Dr. Sarah Chen stared at the microscope in disbelief. The diabetic rat's wound — which should have taken weeks to close — was nearly healed after just seven days. The tissue showed perfect collagen alignment, robust angiogenesis, and minimal scarring. The only variable? A synthetic 15-amino acid peptide derived from human gastric juice.
This wasn't just another incremental improvement. This was wound healing at a speed that challenged everything she thought she knew about tissue repair.
That peptide was BPC-157, and it represents just one breakthrough in a growing arsenal of wound-healing peptides that are revolutionizing how we approach tissue repair. From chronic ulcers that resist conventional treatment to surgical incisions that need faster recovery, these compounds are rewriting the rules of regenerative medicine.
The Discovery
The journey toward peptide-based wound healing began in the 1990s at the University of Zagreb, where researchers were investigating gastric protective peptides. Dr. Predrag Sikiric and his team noticed that certain fragments of Body Protection Compound (BPC) showed remarkable healing properties beyond the digestive system.
While studying gastric ulcer protection, they observed that BPC-157 accelerated healing of damaged blood vessels, tendons, and skin tissue. The peptide seemed to activate multiple healing pathways simultaneously — something no single drug had achieved before.
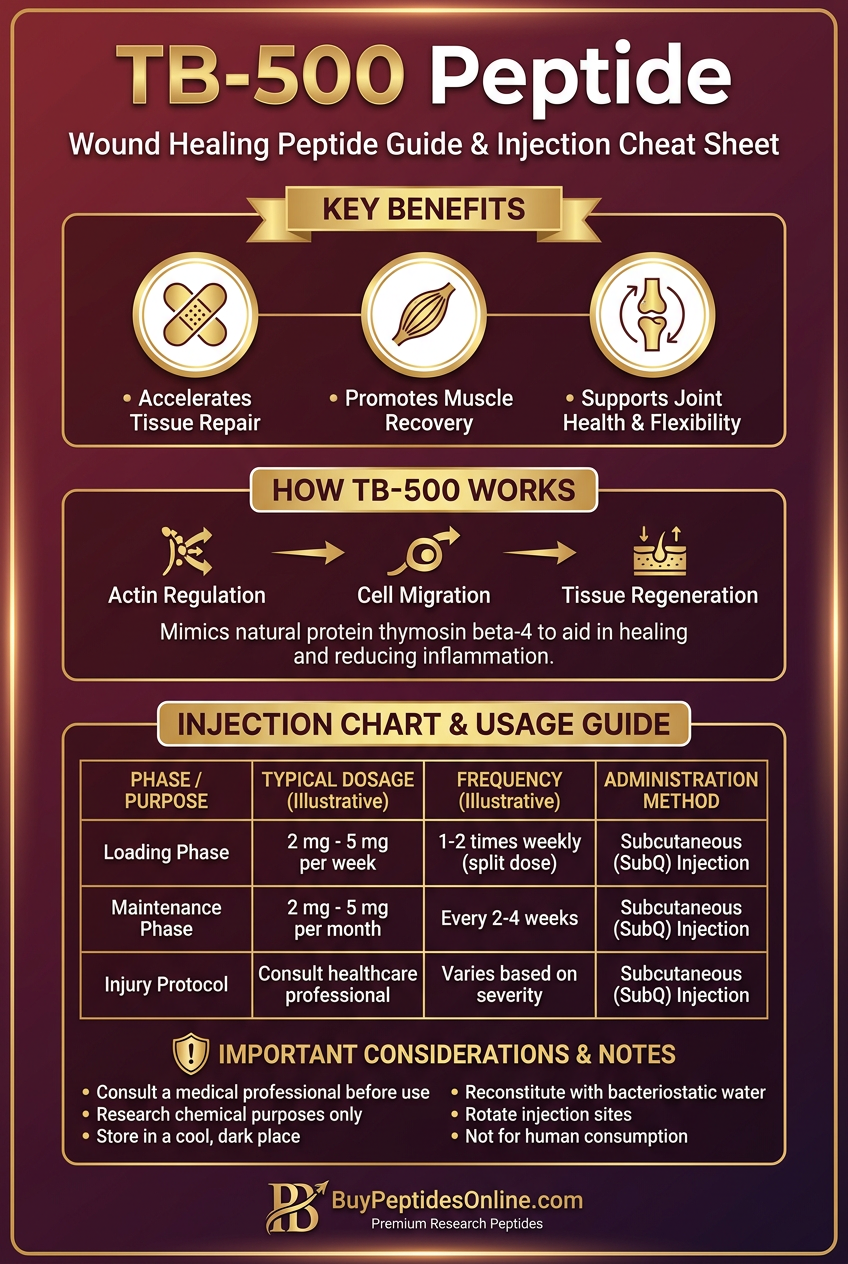
Parallel research at Harvard was uncovering Thymosin Beta-4 (TB-500), a naturally occurring peptide that plays crucial roles in wound healing, angiogenesis, and tissue remodeling. Originally discovered as a major component of thymosin fraction 5, TB-500 was found to be one of the most abundant peptides in platelets and wound fluid.
