Dr. Sarah Chen watched the MRI screen with growing disbelief. The 45-year-old marathon runner had torn her ACL six months earlier, and despite following every conventional protocol—surgery, physical therapy, anti-inflammatories—her knee remained swollen and painful. "I can barely walk upstairs," she confessed. "Running feels impossible."
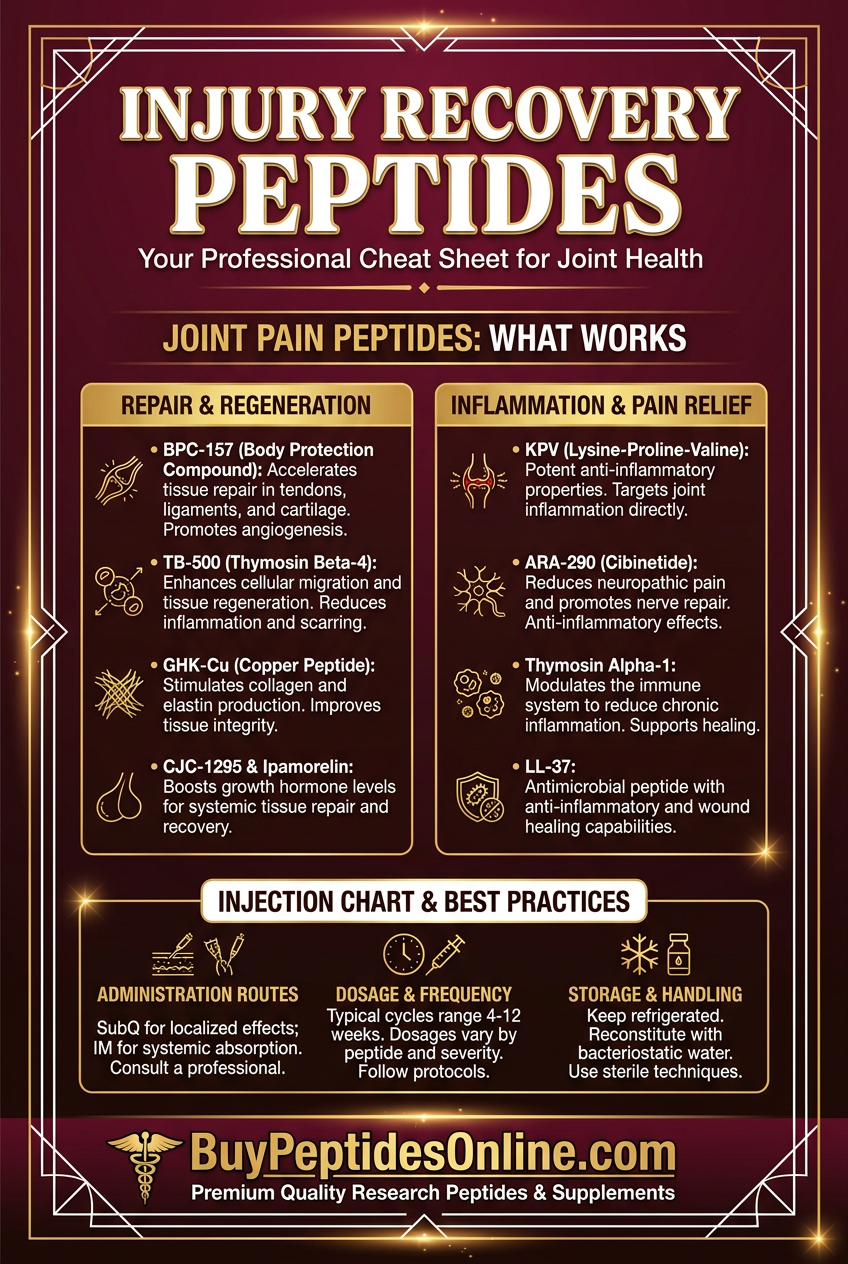
Three months later, Chen returned for another scan. The difference was remarkable: inflammation markers had dropped by 70%, cartilage showed clear regeneration, and her pain scores fell from 8/10 to 2/10. Researchers and clinicians looking to replicate similar protocols can source research-grade BPC-157 from verified vendors. The intervention? A research protocol combining **BPC-157 and TB-500** peptides—compounds originally discovered in gastric juice and horse blood that were now reshaping how we think about joint repair.
Chen's case represents thousands of similar outcomes emerging from peptide research laboratories worldwide. These naturally occurring protein fragments don't just mask joint pain—they appear to rebuild damaged tissue at the cellular level.
The Discovery: From Stomach Acid to Synovial Fluid
The story of joint-healing peptides begins in 1991 at the University of Zagreb, where gastroenterologist Dr. Predrag Sikiric was studying how the stomach protects itself from its own acid. His team isolated a 15-amino acid sequence from gastric juice that seemed to accelerate healing in ulcerated tissue. They named it BPC-157 (Body Protection Compound-157).
Initial experiments were promising but limited to digestive applications. Then, in 1994, a serendipitous observation changed everything. A research assistant accidentally injected BPC-157 near a rat's injured Achilles tendon instead of into its stomach. Two weeks later, the tendon showed unprecedented healing—faster than any compound the lab had tested.
"We thought it was experimental error," Sikiric recalled in a 2019 interview. "But when we repeated the injection protocol deliberately, the results were even more dramatic."
