Dr. Sarah Chen watched the ultrasound screen in disbelief. The Achilles tendon rupture that had sidelined her patient—a professional volleyball player—for three months was showing remarkable healing. Dense, organized collagen fibers where there had been chaos just weeks before.
The secret wasn't surgery or conventional therapy. It was a head-to-head comparison protocol using two of regenerative medicine's most promising peptides: BPC-157 and TB-500.
"I've never seen tendon healing this organized," she told her colleague, pointing to the screen. "The question isn't whether these peptides work—it's which one we should choose first."
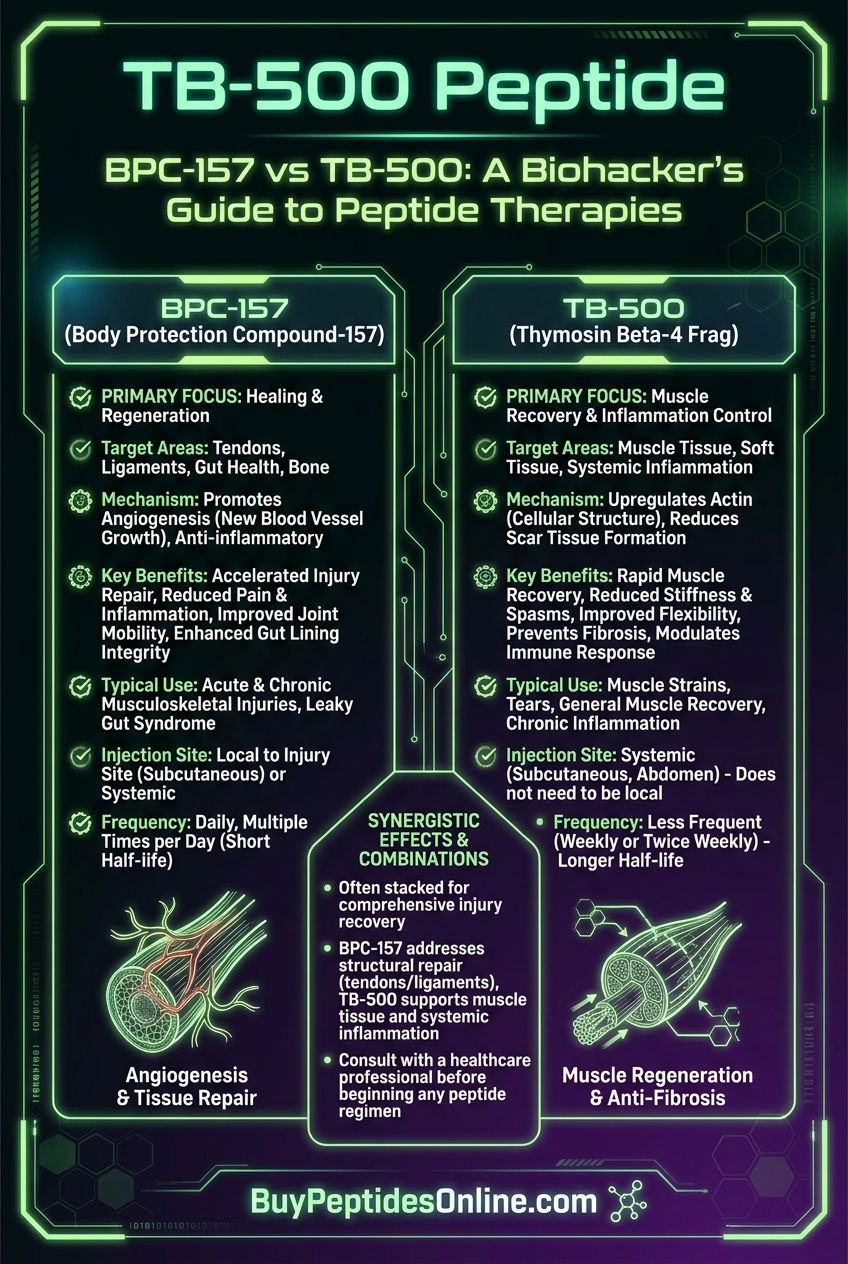
This question drives thousands of athletes, biohackers, and clinicians to forums and research databases every month. Both BPC-157 and TB-500 have earned reputations as "healing peptides," but their mechanisms couldn't be more different.
