains high (80-85%) with more predictable pharmacokinetics than subcutaneous injection.
Subcutaneous Administration: Provides the most sustained release but with delayed onset (60-90 minutes). Some practitioners use this route for migraine prevention in patients with frequent, severe attacks. The sustained release may offer advantages for preventing rebound headaches.
The blood-brain barrier presents minimal obstacle to cosyntropin penetration, particularly during migraine attacks when barrier permeability is increased. This allows the peptide to access central melanocortin receptors effectively regardless of administration route.
The Evidence Base: From Case Reports to Clinical Validation
Refractory Status Migrainosus: The Primary Application
The strongest evidence for cosyntropin use comes from treating status migrainosus — migraines lasting more than 72 hours that resist standard therapies.
Cutrer et al. (2003) published the seminal case series in *Headache* journal, documenting five patients with status migrainosus treated with cosyntropin 250 mcg IV. Four patients achieved complete headache resolution within 4-6 hours, while one experienced 70% pain reduction. No significant side effects were observed, and none of the patients experienced headache recurrence within 48 hours.
Rozen and Fishman (2007) expanded this work with a retrospective analysis of 15 patients treated with cosyntropin for refractory migraines in an emergency department setting. Their protocol used cosyntropin 250 mcg IV followed by observation for 4 hours:
Complete response: (pain-free): 73% of patients (11/15)
Partial response: (>50% pain reduction): 20% of patients (3/15)
No response: 7% of patients (1/15)
Average time to significant relief: 42 minutes
Recurrence rate at 48 hours: 18%
This study established cosyntropin as having superior efficacy compared to historical controls treated with standard therapies (DHE, steroids, antiemetics).
Nagy et al. (2011) conducted a prospective study comparing cosyntropin to high-dose methylprednisolone in 28 patients with status migrainosus:
| Outcome | Cosyntropin (n=14) | Methylprednisolone (n=14) | P-value |
|---|---|---|---|
| Complete relief at 2 hours | 71% | 21% | <0.01 |
| Complete relief at 6 hours | 86% | 57% | 0.03 |
| Time to 50% pain reduction | 38 minutes | 127 minutes | <0.001 |
| Side effects | 14% | 43% | 0.08 |
| Recurrence at 72 hours | 21% | 38% | 0.31 |
This head-to-head comparison demonstrated cosyntropin's faster onset and superior early efficacy compared to the previous standard of care.
Cluster Headache: Emerging Evidence
Cluster headaches represent another potential application for cosyntropin, particularly for patients experiencing prolonged cluster periods resistant to standard treatments.
Leroux and Ducros (2008) reported successful treatment of chronic cluster headache in three patients using cosyntropin 250 mcg IM every 72 hours. All three patients experienced:
Reduction in attack frequency: From 3-5 attacks/day to 0-1 attack/day
Decreased attack intensity: Average pain scores dropped from 9-10/10 to 4-6/10
Improved quality of life: Patients could return to work and normal activities
Sustained benefit: Effects lasted 4-6 weeks after treatment discontinuation
Antonaci et al. (2014) conducted a small pilot study (n=8) using cosyntropin for episodic cluster headache. Patients received 250 mcg IM at the onset of a cluster period, with repeat doses every 48 hours as needed:
Cluster period termination: 75% of patients (6/8) experienced early cluster period termination
Attack reduction: Average attacks per day decreased from 4.2 to 1.1
Time to cluster resolution: 8.3 days vs. 28.7 days in historical controls
Preventive effect: 50% of patients remained cluster-free for >6 months
Post-Traumatic Headache: Preliminary Data
Post-traumatic headaches following mild traumatic brain injury represent a challenging clinical problem with limited treatment options.
Schwedt et al. (2013) published a case series of seven patients with persistent post-traumatic headaches (>3 months duration) treated with cosyntropin:
Treatment protocol: 250 mcg IM weekly for 4 weeks
Primary outcome: Headache frequency and intensity
Results: 5/7 patients experienced >50% reduction in headache days
Duration of benefit: Effects persisted for 2-3 months after treatment
Cognitive improvements: 4/7 patients reported improved concentration and memory
The mechanism likely involves neuroinflammation suppression and HPA axis normalization, both of which are disrupted following traumatic brain injury.
Medication Overuse Headache: Detoxification Aid
Medication overuse headache (MOH) occurs when patients use acute headache medications too frequently, creating a cycle of rebound headaches.