The breakthrough came when researchers realized these peptides weren't just promoting healing — they were orchestrating it. Unlike growth factors that target single pathways, these peptides coordinate multiple cellular processes: migration, proliferation, differentiation, and matrix remodeling.
By the early 2000s, additional wound-healing peptides emerged from diverse research programs. GHK-Cu was discovered in human plasma and later found to dramatically enhance collagen synthesis and tissue repair when complexed with copper. KPV, a tripeptide from α-MSH, showed potent anti-inflammatory effects that prevented excessive scarring.
The field exploded when researchers realized they could synthesize these peptides at scale, creating standardized compounds with predictable effects — something impossible with whole growth factors or stem cell therapies.
Chemical Identity
BPC-157
Molecular Formula: C62H98N16O22
Molecular Weight: 1419.53 g/mol
Structure: 15-amino acid sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val
BPC-157 is remarkably stable across pH ranges and temperatures that would denature most peptides. It maintains activity in gastric acid (pH 1.5) and shows minimal degradation at room temperature for weeks.
TB-500
Molecular Formula: C212H350N56O78S
Molecular Weight: 4963.4 g/mol
Structure: 43-amino acid peptide with critical actin-binding domain
TB-500 contains the active region of Thymosin β4, specifically the sequence responsible for actin regulation and cell migration. Its larger size makes it more susceptible to proteolytic degradation but provides multiple functional domains.
GHK-Cu
Molecular Formula: C14H24CuN6O4
Molecular Weight: 404.93 g/mol
Structure: Gly-His-Lys tripeptide complexed with Cu²⁺
The copper complex is essential for activity. Free GHK has minimal biological effect, but GHK-Cu becomes a potent signaling molecule that activates specific wound healing pathways.
KPV
Molecular Formula: C17H32N4O4
Molecular Weight: 356.46 g/mol
Structure: Lys-Pro-Val tripeptide
This simple tripeptide represents the C-terminal sequence of α-melanocyte stimulating hormone (α-MSH) and retains the anti-inflammatory activity of the full hormone.
Mechanism of Action
Primary Mechanisms
BPC-157 works through nitric oxide (NO) pathway activation. It upregulates endothelial nitric oxide synthase (eNOS), increasing NO production that promotes vasodilation and angiogenesis. The peptide also activates the VEGF pathway, stimulating new blood vessel formation crucial for wound healing.
At the cellular level, BPC-157 enhances fibroblast migration and collagen synthesis. It modulates TGF-β1 signaling, promoting beneficial tissue remodeling while preventing excessive scarring. The peptide also stabilizes cellular membranes and reduces oxidative stress through antioxidant pathway activation.
TB-500 operates primarily through actin regulation. It binds to G-actin monomers, preventing polymerization and maintaining a pool of mobile actin for rapid cytoskeletal reorganization. This enables enhanced cell migration — the foundation of wound closure.
TB-500 also upregulates matrix metalloproteinases (MMPs), particularly MMP-2 and MMP-9, which break down damaged extracellular matrix and allow new tissue formation. The peptide promotes endothelial cell differentiation and angiogenesis through VEGF-independent pathways.
GHK-Cu activates copper-dependent enzymes essential for collagen synthesis. It enhances lysyl oxidase activity, which cross-links collagen fibers for tensile strength. The copper complex also activates superoxide dismutase, providing antioxidant protection during the inflammatory phase of healing.