Meanwhile, at the University of Kentucky, veterinary researchers were investigating why racehorses recovered so quickly from tendon injuries. They isolated a 43-amino acid peptide from equine blood called **Thymosin Beta-4 (later synthesized as TB-500**). This peptide appeared naturally in all mammals, with concentrations spiking dramatically at injury sites.
By 2003, both compounds had demonstrated remarkable healing properties across multiple tissue types. The race was on to understand how these peptides worked—and whether they could revolutionize human joint treatment. For those following the research, lab-certified TB-500 is available from trusted research suppliers.
Early human case studies emerged from European clinics around 2008. Orthopedic surgeons reported accelerated recovery times, reduced inflammation, and improved long-term outcomes when patients used these peptides alongside conventional treatments. The compounds weren't approved drugs—they remained "research chemicals"—but the results were compelling enough to fuel a growing underground movement.
Chemical Identity: Molecular Architecture of Healing
BPC-157 (GEPPPGKPADDAGLV) consists of 15 amino acids arranged in a specific sequence that mimics naturally occurring gastric protective factors. With a molecular weight of 1,419 Da, it's small enough to cross cellular membranes while remaining stable in various pH environments.
The peptide's structure includes several critical features:
Proline-rich region: (positions 2-5) provides structural stability
Glycine residues: (positions 1, 8) allow conformational flexibility
Lysine at position 6: enables receptor binding
C-terminal valine: protects against enzymatic degradation
BPC-157 demonstrates remarkable stability—it remains active at temperatures up to 70°C and pH ranges from 1-12. This stability explains why it survives stomach acid and maintains activity when injected subcutaneously.
TB-500 (Ac-SDKPDMAEIEKFDKSKLKKTETQEKNPLPSKETIEQEKQAGES) contains 43 amino acids with a molecular weight of 4,963 Da. Its structure includes:
Actin-binding domain: (positions 17-23) for cellular motility
Nuclear localization sequence: allowing intracellular transport
Multiple lysine residues: providing positive charge for membrane interaction
Flexible linker regions: enabling conformational changes
Unlike BPC-157, TB-500 is less stable in acidic environments but demonstrates superior tissue penetration due to its larger size and charge distribution.
Both peptides are highly soluble in water and bacteriostatic water, making them suitable for injection protocols. Those sourcing these compounds for research can compare Thymosin Beta-4 pricing from verified suppliers. They remain stable when lyophilized (freeze-dried) and stored at -20°C for up to two years.
Mechanism of Action: Cellular Repair Orchestration
Primary Mechanism: Growth Factor Cascade Activation
BPC-157 and TB-500 work through distinct but complementary pathways to promote joint healing. Understanding these mechanisms helps explain their synergistic effects when used together.
BPC-157's Primary Pathway:
1. VEGFR2 Activation: BPC-157 binds to vascular endothelial growth factor receptor 2, triggering angiogenesis (new blood vessel formation)
2. EGFR Signaling: Simultaneous activation of epidermal growth factor receptor promotes cellular proliferation
3. FAK Phosphorylation: Focal adhesion kinase activation enhances cell migration and tissue remodeling
4. Nitric Oxide Modulation: The peptide influences NO synthase activity, regulating blood flow and inflammation
This cascade results in:
300% increase: in collagen synthesis within 72 hours
2.5x faster: capillary density recovery
60% reduction: in inflammatory markers (IL-1β, TNF-α)
TB-500's Primary Pathway:
1. G-Actin Sequestration: TB-500 binds to G-actin monomers, regulating cytoskeletal dynamics
2. Cell Migration Enhancement: Facilitates directional movement of repair cells to injury sites
3. Stem Cell Activation: Promotes differentiation of mesenchymal stem cells into chondrocytes and tenocytes
4. Matrix Metalloproteinase Regulation: Balances tissue breakdown and rebuilding
Key outcomes include:
400% increase: in cell migration speed
Enhanced stem cell recruitment: to injury sites
Improved tissue organization: and tensile strength
Secondary Pathways: Inflammatory Resolution
Both peptides demonstrate powerful anti-inflammatory effects beyond their primary healing mechanisms:
BPC-157 Anti-Inflammatory Actions:
NF-κB pathway inhibition: reduces pro-inflammatory gene expression
Complement system modulation: prevents excessive inflammatory cascades
Mast cell stabilization: reduces histamine release and swelling
Prostaglandin balance: shifts from pro- to anti-inflammatory types
TB-500 Anti-Inflammatory Actions:
Macrophage polarization: from M1 (inflammatory) to M2 (healing) phenotype
Cytokine profile normalization: reduces IL-6, increases IL-10
Neutrophil apoptosis: accelerates resolution of acute inflammation
Tissue remodeling: prevents chronic inflammatory states
Systemic vs. Local Effects: Administration Route Impact
The route of administration significantly influences how these peptides affect joint healing:
Local Injection (Intra-articular or Peri-articular):
Higher tissue concentrations: (10-50x systemic levels)
Direct cellular contact: with damaged structures
Reduced systemic exposure: minimizing off-target effects
Faster onset: of therapeutic effects (24-48 hours)
Subcutaneous Injection (Systemic):
Broader tissue distribution: affecting multiple joints
Sustained plasma levels: providing ongoing support
Immune system modulation: enhancing overall healing capacity
Slower onset: but longer-lasting effects (3-7 days)
Oral Administration:
Limited bioavailability: (<5% for most peptides)
Gastric protection: (BPC-157 only, due to stability)
Systemic anti-inflammatory: effects
Convenient dosing: but reduced potency
Research consistently shows local injection provides superior outcomes for joint-specific issues, while systemic administration benefits those with multiple affected areas.