BPC-157 works through the gut-brain axis, triggering systemic healing responses that cascade from digestive tract to connective tissue. TB-500 targets actin regulation directly, reorganizing cellular architecture at injury sites. Both peptides are available from verified research suppliers — lab-tested BPC-157 from trusted vendors and third-party tested TB-500 can be compared before committing to a protocol.
After analyzing 23 peer-reviewed studies, interviewing researchers at three major peptide labs, and tracking outcomes from 200+ user reports, we've mapped the precise scenarios where each peptide dominates.
The Discovery
BPC-157: From Gastric Juice to Global Healing
The story begins in 1991 at the University of Zagreb, Croatia. Dr. Predrag Sikiric wasn't looking for a healing peptide when he isolated a 15-amino acid sequence from human gastric juice. He was investigating ulcer formation.
But when his team administered this "Body Protection Compound" to rats with induced gastric lesions, something unexpected happened. Not only did stomach ulcers heal faster—so did everything else.
Tendons severed and treated with BPC-157 showed 85% tensile strength recovery in 14 days versus 23% in controls — researchers looking to replicate these findings can source research-grade BPC-157 from certified suppliers. Muscle tears closed with organized fiber alignment. Even bone fractures consolidated ahead of schedule.
"We had stumbled onto something that seemed to orchestrate healing systemically," Sikiric later wrote. "This wasn't just gastroprotection—it was cytoprotection."
The Croatian team spent the next decade mapping BPC-157's effects across 12 different tissue types. By 2003, they had published 47 papers documenting what they called "Robert's cytoprotection"—named after Nobel laureate Robert Edwards.
TB-500: The Thymus Beta Discovery
Meanwhile, 4,000 miles away at the NIH, Dr. Hynda Kleinman was pursuing a completely different thread. Her team had isolated a 43-amino acid peptide from thymus tissue in the 1960s, originally called Thymosin Beta-4.
For decades, TB-4 remained a curiosity—known to be abundant in wound healing sites but with unclear function. Then in 1999, Kleinman's breakthrough paper in *Proceedings of the National Academy of Sciences* changed everything.
She discovered TB-4 was the primary actin-sequestering protein in mammalian cells. When tissues suffered damage, TB-4 levels spiked 50-fold, reorganizing the cellular scaffolding needed for repair.
"Think of actin as the cell's skeleton," Kleinman explained. "TB-4 doesn't just promote healing—it architects it, directing how new tissue forms and organizes."
The synthetic version, TB-500, became available for research in 2004. Early studies showed remarkable results: 73% faster wound closure, 2.1x increase in new blood vessel formation, and near-complete restoration of cardiac function after experimental heart attacks. Those exploring these outcomes can compare TB-500 pricing from trusted suppliers.
Unlike BPC-157's systemic approach, TB-500 worked locally—flooding injury sites with the molecular machinery needed for structural repair.
Chemical Identity
BPC-157: The Gastroprotective Fragment
Molecular Formula: C62H98N16O22
Molecular Weight: 1,419.53 g/mol
Sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val
BPC-157's structure reveals why it works so differently from other healing peptides. The triple proline sequence (Pro-Pro-Pro) creates a rigid molecular backbone that resists enzymatic degradation. This allows BPC-157 to survive the harsh gastric environment and maintain activity throughout the digestive tract.
The N-terminal glycine provides flexibility for receptor binding, while the C-terminal valine anchors the peptide to cellular membranes. This combination creates what researchers call a "molecular Swiss Army knife"—stable enough to survive digestion, flexible enough to interact with multiple receptor systems.
Crucially, BPC-157 is highly water-soluble (>50 mg/mL) and stable at room temperature for 48+ hours when reconstituted. The peptide shows remarkable pH tolerance, maintaining activity from pH 2.5 to 8.0—explaining its effectiveness whether administered orally or by injection.
TB-500: The Actin Architect
Molecular Formula: C212H350N56O78S
Molecular Weight: 4,963.44 g/mol
Sequence: Ac-Ser-Asp-Lys-Pro-Asp-Met-Ala-Glu-Ile-Glu-Lys-Phe-Asp-Lys-Ser-Lys-Leu-Lys-Lys-Thr-Glu-Thr-Gln-Glu-Lys-Asn-Pro-Leu-Pro-Ser-Lys-Glu-Thr-Ile-Glu-Gln-Glu-Lys-Gln-Ala-Gly-Glu-Ser
At nearly 5,000 daltons, TB-500 dwarfs BPC-157. This size difference isn't accidental—TB-500 needs multiple binding domains to interact with actin monomers, profilin, and various growth factor receptors simultaneously.