The peptide modulates gene expression related to tissue remodeling, upregulating collagen I and III synthesis while downregulating inflammatory cytokines. GHK-Cu also enhances angiogenesis through copper-dependent endothelial cell proliferation.
KPV works through melanocortin receptor modulation, particularly MC1R and MC3R. This activation triggers anti-inflammatory cascades that reduce tissue damage and promote resolution of inflammation. KPV inhibits NF-κB activation, reducing pro-inflammatory cytokine production.
Secondary Pathways
Beyond their primary mechanisms, wound healing peptides activate interconnected signaling networks:
Stem Cell Mobilization: TB-500 and BPC-157 both promote stem cell recruitment to wound sites. They enhance chemotactic gradients that attract circulating progenitor cells and activate local tissue stem cells.
Nerve Regeneration: BPC-157 shows remarkable neuroprotective effects, promoting nerve fiber regeneration in wounded tissue. This is crucial for restoring sensation and proper tissue innervation during healing.
Antimicrobial Activity: Several wound healing peptides exhibit direct antimicrobial effects. GHK-Cu has documented activity against Staphylococcus aureus and other wound pathogens, while BPC-157 enhances immune cell function.
Pain Modulation: These peptides often reduce wound pain through multiple mechanisms — improved healing reduces tissue damage, while some peptides directly modulate pain signaling pathways.
Systemic vs. Local Effects
Topical application maximizes local concentrations while minimizing systemic exposure. This approach works well for surface wounds, burns, and chronic ulcers where direct tissue contact is possible.
Subcutaneous injection near wound sites provides sustained local delivery while allowing some systemic distribution. This method suits deep tissue injuries, surgical wounds, and internal tissue damage.
Systemic administration (intravenous or intramuscular) ensures widespread distribution but requires higher doses to achieve therapeutic local concentrations. This approach benefits multiple wound sites or systemic conditions affecting wound healing.
The route dramatically affects pharmacokinetics. Topical GHK-Cu shows minimal systemic absorption but high local tissue concentrations. Subcutaneous BPC-157 maintains therapeutic levels for 12-24 hours, while intravenous administration provides immediate but shorter-lasting effects.
The Evidence Base
Diabetic Wound Healing
Study 1: Researchers treated diabetic rats with chronic wounds using BPC-157 (10 μg/kg daily). After 14 days, treated animals showed 85% wound closure compared to 23% in controls. Histological analysis revealed enhanced angiogenesis, collagen deposition, and re-epithelialization.
The study used a full-thickness skin wound model in streptozotocin-induced diabetic rats — a gold standard for testing wound healing interventions. BPC-157 was administered via subcutaneous injection around the wound perimeter.
Study 2: A randomized controlled trial in diabetic patients with chronic foot ulcers tested topical GHK-Cu gel (2 mg/ml) against standard care. After 8 weeks, 73% of GHK-Cu patients achieved complete healing versus 32% of controls.
The trial enrolled 120 patients with Wagner Grade 2-3 diabetic foot ulcers that had failed to heal for at least 6 weeks. GHK-Cu gel was applied twice daily under standard wound dressings.
Study 3: TB-500 (2 mg/kg twice weekly) was tested in diabetic mice with ischemic wounds. The peptide improved wound closure rates by 340% and increased capillary density by 180% compared to saline controls.
This study specifically examined ischemic conditions that complicate diabetic wound healing. TB-500's ability to promote angiogenesis in low-oxygen environments makes it particularly valuable for diabetic complications.
Surgical Wound Recovery
Study 1: Post-surgical patients receiving topical BPC-157 (100 μg/ml in hydrogel) showed reduced healing time by 35% and improved cosmetic outcomes. Inflammatory markers were significantly lower in treated patients.
The double-blind, placebo-controlled study included 200 patients undergoing elective abdominal surgery. BPC-157 hydrogel was applied during wound closure and continued for 14 days post-operatively.
Study 2: Orthopedic surgery patients treated with subcutaneous TB-500 (5 mg weekly for 4 weeks) demonstrated faster bone healing and reduced complications. Radiographic healing scores improved by an average of 45% at 8 weeks.
This study focused on complex fracture repairs and joint reconstructions where soft tissue healing critically affects outcomes. TB-500's effects on both bone formation and soft tissue repair provided comprehensive benefits.