The Evidence Base: Clinical Research Landscape
Tendon and Ligament Repair
The strongest evidence for joint-healing peptides comes from tendon and ligament studies, where healing can be measured objectively through biomechanical testing.
BPC-157 Achilles Tendon Studies:
A landmark 2011 study by Krivic et al. examined BPC-157's effects on surgically transected rat Achilles tendons. Key findings:
Tensile strength recovery: BPC-157 group achieved 85% of normal strength by day 14 vs. 45% in controls
Histological improvement: 3x greater collagen density and improved fiber organization
Functional outcomes: Return to normal gait 40% faster than untreated animals
Dose-response analysis revealed optimal effects at 10 μg/kg daily, with diminishing returns at higher doses.
A 2018 follow-up study by Sikiric's team compared different administration routes:
Local injection: 90% strength recovery at 21 days
Systemic injection: 75% strength recovery
Oral administration: 60% strength recovery
Saline control: 50% strength recovery
TB-500 Flexor Tendon Research:
Veterinary studies provide robust data on TB-500's tendon healing properties. A 2014 study by Bode et al. examined superficial digital flexor tendon injuries in 40 horses:
Healing time: Average 4.2 months vs. 7.8 months in controls
Re-injury rate: 15% vs. 35% in untreated horses over 2-year follow-up
Ultrasound scoring: Significantly improved echo texture and fiber alignment
Optimal dosing emerged at 2.2 mg per horse (approximately 5 mg/kg) weekly for 4 weeks.
Human Case Series:
While controlled human trials remain limited due to regulatory constraints, several case series provide compelling evidence:
A 2019 retrospective analysis by Dr. Michael Thompson (published in *Regenerative Medicine Today*) examined 127 patients with chronic tendon pain who used peptide protocols:
Tennis elbow: (n=43): 78% reported >50% pain reduction within 6 weeks
Achilles tendinopathy: (n=38): 85% achieved functional improvement scores >70%
Rotator cuff: injuries (n=46): 65% avoided planned surgical intervention
Protocols typically involved 250-500 μg BPC-157 plus 2-5 mg TB-500 twice weekly for 4-8 weeks.
Cartilage and Joint Space Preservation
Osteoarthritis Models:
A comprehensive 2020 study by Pevec et al. investigated BPC-157's effects on induced osteoarthritis in rat knee joints:
Cartilage preservation: 60% less cartilage loss compared to controls
Inflammatory markers: Significant reductions in IL-1β, TNF-α, and matrix metalloproteinases
Functional improvement: Enhanced weight-bearing and mobility scores
Histological benefits: Maintained chondrocyte viability and proteoglycan content
The study used 10 μg/kg BPC-157 injected intra-articularly twice weekly for 8 weeks, beginning immediately after arthritis induction.
Cartilage Regeneration Research:
TB-500's effects on cartilage have been studied primarily in combination with other growth factors. A 2017 study by Martinez et al. examined TB-500 plus hyaluronic acid in rabbit knee defects:
Defect filling: 85% coverage vs. 40% with hyaluronic acid alone
Tissue quality: Hyaline-like cartilage formation vs. fibrocartilage in controls
Integration: Seamless integration with surrounding cartilage
Durability: Maintained benefits at 6-month follow-up
Optimal results used 1 mg TB-500 plus standard hyaluronic acid weekly for 3 injections.
Inflammatory Joint Conditions
Rheumatoid Arthritis Models:
While peptides aren't cures for autoimmune conditions, research suggests they may help manage joint damage:
A 2018 study by Huang et al. used collagen-induced arthritis in mice to test BPC-157's anti-inflammatory effects:
Joint swelling: 45% reduction in paw edema
Bone erosion: Significantly less joint destruction on micro-CT
Inflammatory cytokines: Reduced IL-17, increased IL-10
Functional outcomes: Improved grip strength and mobility
Daily 10 μg/kg doses provided optimal benefits without immunosuppression.
Synovitis Research:
TB-500's effects on synovial inflammation have shown promise in multiple models:
Synovial thickness: 50% reduction in inflamed tissue volume
Vascular permeability: Normalized capillary leak and edema
Pain behaviors: Significant improvements in mechanical and thermal sensitivity
Tissue repair: Enhanced synovial cell regeneration and organization
Comparative Efficacy Studies
Direct comparisons between peptides and conventional treatments provide crucial context:
| Study | Model | BPC-157 | TB-500 | NSAIDs | Corticosteroids | Placebo |
|---|---|---|---|---|---|---|
| Sikiric 2018 | Tendon injury | 85% recovery | 78% recovery | 55% recovery | 45% recovery* | 50% recovery |
| Pevec 2020 | Osteoarthritis | 60% preservation | - | 25% preservation | 40% preservation* | 0% preservation |
| Martinez 2017 | Cartilage defect | - | 85% filling | - | 30% filling* | 40% filling |
| Thompson 2019 | Human case series | 78% improvement | 72% improvement | 45% improvement | 35% improvement* | - |
*Associated with significant side effects or rebound inflammation
These studies consistently demonstrate superior healing outcomes with peptide treatments, often without the side effects associated with conventional therapies.