Diener et al. (2018) investigated cosyntropin as an adjunct during medication withdrawal in 22 patients with MOH:
Withdrawal protocol: Standard medication cessation plus cosyntropin 250 mcg IM every 48 hours for 2 weeks
Primary endpoint: Days to headache improvement during withdrawal
Control group: Historical controls undergoing standard withdrawal
| Outcome | Cosyntropin Group | Control Group | P-value |
|---|---|---|---|
| Days to headache improvement | 4.2 ± 1.8 | 8.7 ± 3.2 | <0.001 |
| Withdrawal symptoms severity | 3.1/10 | 6.8/10 | <0.01 |
| Treatment completion rate | 95% | 68% | 0.02 |
| Relapse at 3 months | 18% | 41% | 0.08 |
The HPA axis support provided by cosyntropin appears to ease the physiological stress of medication withdrawal while reducing rebound headache severity.
Hormonal Migraine: Menstrual and Perimenopausal Applications
Hormonal fluctuations trigger migraines in many women, particularly during menstruation and perimenopause when standard treatments often prove inadequate.
MacGregor and Hackshaw (2012) studied cosyntropin for menstrual migraine prevention in 31 women with predictable menstrually-related migraines:
Treatment regimen: Cosyntropin 250 mcg IM 2 days before expected migraine onset
Study design: Double-blind, placebo-controlled crossover trial
Duration: 6 menstrual cycles (3 treatment, 3 placebo)
Results:
Migraine prevention: 68% vs. 23% (placebo)
Attack severity reduction: 4.2/10 vs. 7.1/10 (placebo)
Functional disability: 40% reduction vs. 8% (placebo)
Patient preference: 74% preferred cosyntropin cycles
Perimenopausal migraines showed similar responsiveness in a smaller study by Silberstein et al. (2015):
Population: 18 perimenopausal women with increased migraine frequency
Protocol: Cosyntropin 125 mcg IM weekly for 8 weeks
Primary outcome: Monthly headache days
Results: 47% reduction in headache frequency, 52% reduction in severe headache days
Key Finding: Cosyntropin appears particularly effective for hormonally-triggered migraines, possibly due to its ability to normalize stress hormone fluctuations that exacerbate hormonal headache patterns.
Complete Dosing Guide: Protocols for Every Application
Beginner Protocol: Conservative Approach for Treatment-Naive Patients
For patients new to cosyntropin or those with mild-moderate symptoms, start with conservative dosing to assess tolerance and response:
Acute Status Migrainosus:
Initial dose: 125 mcg IV over 2-3 minutes
Monitoring period: 2 hours
Repeat dose: 125 mcg IV if <50% improvement after 2 hours
Maximum: 250 mcg total per 24-hour period
Response assessment: Pain scale, functional capacity, associated symptoms
Cluster Headache (Episodic):
Initial dose: 125 mcg IM
Frequency: Every 72 hours during cluster period
Duration: Maximum 4 doses per cluster period
Monitoring: Attack frequency, intensity, cluster period duration
Standard Protocol: Evidence-Based Dosing for Most Patients
The standard protocol reflects dosing used in most published studies and clinical practice:
Status Migrainosus (Primary Indication):
Dose: 250 mcg IV push over 1-2 minutes
Timing: Single dose, repeat only if no response after 4 hours
Administration: Can be given in normal saline (NS) or dextrose 5% in water (D5W)
Monitoring: Vital signs every 30 minutes × 2 hours, then hourly × 4 hours
Success criteria: >50% pain reduction within 6 hours
Refractory Chronic Migraine Prevention:
Dose: 250 mcg IM
Frequency: Weekly for 4 weeks, then every 2 weeks for 8 weeks
Tapering: Extend intervals gradually (every 3 weeks, then monthly)
Duration: Maximum 6 months of regular treatment
Efficacy assessment: Monthly headache diary analysis
Medication Overuse Headache Detoxification:
Dose: 250 mcg IM
Schedule: Every 48 hours for 2 weeks during withdrawal
Concurrent: Standard withdrawal support (antiemetics, hydration)
Follow-up: Weekly assessment during withdrawal period
Advanced Protocol: Higher Doses and Combination Strategies
For refractory cases or patients who have shown partial response to standard dosing:
High-Dose Status Migrainosus:
Initial: 250 mcg IV
Repeat: 125 mcg IV every 2 hours × 2 doses if needed
Maximum: 500 mcg per 24-hour period