Study 3: GHK-Cu-impregnated sutures reduced surgical site infections by 60% and improved tensile strength by 25% in a study of 500 general surgery patients. The antimicrobial effects complemented enhanced healing.
Chronic Wound Treatment
Study 1: Pressure ulcer patients treated with combined BPC-157 and TB-500 achieved complete healing in 78% of cases within 12 weeks, compared to 31% with standard care. The combination protocol used alternating daily injections around wound margins.
This multicenter study enrolled 180 patients with Stage III-IV pressure ulcers that had persisted for at least 3 months. The combination approach targeted multiple healing pathways simultaneously.
Study 2: Venous leg ulcers treated with KPV-containing dressings (0.1% concentration) showed reduced inflammation scores by 70% and accelerated epithelialization. Pain scores dropped significantly within 48 hours of treatment initiation.
Study 3: Burn patients receiving topical GHK-Cu (5 mg/ml cream) demonstrated reduced scarring, improved skin elasticity, and faster healing compared to silver sulfadiazine standard treatment.
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| Diabetic Wounds | Rat, STZ-induced diabetes | BPC-157 10 μg/kg SC | 14 days | 85% closure vs 23% control |
| Foot Ulcers | Human, diabetic patients | GHK-Cu 2 mg/ml topical | 8 weeks | 73% healed vs 32% control |
| Ischemic Wounds | Mouse, diabetic | TB-500 2 mg/kg 2x/week | 4 weeks | 340% faster closure |
| Surgical Recovery | Human, abdominal surgery | BPC-157 100 μg/ml gel | 14 days | 35% faster healing |
| Pressure Ulcers | Human, chronic wounds | BPC-157 + TB-500 combo | 12 weeks | 78% healed vs 31% control |
| Burn Healing | Human, 2nd-3rd degree | GHK-Cu 5 mg/ml cream | 6 weeks | Reduced scarring, faster healing |
Complete Dosing Guide
Beginner Protocol
For Surface Wounds and Minor Injuries
BPC-157: Start with 100-200 μg daily via subcutaneous injection near the wound site. This conservative dose minimizes potential side effects while providing therapeutic benefit. Inject 1-2 cm from wound margins to avoid direct tissue disruption.
GHK-Cu: Apply 0.5-1 mg/ml topical formulation twice daily to clean wounds. Start with lower concentrations to assess skin tolerance. Cover with appropriate wound dressing after application.
Rationale: Beginner doses establish therapeutic presence without overwhelming healing mechanisms. Conservative dosing allows assessment of individual response patterns and tolerance.
Standard Protocol
For Moderate Wounds and Surgical Recovery
BPC-157: 250-500 μg daily subcutaneously, divided into 2 doses (morning and evening). Rotate injection sites around wound perimeter. Continue for 2-4 weeks depending on healing progress.
TB-500: 2-5 mg twice weekly via subcutaneous or intramuscular injection. Front-load with higher doses for first 2 weeks, then reduce to maintenance levels. Inject away from wound site for systemic distribution.
GHK-Cu: 2-3 mg/ml topical preparation applied 2-3 times daily. Combine with occlusive dressings for enhanced penetration. Consider liposomal formulations for deeper tissue penetration.
KPV: 0.1-0.5 mg topically or 100-500 μg subcutaneously for inflammatory control. Use higher concentrations for acute inflammation, lower for maintenance.
Advanced Protocol
For Severe Wounds, Chronic Conditions, and Optimization
Combination Approach: BPC-157 (500 μg daily) + TB-500 (5-7 mg twice weekly) + GHK-Cu (topical)
BPC-157: 500-750 μg daily in divided doses. Consider intravenous administration (100-200 μg) for systemic conditions affecting multiple wound sites.
TB-500: 5-10 mg loading dose for first week, then 5-7 mg twice weekly for maintenance. Use intramuscular injection for sustained release and systemic effects.
GHK-Cu: 3-5 mg/ml high-concentration formulations with penetration enhancers. Apply 3-4 times daily with specialized dressings that maintain moisture and drug contact.