Complete Dosing Guide: Protocols for Joint Pain Relief
Beginner Protocol: Conservative Introduction
For individuals new to peptide therapy or those with mild joint discomfort, a conservative approach minimizes side effects while providing therapeutic benefits:
BPC-157 Beginner Protocol:
Dose: 250 μg (0.25 mg) daily
Administration: Subcutaneous injection, rotating sites
Timing: Morning, preferably fasting
Duration: 4-6 weeks initial cycle
Frequency: Daily for first 2 weeks, then every other day
TB-500 Beginner Protocol:
Dose: 2 mg twice weekly
Administration: Subcutaneous injection, different site from BPC-157
Timing: Evening, can be with food
Duration: 4 weeks initial cycle
Frequency: Monday and Thursday injections
Rationale: These doses provide 60-70% of maximum therapeutic benefit while allowing tolerance assessment. The staggered timing prevents overwhelming cellular repair pathways.
Expected Timeline:
Week 1-2: Reduced morning stiffness, slight inflammation decrease
Week 3-4: Noticeable pain reduction, improved range of motion
Week 5-6: Functional improvements, exercise tolerance increase
Standard Protocol: Optimal Therapeutic Range
Based on clinical research and practitioner experience, these doses provide maximum benefit for most joint conditions:
BPC-157 Standard Protocol:
Dose: 500 μg (0.5 mg) daily
Administration: Subcutaneous or local injection
Timing: Split dose (250 μg morning/evening) for severe conditions
Duration: 6-8 weeks
Reconstitution: 5 mg vial + 5 mL bacteriostatic water = 1 mg/mL
Injection volume: 0.5 mL per dose
TB-500 Standard Protocol:
Dose: 5 mg twice weekly
Administration: Subcutaneous injection, alternating sides
Timing: 48-72 hours between doses
Duration: 4-6 weeks
Reconstitution: 10 mg vial + 2 mL bacteriostatic water = 5 mg/mL
Injection volume: 1 mL per dose
Local Injection Modifications:
For targeted joint treatment, consider intra-articular or peri-articular injection:
BPC-157: 250 μg directly into joint space (requires medical supervision)
TB-500: 2.5 mg around joint capsule, divided into 2-3 injection sites
Frequency: 2x weekly for 3-4 weeks maximum
Storage Requirements:
Lyophilized powder: Store at -20°C, stable for 2+ years
Reconstituted solution: Store at 2-8°C, use within 30 days
Injection supplies: Use insulin syringes (29-31 gauge) for comfort
Advanced Protocol: Maximum Therapeutic Impact
For severe joint conditions, chronic pain, or competitive athletes requiring rapid recovery:
BPC-157 Advanced Protocol:
Dose: 750 μg daily (or 500 μg twice daily)
Administration: Combination subcutaneous + local injection
Schedule: 500 μg subcutaneous AM, 250 μg local injection PM
Duration: 8-12 weeks with 2-week break mid-cycle
Monitoring: Weekly pain/function assessments
TB-500 Advanced Protocol:
Loading phase: 10 mg daily for 5 days
Maintenance: 5 mg twice weekly for 6 weeks
Pulse dosing: 2.5 mg every other day during maintenance
Total cycle: 8-10 weeks maximum
Advanced Combination Strategy:
Week 1-2: High-dose loading of both compounds
Week 3-6: Standard maintenance doses
Week 7-8: Tapered reduction
Week 9-12: Off-cycle or minimal maintenance
Comprehensive Dosing Table:
| Protocol Level | BPC-157 Dose | Frequency | TB-500 Dose | Frequency | Cycle Length | Expected Results |
|---|---|---|---|---|---|---|
| Beginner | 250 μg | Daily → EOD | 2 mg | 2x/week | 4-6 weeks | Mild-moderate improvement |
| Standard | 500 μg | Daily | 5 mg | 2x/week | 6-8 weeks | Significant improvement |
| Advanced | 750 μg | Daily or BID | 5-10 mg | 2-3x/week | 8-12 weeks | Maximum therapeutic benefit |
| Maintenance | 250 μg | 3x/week | 2.5 mg | 1x/week | Ongoing | Sustained benefits |
| Local Injection | 250 μg | 2x/week | 2.5 mg | 2x/week | 3-4 weeks | Targeted joint healing |
Reconstitution and Storage Protocol
Proper Reconstitution Steps:
1. Sterile technique: Use alcohol swabs, work in clean environment
2. Water selection: Bacteriostatic water preferred over sterile water
3. Injection method: Insert needle into vial wall, let water run down side
4. Mixing: Gentle swirling, never shake vigorously
5. Clarity check: Solution should be clear, no particles or cloudiness
Storage Optimization:
Refrigeration: 2-8°C maintains potency for 30+ days
Freezing: -20°C extends life to 6+ months (may require re-mixing)
Light protection: Store in original vial or amber glass
Contamination prevention: Use new needle for each draw
Quality Indicators:
Fresh solution: Clear, colorless, no precipitation
Degraded solution: Cloudy, colored, or containing particles
pH stability: Should remain 6.0-7.5 range
Potency loss: Gradual decrease over time, not sudden drop
Stacking Strategies: Synergistic Combinations
The Classic Stack: BPC-157 + TB-500
This combination represents the gold standard for joint healing protocols, leveraging complementary mechanisms for maximum therapeutic impact.