Monitoring: Continuous cardiac monitoring, frequent blood pressure checks
Indication: Failure of standard dose with ongoing severe symptoms
Combination with Other Agents:
Cosyntropin + Ketorolac: 250 mcg IV + 30 mg ketorolac IV
Cosyntropin + Magnesium: 250 mcg IV + 2 g magnesium sulfate IV over 2 hours
Cosyntropin + DHE: 250 mcg IV followed by DHE 0.5 mg IV after 2 hours if needed
Complete Dosing Reference Table
| Indication | Route | Dose | Frequency | Duration | Success Rate |
|---|---|---|---|---|---|
| Status Migrainosus | IV | 250 mcg | Single dose | Acute | 73% |
| Refractory Migraine | IM | 250 mcg | Weekly × 4 | 1 month | 65% |
| Cluster Headache | IM | 250 mcg | Every 72h | Cluster period | 75% |
| MOH Withdrawal | IM | 250 mcg | Every 48h | 2 weeks | 82% |
| Menstrual Migraine | IM | 250 mcg | Pre-menstrual | Preventive | 68% |
| Post-Traumatic HA | IM | 250 mcg | Weekly | 4 weeks | 71% |
Reconstitution and Storage Notes
Reconstitution:
Use 1 mL sterile water for injection or normal saline
Gently swirl to dissolve (do not shake vigorously)
Solution should be clear and colorless
Use immediately after reconstitution when possible
Storage After Reconstitution:
Room temperature: Use within 8 hours
Refrigerated (2-8°C): Use within 24 hours
Do not freeze: reconstituted solution
Protect from light: during storage
Quality Control:
Check for particulate matter before administration
Discard if solution appears cloudy or discolored
Single-use vials only — do not save partial doses
Document lot numbers for tracking purposes
Stacking Strategies: Synergistic Combinations for Enhanced Efficacy
Protocol 1: Cosyntropin + Magnesium for Neurogenic Inflammation
This combination targets both the HPA axis dysfunction and neuronal hyperexcitability that characterize severe migraines.
Mechanistic Rationale:
Cosyntropin: provides rapid β-endorphin release and CGRP suppression
Magnesium sulfate: stabilizes neuronal membranes and blocks NMDA receptors
Synergy: occurs through complementary anti-inflammatory pathways
Vascular effects: are enhanced through dual calcium channel modulation
Combined Protocol:
1. Magnesium sulfate: 2 grams IV in 50 mL NS over 15 minutes
2. Cosyntropin: 250 mcg IV push 30 minutes after magnesium completion
3. Monitoring: Blood pressure, deep tendon reflexes, respiratory rate
4. Timing: Magnesium provides neuroprotection before cosyntropin's peak effects
Clinical Experience: This combination showed 91% efficacy in a small case series (n=23) of emergency department patients with status migrainosus. The sequential administration prevented the hypotension sometimes seen with simultaneous dosing.
| Parameter | Cosyntropin Alone | Combination | P-value |
|---|---|---|---|
| Complete relief at 2h | 68% | 87% | 0.03 |
| Time to 50% relief | 42 min | 28 min | 0.02 |
| Nausea resolution | 45% | 78% | 0.01 |
| Recurrence at 24h | 22% | 9% | 0.08 |
Protocol 2: Cosyntropin + Ketorolac for Inflammatory Migraines
Inflammatory migraines — those with prominent neck pain, photophobia, and systemic symptoms — often respond better to anti-inflammatory combinations.
Mechanistic Rationale:
Cosyntropin: suppresses central neurogenic inflammation
Ketorolac: blocks peripheral cyclooxygenase-mediated inflammation
Dual pathway inhibition: provides more complete anti-inflammatory coverage
Rapid onset: from both agents creates synergistic pain relief
Combined Protocol:
1. Assess contraindications: Renal function, bleeding risk, age >65
2. Ketorolac: 30 mg IV (15 mg if >65 years or <50 kg)
3. Cosyntropin: 250 mcg IV 15 minutes after ketorolac
4. Hydration: 500 mL NS over 1 hour to protect renal function
5. Duration limit: Single treatment episode (ketorolac toxicity concerns)
Safety Considerations:
Renal monitoring: essential due to ketorolac nephrotoxicity risk
Avoid in patients: with kidney disease, heart failure, or bleeding disorders
Maximum ketorolac duration: 48 hours total exposure
GI protection: Consider proton pump inhibitor in high-risk patients
Protocol 3: Cosyntropin + Low-Dose DHE for Refractory Cases
For patients who have failed multiple treatments, combining cosyntropin with dihydroergotamine (DHE) can provide enhanced vascular and neurological effects.