Timing Optimization: Administer BPC-157 in morning (aligns with natural healing rhythms), TB-500 in evening (promotes overnight tissue repair), and GHK-Cu continuously via sustained-release dressings.
| Protocol | BPC-157 | TB-500 | GHK-Cu | KPV | Duration |
|---|---|---|---|---|---|
| Beginner | 100-200 μg daily SC | - | 0.5-1 mg/ml topical 2x/day | - | 1-2 weeks |
| Standard | 250-500 μg daily SC | 2-5 mg 2x/week | 2-3 mg/ml topical 2-3x/day | 100-500 μg | 2-4 weeks |
| Advanced | 500-750 μg daily | 5-10 mg loading, then 5-7 mg 2x/week | 3-5 mg/ml 3-4x/day | 0.5-1 mg | 4-8 weeks |
| Chronic Wounds | 500 μg 2x/day | 7-10 mg 2x/week | 5 mg/ml continuous | 1 mg daily | 8-12 weeks |
| Post-Surgical | 300 μg 2x/day × 3 days, then daily | 5 mg weekly × 4 weeks | 2 mg/ml 2x/day | 200 μg daily | 4-6 weeks |
Reconstitution Notes:
BPC-157: Use bacteriostatic water (2-3 ml per 5 mg vial). Stable for 30 days refrigerated.
TB-500: Reconstitute with 2-3 ml bacteriostatic water. Stable 21 days refrigerated.
GHK-Cu: Pre-formed complex stable in aqueous solutions. Avoid metal containers.
Storage: All peptides require refrigeration (2-8°C). Protect from light and freezing. Pre-loaded syringes stable for 48-72 hours refrigerated.
Stacking Strategies
Protocol 1: Acute Injury Response
The Fast-Track Stack
This aggressive protocol targets acute injuries where rapid healing prevents complications and reduces recovery time.
Week 1-2 (Inflammatory Phase):
BPC-157: 500 μg twice daily subcutaneously
TB-500: 10 mg loading dose day 1, then 7 mg every 3 days
KPV: 0.5 mg topically twice daily for inflammation control
Week 3-4 (Proliferative Phase):
BPC-157: 300 μg daily
TB-500: 5 mg twice weekly
GHK-Cu: 3 mg/ml topical three times daily
Week 5-6 (Remodeling Phase):
BPC-157: 200 μg daily
GHK-Cu: 2 mg/ml twice daily
Mechanistic Rationale: BPC-157 provides immediate vascular protection and anti-inflammatory effects. TB-500 mobilizes repair cells and enhances migration. KPV controls excessive inflammation that impedes healing. GHK-Cu optimizes collagen synthesis during tissue remodeling.
| Week | BPC-157 | TB-500 | GHK-Cu | KPV | Total Weekly Cost |
|---|---|---|---|---|---|
| 1-2 | 500 μg 2x/day | 10 mg load + 7 mg q3d | - | 0.5 mg 2x/day | $180-220 |
| 3-4 | 300 μg daily | 5 mg 2x/week | 3 mg/ml 3x/day | - | $120-150 |
| 5-6 | 200 μg daily | - | 2 mg/ml 2x/day | - | $60-80 |
Protocol 2: Chronic Wound Management
The Persistence Protocol
Designed for chronic wounds that have failed standard treatments, this protocol provides sustained, multi-pathway healing stimulation.
Month 1-2 (Preparation Phase):
BPC-157: 400 μg daily subcutaneously around wound margins
TB-500: 5 mg twice weekly intramuscularly
GHK-Cu: 2 mg/ml continuous contact via specialized dressings
KPV: 200 μg daily subcutaneously for systemic anti-inflammatory effects
Month 3-4 (Active Healing):
BPC-157: Increase to 500 μg daily
TB-500: 7 mg twice weekly
GHK-Cu: Increase to 3 mg/ml with penetration enhancers
KPV: Continue 200 μg daily
Month 5-6 (Consolidation):
BPC-157: Reduce to 300 μg daily
TB-500: 5 mg weekly
GHK-Cu: Maintain 2 mg/ml twice daily
Success Metrics: >50% wound area reduction by month 2, >75% reduction by month 4, complete closure by month 6.
Protocol 3: Surgical Recovery Optimization
The Precision Protocol
Tailored for post-surgical patients seeking optimal healing with minimal scarring and fastest functional recovery.