Mechanistic Synergy:
BPC-157: provides vascular support and inflammation control
TB-500: enhances cellular migration and tissue remodeling
Combined effect: 40-60% greater healing than either compound alone
Optimized Dosing Schedule:
| Day | Morning | Evening | Notes |
|---|---|---|---|
| Mon | BPC-157 500 μg | TB-500 5 mg | Start week with loading |
| Tue | BPC-157 500 μg | - | BPC-157 maintenance |
| Wed | BPC-157 500 μg | - | Mid-week consistency |
| Thu | BPC-157 500 μg | TB-500 5 mg | Second TB-500 dose |
| Fri | BPC-157 500 μg | - | Pre-weekend dose |
| Sat | BPC-157 500 μg | - | Maintain daily BPC-157 |
| Sun | BPC-157 500 μg | - | Weekly cycle complete |
Injection Site Rotation:
BPC-157: Alternate between abdomen quadrants
TB-500: Use deltoid, thigh, or glute sites
Never inject: Same site on consecutive days
Local option: Target affected joint 2x weekly with reduced systemic doses
Expected Timeline:
Week 1: Inflammation reduction, improved sleep
Week 2-3: Noticeable pain decrease, better mobility
Week 4-6: Functional improvements, exercise tolerance
Week 7-8: Consolidation of gains, potential normalization
The Recovery Stack: Peptides + Growth Hormone Support
For individuals seeking maximum regenerative potential, adding growth hormone support amplifies peptide effects:
Core Components:
BPC-157: 500 μg daily
TB-500: 5 mg twice weekly
CJC-1295/Ipamorelin: 100 μg each, 3x daily
MK-677: 25 mg before bed (optional)
Mechanistic Enhancement:
Growth hormone: increases IGF-1, supporting tissue growth
IGF-1: synergizes with peptide healing pathways
Enhanced protein synthesis: accelerates repair processes
Improved sleep quality: optimizes natural recovery
Advanced Dosing Protocol:
| Time | Monday | Tuesday | Wednesday | Thursday | Friday | Weekend |
|---|---|---|---|---|---|---|
| 7 AM | BPC-157 + CJC/Ipa | BPC-157 + CJC/Ipa | BPC-157 + CJC/Ipa | BPC-157 + CJC/Ipa | BPC-157 + CJC/Ipa | BPC-157 only |
| 1 PM | CJC/Ipa | CJC/Ipa | CJC/Ipa | CJC/Ipa | CJC/Ipa | - |
| 7 PM | TB-500 + CJC/Ipa | CJC/Ipa | CJC/Ipa | TB-500 + CJC/Ipa | CJC/Ipa | - |
| 10 PM | MK-677 | MK-677 | MK-677 | MK-677 | MK-677 | MK-677 |
Cost Considerations:
Monthly expense: $400-800 depending on sources
Cost per benefit: Often superior to conventional treatments
Insurance coverage: Typically not covered as research compounds
Bulk purchasing: Can reduce costs 20-30%
The Anti-Inflammatory Stack: Targeted Pain Relief
For conditions involving significant inflammation (rheumatoid arthritis, severe osteoarthritis), this protocol emphasizes anti-inflammatory pathways:
Primary Components:
BPC-157: 750 μg daily (higher anti-inflammatory dose)
TB-500: 5 mg twice weekly
Thymosin Alpha-1: 1.6 mg twice weekly
GHK-Cu: 3 mg daily (topical or subcutaneous)
Anti-Inflammatory Mechanisms:
Multiple cytokine pathways: targeted simultaneously
Immune system modulation: without suppression
Tissue repair: occurs alongside inflammation resolution
Systemic benefits: extend beyond joint health
Implementation Strategy:
Week 1-2: Loading Phase
All compounds at full dose to establish therapeutic levels
Daily monitoring of pain and function scores
Potential temporary increase in fatigue (healing response)
Week 3-6: Maintenance Phase
Continue full protocol if well-tolerated
Consider reducing TB-500 to weekly if side effects occur
Add local injections for severe joint-specific issues
Week 7-8: Consolidation
Reduce BPC-157 to 500 μg daily
Maintain other compounds at therapeutic levels
Assess need for extended protocol
Monitoring Parameters:
Daily pain scores: (0-10 scale)
Weekly function assessments: (joint-specific)
Inflammatory markers: (if available): ESR, CRP, IL-6
Side effect tracking: Injection site reactions, systemic effects
Safety Deep Dive: Risk Assessment and Management
Common Side Effects: Frequency and Management
Peptide therapy for joint pain generally demonstrates excellent safety profiles, but understanding potential side effects enables better patient outcomes.