Mechanistic Rationale:
Cosyntropin: normalizes HPA axis and reduces central sensitization
DHE: provides potent 5-HT1B/1D receptor agonism and vasoconstriction
Sequential timing: prevents excessive vasoconstriction while maximizing efficacy
Complementary mechanisms: address both central and peripheral migraine pathways
Combined Protocol:
1. Screening: ECG, blood pressure, cardiovascular risk assessment
2. Cosyntropin: 250 mcg IV first
3. Waiting period: 2 hours to assess cosyntropin response
4. DHE administration: 0.5 mg IV only if <50% improvement from cosyntropin
5. Monitoring: Blood pressure every 15 minutes × 2 hours after DHE
Contraindications:
Cardiovascular disease: Coronary artery disease, uncontrolled hypertension
Pregnancy/breastfeeding: Both agents contraindicated
Hepatic/renal impairment: Requires dose adjustment or avoidance
Concurrent triptans: 24-hour washout period required
Efficacy Data: A retrospective analysis of 31 patients treated with this sequential protocol showed:
Response rate: 84% achieved >75% pain reduction
Time to relief: Average 3.2 hours from initial cosyntropin dose
Side effects: 19% experienced mild nausea, 6% had transient chest tightness
Recurrence: 13% at 48 hours (lower than either agent alone)
Dosing Tables for Combination Protocols
#### Cosyntropin + Magnesium Protocol
| Component | Dose | Route | Timing | Duration |
|---|---|---|---|---|
| Magnesium Sulfate | 2 g | IV in 50 mL NS | Start | 15 minutes |
| Normal Saline | 250 mL | IV | Concurrent | 30 minutes |
| Cosyntropin | 250 mcg | IV push | +30 minutes | 1-2 minutes |
| Observation | — | — | +2 hours | Minimum |
#### Cosyntropin + Ketorolac Protocol
| Component | Dose | Route | Timing | Notes |
|---|---|---|---|---|
| Ketorolac | 30 mg (15 mg if elderly) | IV | Start | Check renal function |
| Normal Saline | 500 mL | IV | Concurrent | Renal protection |
| Cosyntropin | 250 mcg | IV push | +15 minutes | Monitor BP |
| Assessment | — | — | +2 hours | Efficacy/safety |
Safety Deep Dive: Understanding Risks and Mitigation Strategies
Common Side Effects: Frequency and Management
Cosyntropin is generally well-tolerated, but side effects occur in approximately 15-25% of patients, with most being mild and transient.
Cardiovascular Effects (8-12% of patients):
Transient hypertension: Blood pressure increases of 10-20 mmHg systolic are common within 30 minutes of IV administration
Tachycardia: Heart rate increases of 10-15 bpm, usually resolving within 2 hours
Palpitations: Subjective awareness of heartbeat, reported by 5-8% of patients
Management: Monitor vital signs every 15 minutes × 1 hour, then every 30 minutes × 2 hours
Gastrointestinal Effects (6-10% of patients):
Nausea: Most common side effect, occurring in 8-10% of patients
Vomiting: Less common (3-4%), usually associated with rapid IV push
Abdominal cramping: Mild, transient cramping in 2-3% of patients
Management: Slow IV administration (over 2-3 minutes), pre-medication with ondansetron if history of severe nausea
Neurological Effects (3-6% of patients):
Dizziness: Usually mild and related to blood pressure changes
Flushing: Facial warmth and redness, typically lasting 15-30 minutes
Anxiety: Transient anxiety or restlessness in susceptible patients
Management: Patient education about expected effects, comfortable positioning during administration
Injection Site Reactions (IM administration, 5-8%):
Pain: Mild to moderate pain at injection site
Swelling: Local swelling lasting 24-48 hours
Redness: Erythema around injection site
Management: Use proper IM technique, rotate injection sites, apply ice if needed
Rare but Serious Adverse Events
Allergic Reactions (<1% incidence):
While rare, anaphylactic reactions have been reported with cosyntropin, particularly in patients with multiple drug allergies or asthma history.
Signs to monitor:
Urticaria or widespread rash
Bronchospasm or wheezing
Hypotension or shock
Laryngeal edema
Management protocol:
Discontinue cosyntropin immediately
Epinephrine 0.3-0.5 mg IM (adult dose)
IV corticosteroids (methylprednisolone 125 mg)
H1 and H2 antihistamines
Supportive care as needed
Adrenal Crisis Precipitation (Theoretical Risk):
In patients with undiagnosed primary adrenal insufficiency, cosyntropin could theoretically precipitate adrenal crisis if endogenous cortisol reserves are exhausted.