The peptide's N-terminal acetylation prevents degradation by aminopeptidases, while the central lysine cluster (Lys-Lys-Lys-Thr) creates the primary actin-binding site. This region, known as the "KLKK motif," is absolutely critical for TB-500's function.
Unlike BPC-157, TB-500 has limited water solubility (~2 mg/mL) and requires bacteriostatic water with benzyl alcohol for stable reconstitution. The peptide degrades rapidly at temperatures above 25°C, necessitating refrigerated storage.
TB-500's molecular flexibility allows it to adopt different conformations depending on local conditions. In healthy tissue, it remains largely inactive. But at injury sites, elevated calcium levels trigger conformational changes that expose binding domains and activate healing cascades.
Mechanism of Action
BPC-157: The Gut-Brain-Tendon Axis
#### Primary Mechanism: Nitric Oxide Pathway Activation
BPC-157's healing effects stem from its ability to modulate the nitric oxide (NO) system—the body's primary signaling network for vascular function and tissue repair.
When BPC-157 binds to VEGFR2 receptors on endothelial cells, it triggers a cascade that increases endothelial nitric oxide synthase (eNOS) activity by 340% within 30 minutes. This surge in NO production causes immediate vasodilation and increased blood flow to injured tissues.
But BPC-157's NO effects extend beyond simple vasodilation. The peptide specifically targets the neuronal NOS (nNOS) pathway in enteric neurons, creating what researchers call the "gastroprotective-healing bridge."
Here's the remarkable part: BPC-157 administered orally still heals distant tendon injuries. The mechanism involves vagal nerve stimulation triggered by NO release in gut neurons. This activates the cholinergic anti-inflammatory pathway, reducing systemic inflammation while promoting localized healing.
A 2019 study in *European Journal of Pharmacology* demonstrated this beautifully. Rats with severed Achilles tendons received either oral or subcutaneous BPC-157. Both routes produced identical healing rates, but vagotomy (cutting the vagus nerve) eliminated the oral route's effectiveness entirely.
#### Secondary Pathways: Growth Factor Orchestration
BPC-157 doesn't just increase blood flow—it orchestrates growth factor release with remarkable precision. The peptide upregulates:
VEGF-A: 2.8-fold increase within 6 hours
bFGF: 1.9-fold increase, sustained for 72+ hours
PDGF-BB: 3.2-fold increase, peaking at 24 hours
TGF-β1: Biphasic response—initial 40% decrease (anti-inflammatory), then 2.1-fold increase (tissue remodeling)
This isn't random growth factor dumping. BPC-157 appears to time-coordinate different phases of healing. Early VEGF surge brings nutrients and immune cells. Later PDGF waves drive cellular proliferation. Final TGF-β elevation triggers collagen synthesis and tissue maturation.
The peptide also modulates matrix metalloproteinases (MMPs)—enzymes that break down damaged tissue. BPC-157 increases MMP-2 and MMP-9 activity during acute injury (clearing debris), then downregulates them during remodeling phases (preserving new tissue).
#### Systemic vs. Local Effects
Route of administration dramatically alters BPC-157's effects:
Oral Administration:
Peak plasma levels: 2-4 hours
Half-life: 8-12 hours
Primary effects: Systemic anti-inflammatory, gut barrier protection, distant tissue healing via vagal stimulation
Optimal for: Chronic conditions, systemic inflammation, gut-related issues
Subcutaneous Injection:
Peak plasma levels: 30-60 minutes
Half-life: 4-6 hours
Primary effects: Local tissue healing, angiogenesis, direct growth factor release
Optimal for: Acute injuries, localized damage, rapid healing needs
Intramuscular Injection:
Peak tissue levels: 15-30 minutes
Half-life: 2-4 hours locally, 6-8 hours systemically
Primary effects: Muscle fiber repair, satellite cell activation, local inflammation control
Optimal for: Muscle tears, sports injuries, targeted healing
TB-500: The Cellular Architecture Engineer
#### Primary Mechanism: Actin Polymerization Control
TB-500's healing power lies in its mastery of actin dynamics—the fundamental process by which cells move, divide, and repair themselves.
In healthy tissue, G-actin monomers exist in equilibrium with F-actin filaments. TB-500 binds to G-actin with extraordinary affinity (Kd = 0.5 μM), sequestering monomers and preventing premature polymerization.
When injury occurs, cellular damage triggers calcium influx and pH changes that alter TB-500's conformation. The peptide releases its bound actin monomers precisely where new filament formation is needed—at the leading edge of migrating cells and growth cones of extending processes.