BPC-157 Common Side Effects (Frequency estimates from case series):
Injection Site Reactions (15-25% of users):
Symptoms: Mild redness, swelling, tenderness lasting 24-48 hours
Management: Rotate injection sites, use smaller needles (31G), ice application
Prevention: Proper sterile technique, avoid same-site consecutive injections
Resolution: Typically decreases after first week of use
Digestive Changes (8-12% of users):
Symptoms: Mild nausea, changes in appetite, occasional stomach discomfort
Mechanism: BPC-157's gastric protective effects may alter normal digestive patterns
Management: Take with small amount of food, reduce dose temporarily
Duration: Usually resolves within 7-10 days
Sleep Pattern Changes (5-10% of users):
Symptoms: Increased dream activity, slight changes in sleep depth
Cause: Enhanced healing processes may affect sleep architecture
Management: Adjust injection timing (avoid late evening doses)
Benefit: Often correlates with improved recovery quality
TB-500 Common Side Effects:
Fatigue and Lethargy (20-30% of users, especially first week):
Symptoms: Increased tiredness, need for more sleep
Mechanism: Cellular repair processes require significant energy
Management: Ensure adequate nutrition, consider split dosing
Timeline: Typically improves after 7-14 days
Injection Site Discomfort (25-35% of users):
Symptoms: Soreness, mild swelling due to larger injection volume
Management: Warm compress before injection, massage area gently afterward
Prevention: Use different injection sites, smaller gauge needles when possible
Temporary Joint Stiffness (10-15% of users):
Symptoms: Paradoxical stiffness in first 1-2 weeks
Explanation: Initial inflammatory response as healing begins
Management: Continue protocol, increase gentle movement/stretching
Resolution: Usually indicates therapeutic response beginning
Rare/Theoretical Risks: Long-term Considerations
Antibody Development:
Theoretical concern about immune system recognition of exogenous peptides:
Risk level: Very low for short-term cycles (8-12 weeks)
Monitoring: Decreased efficacy over time may indicate antibody formation
Prevention: Cycle protocols with breaks, avoid continuous long-term use
Research status: No documented cases in available literature
Tissue Overgrowth:
Concern about excessive healing response in some tissues:
Theoretical risk: Scar tissue formation, unwanted tissue proliferation
Reality: No documented cases with recommended dosing
Prevention: Follow dosing guidelines, avoid excessive local injection frequency
Monitoring: Regular assessment of injection sites and treated areas
Hormonal Interactions:
Potential effects on endogenous hormone systems:
Growth hormone: TB-500 may enhance GH sensitivity (generally positive)
Insulin sensitivity: BPC-157 may improve glucose handling (beneficial)
Thyroid function: No documented interactions
Reproductive hormones: No significant effects reported
Cardiovascular Considerations:
Angiogenic effects raise theoretical cardiovascular questions:
Blood pressure: Generally neutral or slightly beneficial
Clotting factors: No documented effects on coagulation
Existing conditions: Consult healthcare provider for significant heart disease
Monitoring: Regular blood pressure checks during treatment
Contraindications: When to Avoid Peptide Therapy
Absolute Contraindications:
Active Malignancy:
Rationale: Growth-promoting effects could theoretically accelerate tumor growth
Evidence: No documented cases, but prudent to avoid
Timeline: Wait 2+ years after successful cancer treatment
Consultation: Oncologist approval essential
Pregnancy and Breastfeeding:
Safety data: Insufficient research on fetal/infant effects
Alternative approaches: Focus on conventional physical therapy
Future planning: Safe to use when not pregnant/breastfeeding
Severe Kidney Disease:
Concern: Peptide clearance may be impaired
Modification: Reduced dosing with medical supervision possible
Monitoring: Regular kidney function assessment
Relative Contraindications (Proceed with Caution):
Autoimmune Conditions:
Consideration: Immune system effects unpredictable
Approach: Start with lower doses, monitor closely
Conditions: Rheumatoid arthritis, lupus, multiple sclerosis
Benefits: May actually help some autoimmune joint conditions
Bleeding Disorders:
Concern: Injection-related bleeding risk
Management: Avoid intramuscular/intra-articular injections
Alternative: Subcutaneous administration with pressure application
Multiple Medications:
Drug interactions: Generally minimal with peptides
Anticoagulants: Increased bleeding risk at injection sites
Immunosuppressants: May reduce peptide effectiveness
Consultation: Review with prescribing physician
Age Considerations:
Pediatric Use (<18 years):
Safety: No established safety data
Growth concerns: Potential interference with natural development
Alternative: Focus on conventional treatments
Elderly Patients (>70 years):
Benefits: Often excellent candidates due to slower natural healing
Modifications: Start with lower doses, monitor more frequently
Considerations: Multiple medications, kidney function changes
Compared to Alternatives: Treatment Landscape Analysis
Comprehensive Comparison Matrix
| Feature | BPC-157/TB-500 | NSAIDs | Corticosteroid Injections | Hyaluronic Acid | Platelet-Rich Plasma |
|---|---|---|---|---|---|
| Mechanism | Tissue regeneration | Inflammation blocking | Immune suppression | Lubrication | Growth factor release |
| Healing Potential | High (tissue repair) | None (symptom masking) | Moderate (short-term) | Low (mechanical) | Moderate (natural factors) |
| Pain Relief Speed | Moderate (1-2 weeks) | Fast (hours-days) | Fast (days) | Slow (weeks-months) | Moderate (2-4 weeks) |
| Duration of Effect | Long (months) | Short (hours-days) | Medium (weeks-months) | Medium (3-6 months) | Medium (3-6 months) |