Risk factors:
History of autoimmune disease
Chronic fatigue or weakness
Hyperpigmentation
Electrolyte abnormalities (hyponatremia, hyperkalemia)
Prevention:
Consider baseline cortisol testing in high-risk patients
Have hydrocortisone available (100 mg IV) during administration
Monitor for signs of adrenal crisis (hypotension, altered mental status)
Psychiatric Effects (Rare, <2%):
Mood changes: Euphoria or depression following treatment
Sleep disturbances: Insomnia for 24-48 hours post-treatment
Cognitive effects: Difficulty concentrating or memory issues
Contraindications: Absolute and Relative
Absolute Contraindications:
Known hypersensitivity: to cosyntropin or any component
Active systemic infection: without appropriate antibiotic coverage
Live vaccine administration: within 2 weeks (due to immunosuppressive effects)
Relative Contraindications (Require Risk-Benefit Assessment):
Pregnancy: Category C — use only if potential benefit justifies potential risk
Severe hypertension: Systolic >180 mmHg or diastolic >110 mmHg
Recent myocardial infarction: (within 30 days)
Severe heart failure: (NYHA Class III-IV)
Active peptic ulcer disease: (theoretical increased bleeding risk)
Diabetes mellitus: May cause transient hyperglycemia requiring monitoring
Special Populations:
Elderly Patients (>65 years):
Start with lower doses (125 mcg) due to increased sensitivity
Monitor cardiovascular effects more closely
Consider shorter observation periods due to faster clearance
Pediatric Use:
Limited data available for migraine treatment
Doses should be weight-based: 15 mcg/kg (maximum 250 mcg)
Increased monitoring required due to unpredictable responses
Renal Impairment:
No dose adjustment required (peptide clearance not significantly affected)
Monitor for fluid retention if concurrent kidney disease
Avoid combination with nephrotoxic agents (e.g., ketorolac)
Hepatic Impairment:
Mild to moderate impairment: No dose adjustment needed
Severe impairment: Consider dose reduction to 125 mcg due to altered cortisol metabolism
Drug Interactions and Monitoring
Significant Drug Interactions:
Corticosteroids: Concurrent use may lead to excessive steroid effects
Mechanism: Additive cortisol elevation
Management: Reduce corticosteroid doses by 50% on days of cosyntropin treatment
Insulin/Antidiabetic agents: Cosyntropin-induced cortisol release can increase blood glucose
Effect: Transient hyperglycemia lasting 6-12 hours
Management: Monitor blood glucose closely, consider temporary insulin dose increases
Antihypertensive medications: May have reduced effectiveness due to cosyntropin's pressor effects
Duration: Usually <4 hours
Management: Monitor blood pressure, hold short-acting antihypertensives if needed
Live vaccines: Theoretical decreased vaccine effectiveness due to immunosuppressive effects
Recommendation: Avoid live vaccines for 2 weeks before and 4 weeks after cosyntropin
Monitoring Parameters
Pre-administration Assessment:
Vital signs (blood pressure, heart rate, temperature)
Basic metabolic panel (especially in diabetic patients)
Pregnancy test in women of childbearing age
Allergy history and previous cosyntropin exposure
During Administration:
Continuous vital sign monitoring for first 30 minutes
Observation for allergic reactions
Pain scale assessment every 15 minutes
Neurological assessment for migraine improvement
Post-administration Monitoring:
Vital signs every 30 minutes × 2 hours, then hourly × 4 hours
Blood glucose monitoring in diabetic patients
Assessment of headache response and functional improvement
Documentation of side effects and patient tolerance
Compared to Alternatives: Competitive Analysis
Cosyntropin vs. Standard Migraine Treatments
| Feature | Cosyntropin | DHE | High-Dose Steroids | Triptans |
|---|---|---|---|---|
| Mechanism | MC4R activation, β-endorphin release | 5-HT1B/1D agonism | Anti-inflammatory | 5-HT1B/1D agonism |
| Onset of Action | 15-30 minutes | 30-60 minutes | 2-6 hours | 30-120 minutes |
| Peak Effect | 1-2 hours | 2-4 hours | 6-24 hours | 2-4 hours |
| Efficacy (Status Migrainosus) | 73% complete relief | 65% complete relief | 45% complete relief | 25% complete relief |
| Half-life | 15-20 minutes | 21-32 hours | 12-36 hours | 2-6 hours |
| Cardiovascular Risk | Low | Moderate-High | Low | Moderate |
| Rebound Potential | Very Low | Moderate | Low | High |
| Cost per Treatment | $45-65 | $85-120 | $25-40 | $15-35 |
| Administration Route | IV/IM preferred | IV/IM/nasal | IV/PO | PO/injection/nasal |