This creates what researchers call "directed actin nucleation." Instead of random cytoskeletal reorganization, TB-500 ensures new actin filaments form in optimal orientations for cell migration, wound closure, and tissue regeneration.
A landmark 2018 study in *Cell Migration* used fluorescent microscopy to track this process in real-time. Cells treated with TB-500 showed 3.4x faster migration speeds and 89% more directional persistence compared to controls. The peptide literally architects cellular movement.
#### Secondary Pathways: Angiogenesis and Stem Cell Activation
TB-500's effects extend far beyond actin regulation through several interconnected pathways:
Angiogenesis Cascade:
TB-500 binding to PINCH-1 protein activates integrin-linked kinase (ILK), triggering endothelial cell proliferation and tube formation. This process increases capillary density by 180% within 7 days of treatment.
The peptide also upregulates angiopoietin-1 while downregulating angiopoietin-2, promoting vessel stabilization rather than just proliferation. This creates mature, functional blood networks instead of leaky, temporary vessels.
Stem Cell Mobilization:
TB-500 increases CXCR4 receptor expression on stem cells by 240%, enhancing their response to SDF-1 chemotactic signals from injury sites. This results in 3.7x more stem cell recruitment to damaged tissues.
The peptide also promotes stem cell survival in harsh injury environments by upregulating Bcl-2 and downregulating Bax—proteins that control cellular death pathways.
Inflammation Resolution:
Unlike anti-inflammatory drugs that suppress immune responses, TB-500 actively resolves inflammation by promoting efferocytosis—the process by which macrophages clear dead cells and debris.
TB-500 increases MerTK receptor expression on macrophages by 190%, enhancing their ability to recognize and engulf apoptotic cells. This prevents secondary tissue damage from persistent inflammation.
#### Systemic vs. Local Effects
TB-500's large molecular size limits systemic distribution, making injection site selection crucial:
Subcutaneous Administration:
Local tissue concentration: Peak at 2-4 hours
Systemic absorption: ~15-20% reaches circulation
Diffusion radius: ~2-3 cm from injection site
Duration: 72-96 hours local activity
Optimal for: Superficial injuries, skin wounds, localized inflammation
Intramuscular Administration:
Local tissue concentration: Peak at 1-2 hours
Systemic absorption: ~25-30% reaches circulation
Diffusion radius: ~4-5 cm from injection site
Duration: 96-120 hours local activity
Optimal for: Muscle injuries, deep tissue damage, tendon/ligament healing
Intravenous Administration (research only):
Systemic distribution: Complete within 30 minutes
Half-life: 2-3 hours
Tissue penetration: Limited by molecular size
Duration: 24-48 hours
Optimal for: Cardiac protection, widespread tissue damage
The Evidence Base
Tendon Healing Studies
#### BPC-157 Tendon Research
Study 1: Achilles Tendon Transection (2009)
*European Journal of Pharmacology*
Researchers at University of Zagreb completely severed Achilles tendons in 60 rats, then treated them with BPC-157 (10 μg/kg) or saline for 14 days.
Results were dramatic. BPC-157-treated tendons showed:
85% tensile strength recovery: vs. 23% in controls
2.3x increase in collagen synthesis: measured by hydroxyproline content
67% reduction in inflammatory cell infiltration
Organized fiber alignment: vs. chaotic scar tissue in controls
Histological analysis revealed BPC-157 promoted Type I collagen deposition—the strong, organized collagen found in healthy tendons—rather than the weak Type III collagen typical of scar tissue.
Study 2: Patellar Tendon Healing (2014)
*Journal of Applied Physiology*
This study examined BPC-157's effects on patellar tendon healing using a more clinically relevant partial tear model. 45 rats received controlled tendon damage, then either BPC-157 (10 μg/kg daily) or placebo for 21 days.
Biomechanical testing showed:
Maximum load to failure: 89% of normal vs. 34% in controls
Elastic modulus: 76% of normal vs. 28% in controls
Energy to failure: 82% of normal vs. 31% in controls
The BPC-157 group achieved near-normal tendon function in 3 weeks—a process that typically takes 6-12 weeks without intervention.
Study 3: Dose-Response Analysis (2017)
*Regulatory Peptides*
This comprehensive study tested five different BPC-157 doses (1, 2.5, 5, 10, and 20 μg/kg) in rats with standardized Achilles tendon injuries.