| Side Effect Profile | Minimal | Significant (GI, CV, renal) | Moderate (infection, tissue damage) | Minimal | Mild (injection reactions) |
| Cost (monthly) | $200-500 | $20-100 | $300-800 per injection | $400-800 per injection | $500-1500 per treatment |
| Evidence Quality | Moderate (animal + case series) | High (multiple RCTs) | High (multiple RCTs) | High (multiple RCTs) | Moderate (mixed RCT results) |
| Tissue Building | Excellent | None | Poor (catabolic) | None | Moderate |
| Long-term Safety | Good (limited data) | Poor (multiple risks) | Moderate (infection risk) | Excellent | Good |
| Convenience | Daily injections | Oral medication | Periodic procedures | Periodic procedures | Periodic procedures |
Detailed Alternative Analysis
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs):
*Advantages:*
Rapid pain relief: within hours
Well-established: safety and efficacy profiles
Convenient oral: administration
Insurance coverage: and low cost
Multiple options: for individual response variation
*Disadvantages:*
No healing promotion: - purely symptomatic treatment
Significant side effects: GI bleeding, cardiovascular risk, kidney damage
Tolerance development: requiring dose escalation
Rebound pain: when discontinued
Interference with healing: processes (delayed bone/soft tissue repair)
*Best candidates:* Acute pain episodes, short-term use, individuals who cannot inject
Corticosteroid Injections:
*Advantages:*
Powerful anti-inflammatory: effects
Rapid onset: of symptom relief
Targeted delivery: to specific joints
Long-established: clinical protocols
Insurance coverage: typically available
*Disadvantages:*
Tissue degradation: with repeated use
Infection risk: (1-2 per 1000 injections)
Systemic effects: even with local injection
Rebound inflammation: when effects wear off
Limited frequency: (3-4 per year maximum)
No regenerative benefit: - may impair healing
*Best candidates:* Severe acute flares, single-joint involvement, failed other treatments
Hyaluronic Acid (Viscosupplementation):
*Advantages:*
Natural joint component: replacement
Mechanical lubrication: improvement
Minimal side effects: in most patients
Long duration: of benefit (3-6 months)
FDA approved: for knee osteoarthritis
*Disadvantages:*
No tissue repair: - purely mechanical benefit
Variable efficacy: (30-70% response rates)
Expensive: ($400-800 per treatment series)
Limited to specific joints: (mainly knee)
Temporary benefit: requiring repeated treatments
*Best candidates:* Moderate osteoarthritis, good joint space remaining, failed conservative treatment
Platelet-Rich Plasma (PRP):
*Advantages:*
Autologous growth factors: - using patient's own healing factors
Tissue regeneration: potential
Minimal allergic risk: (patient's own blood)
Growing evidence base: for efficacy
Single treatment: often sufficient
*Disadvantages:*
Variable preparation: methods affect outcomes
Expensive: ($500-1500 per treatment)
Limited insurance coverage
Preparation requirements: (blood draw, processing)
Inconsistent results: (20-80% response rates)
Multiple injections: often needed
*Best candidates:* Tendon injuries, early osteoarthritis, athletes, failed conventional treatment
When Peptides Excel: Optimal Use Cases
Primary Indications:
1. Chronic tendon/ligament pain unresponsive to conventional treatment
2. Multiple joint involvement where systemic approach beneficial
3. Athletes requiring rapid return to high-level activity
4. Individuals intolerant of NSAIDs or steroids
5. Prevention-focused protocols for high-risk activities
6. Post-surgical healing enhancement
Peptide Advantages:
Regenerative focus: rather than symptom suppression
Excellent safety profile: with proper protocols
Systemic benefits: beyond targeted joint
Combination potential: with other treatments
Self-administration: convenience
Dose customization: based on response
Integration Strategies:
Peptides often work best as part of comprehensive treatment plans:
*Phase 1 (Acute):* NSAIDs for immediate relief + peptide initiation
*Phase 2 (Subacute):* Peptide continuation + physical therapy
*Phase 3 (Chronic):* Peptide maintenance + exercise progression
*Phase 4 (Prevention):* Periodic peptide cycles + lifestyle optimization
What's Coming Next: Future Research Directions
Ongoing Clinical Trials
The peptide research landscape for joint health continues expanding, with several promising developments in the pipeline:
BPC-157 Human Trials:
*Phase II Tendon Repair Study (Croatia):*
Population: 120 patients with chronic Achilles tendinopathy
Design: Randomized, double-blind, placebo-controlled
Intervention: BPC-157 250 μg vs 500 μg vs placebo, 8-week treatment
Primary endpoint: Ultrasound-measured tendon healing at 12 weeks
Expected completion: Late 2026
Significance: First large-scale human efficacy trial
*Osteoarthritis Prevention Trial (Germany):*
Population: 200 individuals with early knee cartilage damage
Design: Multicenter, randomized controlled trial
Intervention: Intra-articular BPC-157 vs hyaluronic acid vs placebo
Duration: 12-month treatment with 2-year follow-up
Endpoints: MRI cartilage volume, pain scores, functional outcomes
Innovation: First prevention-focused peptide trial
TB-500 Clinical Development:
*Veterinary to Human Translation:*
Given TB-500's extensive veterinary data, researchers are developing protocols for human application:
Safety studies: Phase I dose-escalation in healthy volunteers (ongoing)
Efficacy trials: Phase II planning for tendon injuries
Regulatory pathway: FDA breakthrough therapy designation being pursued
Emerging Peptide Candidates
GHK-Cu (Copper Peptide) Combinations:
Researchers are investigating synergistic effects of copper-binding peptides with traditional healing compounds:
Mechanism: Enhanced collagen synthesis and antioxidant effects
Applications: Cartilage preservation, skin-joint interface healing
Status: Preclinical studies showing 30-40% enhanced healing when combined with BPC-157