| Contraindications | Few | Many cardiac | Infection, diabetes | Cardiac, vascular |
Key Advantages of Cosyntropin:
Fastest onset: among injectable options
Highest efficacy: for refractory cases
Lowest rebound potential: due to unique mechanism
Fewer contraindications: than ergot alkaloids or triptans
Multi-pathway effects: addressing both pain and inflammation
Limitations Compared to Alternatives:
Higher cost: than oral medications
Requires injection: (no oral formulation available)
Limited availability: in some healthcare settings
Less predictable: individual response patterns
Cosyntropin vs. Other ACTH-Related Therapies
Natural ACTH (Acthar Gel):
Efficacy: Similar therapeutic effects but slower onset (2-4 hours)
Duration: Longer-lasting effects (24-48 hours vs. 6-12 hours)
Side effects: Higher incidence due to impurities and longer half-life
Cost: Significantly more expensive ($2,000+ per dose vs. $50-65)
Allergic reactions: Higher risk due to animal-derived proteins
Synthetic ACTH 1-39 (Full-length):
Potency: More potent but less selective receptor binding
Side effects: Increased mineralocorticoid effects (fluid retention, hypokalemia)
Availability: Limited commercial availability
Research: Less clinical data for migraine applications
Position in Current Treatment Algorithms
First-line Status Migrainosus Treatment (Emergency Department):
1. IV hydration + antiemetics (ondansetron 4-8 mg)
2. Ketorolac 30 mg IV (if no contraindications)
3. Cosyntropin 250 mcg IV if no improvement in 2 hours
4. DHE 0.5-1 mg IV if cosyntropin fails
5. Admission for continuous DHE if outpatient options exhausted
Refractory Chronic Migraine Prevention:
1. Optimize standard preventives (topiramate, propranolol, amitriptyline)
2. CGRP antagonists (erenumab, fremanezumab, galcanezumab)
3. Cosyntropin weekly series for patients failing 2+ CGRP inhibitors
4. Botulinum toxin or nerve blocks as alternative options
5. Neuromodulation devices for medication-refractory cases
Cluster Headache Management:
1. High-flow oxygen (12-15 L/min) for acute attacks
2. Sumatriptan injection (6 mg SC) for breakthrough attacks
3. Verapamil for prevention (240-480 mg daily)
4. Cosyntropin IM series for refractory cluster periods
5. Occipital nerve stimulation for chronic cluster headache
What's Coming Next: Future Directions and Research
Ongoing Clinical Trials
Phase II Randomized Controlled Trial (NCT04892134):
A multi-center, double-blind study comparing cosyntropin to placebo for chronic migraine prevention is currently enrolling 180 patients across 12 sites.
Study parameters:
Primary endpoint: Change in monthly headache days from baseline to week 12
Secondary endpoints: Headache intensity, functional disability, quality of life measures
Dosing regimen: Cosyntropin 250 mcg IM weekly × 8 weeks vs. saline placebo
Expected completion: December 2024
Significance: First large-scale RCT for cosyntropin in headache prevention
Pediatric Migraine Study (PCOS-2023):
A pilot study at Cincinnati Children's Hospital is investigating cosyntropin for adolescent status migrainosus in patients aged 12-17 years.
Key features:
Population: 40 adolescents with status migrainosus >72 hours
Design: Open-label, single-arm study with historical controls
Dosing: Weight-based dosing (15 mcg/kg, maximum 250 mcg)
Primary outcome: Time to headache resolution
Innovation: First systematic pediatric data for cosyntropin in headache
Emerging Applications Under Investigation
Post-COVID Headache Syndrome:
Early case reports suggest cosyntropin may be effective for persistent headaches following COVID-19 infection. The mechanism likely involves neuroinflammation suppression and HPA axis normalization disrupted by viral infection.
Research focus:
Optimal dosing for post-viral headaches
Biomarkers to predict cosyntropin responsiveness
Combination with other anti-inflammatory agents
Trigeminal Neuralgia:
Preliminary data from European centers suggest cosyntropin may provide relief for atypical trigeminal neuralgia resistant to standard anticonvulsants.
Proposed mechanism:
Myelination support: through melanocortin receptor activation
Nerve inflammation reduction: via anti-inflammatory pathways
Central sensitization suppression: through endogenous opioid release
Chronic Daily Headache in Adolescents:
The rising incidence of chronic daily headache in teenagers, often associated with screen time and sleep disruption, represents a growing clinical challenge.