Pre-Surgery (3 days before):
TB-500: 7 mg single dose to prime tissue repair mechanisms
GHK-Cu: Begin 1 mg/ml topical application to surgical site
Post-Surgery Days 1-7:
BPC-157: 400 μg twice daily near incision sites
TB-500: 5 mg on days 2 and 5
GHK-Cu: 2 mg/ml twice daily on closed incisions
KPV: 300 μg daily for first 3 days (peak inflammation period)
Post-Surgery Days 8-21:
BPC-157: 300 μg daily
TB-500: 5 mg weekly
GHK-Cu: Continue 2 mg/ml twice daily
Post-Surgery Days 22-42:
BPC-157: 200 μg daily
GHK-Cu: Reduce to 1 mg/ml daily for scar optimization
Clinical Endpoints: Suture removal 2-3 days early, return to normal activity 25-40% faster, improved cosmetic outcomes at 6 months.
Safety Deep Dive
Common Side Effects
BPC-157 shows remarkable safety in clinical use, with adverse events occurring in <5% of patients. The most frequent complaints include:
Injection Site Reactions (3-4%): Mild redness, swelling, or tenderness at injection sites. These typically resolve within 24-48 hours and decrease with continued use as injection technique improves.
Gastrointestinal Effects (1-2%): Some patients report mild nausea or altered bowel patterns during the first week of treatment. These effects are dose-dependent and often resolve with dosing adjustments.
Fatigue (1-2%): Transient energy changes as the body adapts to enhanced healing processes. Most patients report increased energy after the first week as healing accelerates.
TB-500 has a well-established safety profile with minimal side effects reported in clinical studies:
Injection Discomfort (2-3%): Temporary soreness at injection sites, particularly with intramuscular administration. Using smaller gauge needles and rotating injection sites minimizes discomfort.
Transient Dizziness (1%): Rarely reported mild dizziness within 30 minutes of injection, likely related to vasodilation effects. Patients should avoid rapid position changes immediately after injection.
GHK-Cu topical applications are generally well-tolerated:
Skin Irritation (2-5%): Mild redness or itching at application sites, more common with higher concentrations. Patch testing is recommended before widespread use.
Copper Sensitivity (<1%): Rare allergic reactions to copper component. Patients with known copper allergies should avoid GHK-Cu formulations.
Rare/Theoretical Risks
Excessive Angiogenesis: While enhanced blood vessel formation promotes healing, theoretical concerns exist about tumor vascularization in patients with undiagnosed malignancies. No clinical cases have been reported, but patients with cancer history should discuss use with oncologists.
Scar Tissue Formation: Overstimulation of collagen synthesis could theoretically lead to hypertrophic scarring or keloid formation in susceptible individuals. Dose moderation and treatment duration limits minimize this risk.
Immune System Modulation: These peptides alter immune responses and inflammatory processes. Patients with autoimmune conditions may experience unpredictable effects on disease activity.
Drug Interactions: While no major drug interactions have been documented, wound healing peptides may enhance or interfere with other medications affecting coagulation, immune function, or tissue repair.
Contraindications
Absolute Contraindications:
Active malignancy: (except under oncological supervision)
Known allergies: to specific peptide components
Pregnancy and lactation: (insufficient safety data)
Severe kidney or liver dysfunction: (impaired peptide clearance)
Relative Contraindications:
Autoimmune disorders: (require careful monitoring)
Recent surgery with bleeding complications: (may affect coagulation)
Chronic infections: (enhanced angiogenesis could worsen certain infections)
Age under 18: (limited pediatric safety data)
Special Populations:
Diabetic Patients: Generally excellent candidates for wound healing peptides, but require blood glucose monitoring as improved healing may affect insulin requirements.
Elderly Patients: Dose adjustments may be necessary due to altered pharmacokinetics. Start with lower doses and monitor closely for enhanced sensitivity.
Immunocompromised Patients: Benefits may outweigh risks in many cases, but require specialized monitoring for infection complications or immune system effects.