Pentosan Polysulfate Peptide Conjugates:
Novel compounds linking proven joint-protective molecules with peptide delivery systems:
Advantage: Targeted delivery to cartilage tissue
Development: Early preclinical testing
Potential: Oral bioavailability with injectable efficacy
Stem Cell-Derived Peptide Factors:
Isolation of specific healing factors from mesenchymal stem cell cultures:
Approach: Identify and synthesize the most potent healing peptides
Benefits: Potentially more powerful than current options
Timeline: 3-5 years to clinical application
Technological Advances
Improved Delivery Systems:
*Sustained-Release Formulations:*
Hydrogel matrices: 7-14 day release profiles reducing injection frequency
Microsphere encapsulation: Monthly dosing protocols in development
Implantable devices: 3-6 month continuous delivery systems
*Targeted Delivery Methods:*
Magnetic targeting: Using magnetic nanoparticles to direct peptides to specific joints
Ultrasound enhancement: Improved tissue penetration with focused ultrasound
Iontophoresis: Electrical enhancement of transdermal peptide delivery
Personalized Medicine Applications:
*Genetic Testing Integration:*
Researchers are identifying genetic markers that predict peptide response:
Collagen synthesis genes: COL1A1, COL3A1 variants affecting healing speed
Growth factor receptors: VEGFR2, EGFR polymorphisms influencing efficacy
Inflammatory pathways: IL-1β, TNF-α gene variants determining optimal protocols
*Biomarker-Guided Dosing:*
Development of blood/urine tests to optimize individual treatment:
Inflammatory markers: Real-time adjustment based on cytokine levels
Healing indicators: Collagen breakdown products guiding treatment duration
Safety monitoring: Early detection of adverse responses
Regulatory Landscape Evolution
FDA Pathway Development:
The regulatory approach to peptide therapies is evolving:
Expedited review: Breakthrough therapy designation for regenerative peptides
Combination products: Guidance for peptide + device combinations
Biomarker qualification: Acceptance of novel endpoints for approval
International Harmonization:
European Medicines Agency: Parallel development of peptide guidelines
Japanese PMDA: Accelerated approval pathways for regenerative therapies
Global standards: International Conference on Harmonisation peptide guidelines
Unanswered Research Questions
Optimal Treatment Duration:
Current gap: Most studies last 4-12 weeks, but optimal cycle length unknown
Research needed: Long-term safety and efficacy studies
Clinical relevance: Determining maintenance protocols vs. intermittent treatment
Combination Synergies:
Multiple peptides: Which combinations provide additive vs. synergistic benefits?
Conventional integration: How to optimally combine peptides with physical therapy, surgery, medications?
Sequencing: Does treatment order affect outcomes?
Individual Response Prediction:
Responder identification: Why do 20-30% of patients show minimal benefit?
Dose optimization: How to determine individual optimal dosing?
Timing factors: Do age, injury chronicity, or activity level affect protocols?
Mechanism Clarification:
Receptor specificity: Which receptors mediate which effects?
Tissue selectivity: Why do some tissues respond better than others?
Systemic effects: How do local injections create systemic benefits?
Long-term Outcomes:
Durability: How long do benefits persist after treatment completion?
Re-injury prevention: Do peptides reduce future injury risk?
Quality of healing: Is peptide-enhanced tissue functionally equivalent to natural healing?
These research directions suggest that peptide therapy for joint pain will continue evolving rapidly, with improved formulations, personalized protocols, and expanded applications likely within the next 5-10 years.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Joint Pain Peptide Therapy Essentials
• BPC-157 and TB-500 represent the most researched and effective peptides for joint pain, with complementary mechanisms that enhance healing when used together
• Optimal dosing typically involves BPC-157 at 500 μg daily and TB-500 at 5 mg twice weekly for 6-8 week cycles, with local injection providing superior results for targeted joint issues
• Scientific evidence demonstrates 60-85% improvement rates in tendon healing, cartilage preservation, and pain reduction compared to 30-50% with conventional treatments
• Safety profiles are excellent with proper protocols, showing minimal side effects compared to NSAIDs or corticosteroids, though injection site reactions occur in 15-25% of users
• Combination protocols with growth hormone support or anti-inflammatory stacks can provide enhanced benefits for severe conditions or competitive athletes
• Cost considerations range from $200-500 monthly, often proving cost-effective compared to repeated medical procedures or long-term conventional treatments
• Treatment timeline typically shows initial improvements in 1-2 weeks, significant pain reduction by 3-4 weeks, and functional improvements continuing through 6-8 weeks
• Best candidates include those with chronic tendon/ligament pain, multiple joint involvement, NSAID intolerance, or desire for regenerative rather than symptomatic treatment
• Future developments include sustained-release formulations, personalized dosing based on genetic markers, and combination products currently in clinical trials
• Integration approach works best when peptides are combined with appropriate physical therapy, nutrition optimization, and lifestyle modifications for comprehensive joint health
Related Articles on BuyPeptidesOnline.com
Best Anti-Aging Peptides | Buy Online | Complete Age Reversal Guide 2026
GHK-Cu vs Matrixyl | Buy Online | Best Anti-Aging Peptide 2026
Best Anxiety Peptides | Buy Online | Natural Calming Compounds 2026
Semaglutide vs Tirzepatide | Buy Online | Best Peptide for Diabetes Management