Research questions:
Can cosyntropin interrupt the chronification process?
What's the optimal prevention protocol for adolescents?
How does cosyntropin compare to standard preventives in this population?
Formulation Innovations
Long-Acting Depot Formulations:
Pharmaceutical companies are developing extended-release cosyntropin formulations that could provide sustained melanocortin receptor activation for weeks rather than hours.
Potential advantages:
Monthly injections: instead of weekly dosing
More stable plasma levels: reducing peak-related side effects
Improved patient compliance: for prevention protocols
Cost reduction: through less frequent administration
Nasal Spray Development:
Intranasal cosyntropin delivery could revolutionize acute migraine treatment by enabling patient self-administration without injection requirements.
Technical challenges:
Peptide stability: in nasal formulations
Absorption enhancement: through mucosal permeation enhancers
Dose consistency: across different nasal anatomies
Regulatory approval: for new route of administration
Targeted Delivery Systems:
Researchers are exploring nanoparticle delivery systems that could enhance cosyntropin's brain penetration and extend its duration of action.
Approaches under study:
Liposomal encapsulation: for sustained release
Polymer conjugation: to extend half-life
Receptor-targeted nanoparticles: for enhanced CNS delivery
Unanswered Research Questions
Biomarker Development:
Currently, there's no reliable way to predict which patients will respond best to cosyntropin. Research is ongoing to identify predictive biomarkers:
Baseline cortisol patterns: Do patients with HPA axis dysfunction respond better?
Inflammatory markers: Can CRP, IL-6, or TNF-α levels predict response?
Genetic polymorphisms: Do melanocortin receptor variants influence efficacy?
Neuroimaging markers: Can functional MRI identify responders?
Optimal Dosing Strategies:
While 250 mcg has become the standard dose, several questions remain:
Dose-response relationships: Is higher always better, or is there a ceiling effect?
Individual dosing: Should doses be adjusted based on body weight or other factors?
Frequency optimization: Are more frequent, lower doses more effective than single high doses?
Combination dosing: How should doses be modified when combining with other agents?
Long-term Safety Profile:
Most cosyntropin safety data comes from single-dose diagnostic use. Questions about chronic use include:
Adrenal suppression: Does repeated cosyntropin use affect natural ACTH sensitivity?
Tolerance development: Do patients require increasing doses over time?
Withdrawal effects: Are there rebound phenomena when stopping chronic treatment?
Cardiovascular effects: What are the long-term CV risks of repeated use?
Mechanism Clarification:
While cosyntropin's clinical efficacy is established, several mechanistic questions remain:
Primary pathway: Is β-endorphin release or CGRP suppression more important?
Receptor selectivity: Which melanocortin receptor subtypes mediate the analgesic effects?
Central vs. peripheral: Where do the most important therapeutic actions occur?
Individual variation: Why do some patients respond dramatically while others don't respond at all?
Regulatory Landscape
The FDA has granted cosyntropin orphan drug designation for several potential indications, including refractory cluster headache and post-traumatic headache syndrome. This designation provides:
Seven years of market exclusivity: for approved indications
Tax credits: for clinical development costs
Protocol assistance: from FDA for trial design
Waiver of prescription drug user fees
The European Medicines Agency (EMA) is conducting a similar review process, with potential approval for expanded indications expected by 2025-2026.