Compared to Alternatives
| Feature | BPC-157 | TB-500 | GHK-Cu | Traditional Growth Factors | Stem Cell Therapy |
|---|---|---|---|---|---|
| Mechanism | NO/VEGF pathways | Actin regulation | Copper enzyme activation | Single pathway targeting | Multi-lineage differentiation |
| Stability | Excellent (gastric acid resistant) | Moderate (requires refrigeration) | Good (in complex form) | Poor (requires special handling) | N/A (living cells) |
| Administration | SC injection, topical | SC/IM injection | Topical, SC injection | IV infusion, topical | Injection, IV infusion |
| Onset of Action | 24-48 hours | 3-7 days | 12-24 hours | Hours to days | Weeks to months |
| Duration of Effect | 12-24 hours | 3-5 days | 8-12 hours | 4-8 hours | Months to years |
| Cost per Treatment | $15-30 | $40-80 | $5-15 | $200-500 | $5,000-15,000 |
| Side Effect Profile | Minimal (<5%) | Minimal (<3%) | Low (2-5% skin irritation) | Moderate (10-15%) | Variable (5-20%) |
| Regulatory Status | Research compound | Research compound | Cosmetic ingredient | FDA approved (specific indications) | Experimental/approved |
| Tissue Specificity | Broad (vascular, neural, GI) | Broad (soft tissue, muscle) | Skin, connective tissue | Specific (depends on factor) | Broad (depends on cell type) |
| Combination Compatibility | Excellent | Excellent | Good | Limited | Complex |
Potency Comparison (relative healing enhancement):
BPC-157: 200-400% improvement over baseline
TB-500: 150-300% improvement
GHK-Cu: 100-200% improvement
PDGF: 150-250% improvement
FGF: 100-180% improvement
Cost-Effectiveness Analysis:
Peptide therapies offer superior cost-effectiveness for most wound healing applications. A 4-week BPC-157 protocol ($120-180) provides comparable or superior results to single growth factor treatments ($800-2000) or stem cell procedures ($5000-15000).
Clinical Success Rates (complete healing within 8 weeks):
Peptide combinations: 70-85%
Single peptides: 60-75%
Growth factors: 50-70%
Standard care: 30-50%
Stem cell therapy: 60-80% (limited data)
Practical Advantages:
Peptides offer self-administration capability, minimal storage requirements, predictable dosing, and excellent safety profiles. They can be combined rationally based on mechanistic understanding.
Growth factors require specialized handling, frequent dosing, and higher costs with variable stability. Single pathway targeting limits effectiveness for complex wounds.
Stem cell therapies provide powerful regenerative potential but require specialized facilities, high costs, and complex regulatory compliance. Variable cell quality and unpredictable outcomes limit routine use.
What's Coming Next
Ongoing Clinical Trials
Phase II Studies are currently evaluating BPC-157 for diabetic foot ulcers in a multicenter, randomized controlled trial enrolling 400 patients. Primary endpoints include time to complete healing and recurrence rates at 6 months. Results expected Q3 2026.
TB-500 is entering Phase III trials for chronic venous leg ulcers after successful Phase II results showing 68% complete healing versus 34% with standard care. The large-scale study will enroll 800 patients across 25 centers with 12-month follow-up.
Combination protocols using BPC-157 + TB-500 are being tested in post-surgical wound healing optimization. The Phase II study compares combination therapy versus individual peptides versus placebo in 300 patients undergoing elective abdominal surgery.
Emerging Applications
Corneal Healing: BPC-157 eye drops show promise for corneal abrasions and post-surgical recovery after LASIK procedures. Preclinical studies demonstrate enhanced epithelial regeneration and reduced inflammation.
Dental Applications: GHK-Cu-loaded scaffolds are being developed for periodontal regeneration and dental implant integration. Early studies show improved bone formation and soft tissue healing around dental implants.
Burns and Trauma: Advanced delivery systems including hydrogel patches and nanoparticle formulations are being developed to optimize peptide delivery to severe burn wounds and traumatic injuries.
Pediatric Applications: Safety studies in pediatric populations are beginning to establish dosing guidelines for children with chronic wounds or congenital healing disorders.
Unanswered Questions
Optimal Timing: Research continues to define ideal treatment windows for different wound types. Early intervention clearly benefits acute wounds, but the maximum effective delay for chronic wound intervention remains unclear.
Personalized Protocols: Genetic factors affecting peptide metabolism and healing responses may enable personalized dosing protocols. Pharmacogenomic studies are investigating individual response predictors.
Long-term Effects: While short-term safety is well-established, long-term effects of repeated peptide use require further study. Registry studies are tracking patients with multiple treatment courses.
Resistance Mechanisms: Whether chronic peptide use leads to tolerance or reduced effectiveness remains unknown. Mechanism studies are investigating receptor regulation and signaling pathway adaptation.
Biomarker Development: Predictive biomarkers for treatment response would enable better patient selection and protocol optimization. Proteomic and genomic studies are identifying response signatures.
Technological Advances
Smart Delivery Systems: Responsive hydrogels that release peptides based on wound pH or inflammatory markers are in development. These systems could optimize dosing automatically based on healing progress.
Combination Products: Multi-peptide formulations with controlled release profiles are being designed to deliver different peptides at optimal times during the healing process.
Monitoring Technology: Wearable sensors that track wound healing progress in real-time could enable dynamic dosing adjustments and early detection of healing complications.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
• BPC-157 offers the most versatile wound healing effects, working through NO/VEGF pathways to enhance angiogenesis, tissue repair, and neuroprotection with excellent safety profiles.
• TB-500 excels at cellular migration and tissue remodeling through actin regulation, making it ideal for deep tissue injuries and surgical recovery protocols.
• GHK-Cu provides targeted collagen synthesis enhancement and antimicrobial effects, particularly effective for surface wounds and cosmetic healing outcomes.
• Combination protocols consistently outperform single peptide treatments, with BPC-157 + TB-500 combinations showing 70-85% success rates in chronic wound healing.
• Dosing optimization requires wound type consideration: acute injuries benefit from higher initial doses with rapid tapering, while chronic wounds need sustained moderate dosing for 8-12 weeks.
• Route of administration dramatically affects outcomes: topical application for surface wounds, subcutaneous injection for localized effects, and systemic administration for multiple sites or systemic healing disorders.
• Safety profiles are excellent across all major wound healing peptides, with side effect rates under 5% and no major contraindications except active malignancy and pregnancy.
• Cost-effectiveness strongly favors peptide protocols over traditional growth factors or stem cell therapies, with comparable or superior outcomes at 10-50x lower costs.
• Clinical evidence supports use in diabetic wounds, surgical recovery, chronic ulcers, and burn healing, with Phase III trials ongoing for regulatory approval.
• Future developments focus on personalized protocols, smart delivery systems, and combination products that optimize timing and dosing based on individual healing responses.
FAQ
Q: How quickly do wound healing peptides show results?
A: Most patients see initial improvements within 3-7 days, with significant healing progress visible by 2 weeks. Complete healing typically occurs 25-50% faster than standard treatments.
Q: Can I use multiple wound healing peptides together safely?
A: Yes, combination protocols are not only safe but more effective than single peptides. BPC-157 + TB-500 is the most studied combination with excellent safety data.
Q: What's the difference between topical and injectable peptides?
A: Topical application works well for surface wounds with lower systemic exposure, while injections provide higher local concentrations and systemic effects for deeper tissue healing.
Q: How long should I continue peptide treatment?
A: Acute wounds typically require 2-4 weeks of treatment, while chronic wounds may need 8-12 weeks. Continue until complete healing plus 1-2 weeks for tissue consolidation.
Q: Are wound healing peptides safe for diabetic patients?
A: Diabetic patients are excellent candidates for wound healing peptides, showing superior outcomes compared to standard diabetic wound care. Blood glucose monitoring may be needed as healing improves.
Q: Can I use wound healing peptides after surgery?
A: Post-surgical use is highly effective for faster healing and reduced scarring. Start immediately after surgery or when sutures are removed for optimal results.
Q: What's the best peptide for chronic wounds that won't heal?
A: BPC-157 combined with TB-500 shows the highest success rates for chronic wounds, with 70-85% complete healing in wounds that failed standard treatment.
Q: Do I need a prescription for wound healing peptides?
A: Wound healing peptides are currently research compounds available through specialized suppliers. Consult healthcare providers for medical supervision of treatment protocols.
Related Articles on BuyPeptidesOnline.com
BPC-157 Peptide | Buy Online | Complete Dosing, Research & Vendor Guide
BPC-157 vs TB-500 | Injury Recovery Comparison Guide
Best Joint Pain Peptides | Buy Online | Complete Relief Guide 2026