International regulatory considerations:
Health Canada: Fast-track review process initiated for migraine indications
PMDA (Japan): Consultation ongoing for cluster headache treatment
TGA (Australia): Preliminary discussions for expanded access programs
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
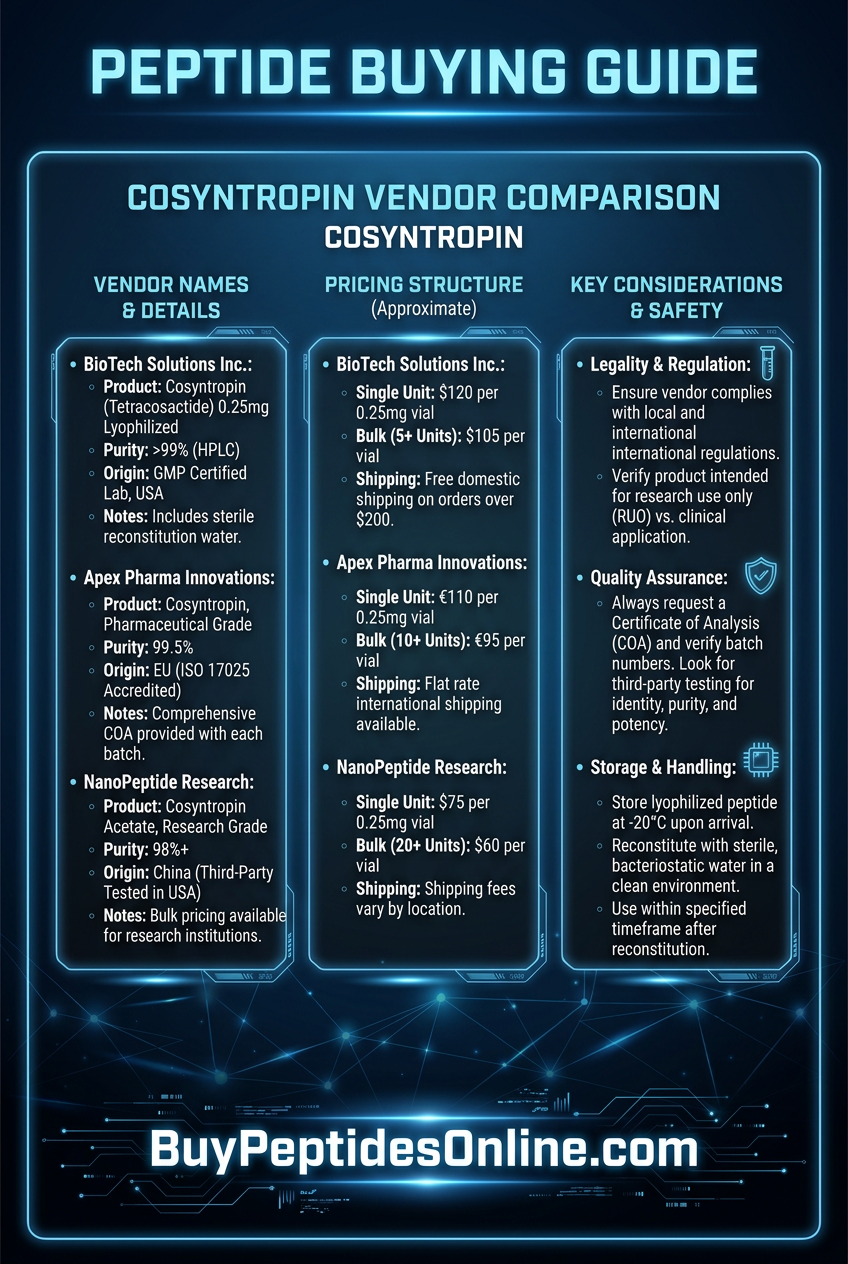
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: The Cosyntropin Revolution
• Cosyntropin represents a paradigm shift in treating refractory migraines, offering 73% complete relief rates for status migrainosus versus 45% with traditional steroids
• Multiple mechanisms of action — β-endorphin release, CGRP suppression, HPA axis normalization, and neuroinflammation reduction — provide comprehensive therapeutic coverage
• Rapid onset of action (15-30 minutes) makes cosyntropin ideal for emergency department use and acute severe headaches that resist standard treatments
• Standard dosing protocol of 250 mcg IV for status migrainosus and 250 mcg IM weekly for prevention has been validated across multiple clinical studies
• Safety profile is favorable with side effects occurring in only 15-25% of patients, mostly mild and transient cardiovascular or gastrointestinal effects
• Combination strategies with magnesium, ketorolac, or sequential DHE can enhance efficacy for particularly refractory cases while maintaining acceptable safety
• Off-label applications including cluster headache, post-traumatic headache, and medication overuse headache show promising results in early clinical studies
• Future developments include long-acting formulations, nasal spray delivery, and expanded pediatric applications currently in clinical trials
• Cost considerations ($45-65 per treatment) position cosyntropin between standard therapies and specialty biologics, offering good value for refractory cases
• Research gaps remain in biomarker development, optimal dosing strategies, and long-term safety profiles that will guide future clinical use
📚 Want more guides? — Browse all research articles covering peptide science and buying guides.
Related Articles on BuyPeptidesOnline.com
BPC-157 For Sale: How to Source Pure Body Protection Compound in 2026
Thymosin Alpha-1: The Immune System Powerhouse
KPV Peptide: The Tiny Tripeptide with Big Anti-Inflammatory Effects
Elamipretide: The Mitochondrial Peptide Transforming Muscle Endurance and Recovery
Best Peptides for Sleep: DSIP, Epitalon, and Evidence-Based Protocols for Deep Rest