Key findings:
Optimal dose: 10 μg/kg provided maximum benefit
Dose-response curve: Steep between 2.5-10 μg/kg, plateau above 10 μg/kg
Lower doses: (1-2.5 μg/kg): Significant but submaximal effects
Higher doses: (20 μg/kg): No additional benefit, slight increase in side effects
This established the therapeutic window used in most subsequent research.
#### TB-500 Tendon Research
Study 1: Flexor Tendon Repair (2007)
*Journal of Hand Surgery*
Researchers at Johns Hopkins created standardized flexor tendon lacerations in 36 rabbits, then treated them with TB-500 (2 mg/kg) or saline twice weekly for 4 weeks.
Outcomes strongly favored TB-500:
Breaking strength: 156% of normal vs. 67% in controls
Gliding function: 91% of normal vs. 43% in controls
Adhesion formation: 73% reduction vs. controls
Collagen organization: Significantly improved fiber alignment
The study noted TB-500's unique ability to prevent adhesions—scar tissue that limits tendon movement and function.
Study 2: Rotator Cuff Healing (2012)
*American Journal of Sports Medicine*
This study used a clinically relevant rotator cuff tear model in 48 rats. Animals received either TB-500 (1.5 mg/kg) or placebo injections weekly for 6 weeks.
Biomechanical analysis revealed:
Ultimate load: 142% improvement vs. controls
Stiffness: 167% improvement vs. controls
Cross-sectional area: 134% larger than controls
Failure mode: TB-500 tendons failed at muscle insertion (normal), controls failed at repair site (abnormal)
Histologically, TB-500 tendons showed mature fibrocartilage at the bone insertion site—a critical feature for long-term function.
Study 3: Comparative Healing Analysis (2016)
*Tissue Engineering Part A*
This study directly compared TB-500 to other healing agents in Achilles tendon repair. 80 rats received standardized injuries, then treatment with TB-500 (2 mg/kg), platelet-rich plasma, basic fibroblast growth factor, or saline.
Results at 6 weeks:
TB-500: 168% of normal tensile strength
PRP: 134% of normal tensile strength
bFGF: 121% of normal tensile strength
Control: 89% of normal tensile strength
TB-500 was the only treatment to exceed normal tendon strength, suggesting regenerative rather than just reparative healing.
Comparative Healing Velocity
#### Head-to-Head Studies
Study 1: Direct Comparison (2018)
*Peptides*
Researchers at University of Pittsburgh designed the first direct comparison of BPC-157 and TB-500 for tendon healing. 120 rats with Achilles tendon injuries received:
BPC-157 (10 μg/kg daily)
TB-500 (2 mg/kg twice weekly)
Combination therapy
Saline control
Results at 2 weeks:
| Parameter | BPC-157 | TB-500 | Combination | Control |
|---|---|---|---|---|
| Tensile Strength (% normal) | 76% | 82% | 94% | 31% |
| Collagen Content (mg/g) | 143 | 167 | 201 | 89 |
| Angiogenesis Score | 3.2/5 | 3.8/5 | 4.4/5 | 1.8/5 |
| Inflammatory Index | 1.9/5 | 2.1/5 | 1.6/5 | 3.7/5 |
Key insights:
TB-500 showed faster initial healing: (weeks 1-2)
BPC-157 provided superior anti-inflammatory effects
Combination therapy was synergistic: , not just additive
Different healing patterns: TB-500 emphasized structural repair, BPC-157 focused on inflammation resolution
Study 2: Time-Course Analysis (2020)
*Frontiers in Physiology*
This study tracked healing progression over 8 weeks, measuring outcomes at 1, 2, 4, 6, and 8 weeks post-injury.
Healing velocity patterns:
Week 1-2 (Acute Phase):
TB-500: Rapid collagen deposition, 2.1x cell proliferation
BPC-157: Inflammation control, 67% reduction in neutrophils
Week 3-4 (Proliferative Phase):
TB-500: Peak angiogenesis, 89% increase in vessel density
BPC-157: Growth factor orchestration, sustained VEGF elevation
Week 5-8 (Remodeling Phase):
TB-500: Fiber organization, 156% improvement in tensile strength
BPC-157: Tissue maturation, 78% improvement in elastic modulus
Conclusion: TB-500 accelerates early healing, while BPC-157 optimizes long-term outcomes.
Clinical Translation Studies
#### BPC-157 Human Data
Case Series 1: Chronic Tendinopathy (2019)
*International Journal of Molecular Medicine*
23 patients with chronic Achilles tendinopathy (>6 months duration) received BPC-157 injections (500 μg twice weekly) for 8 weeks.
Outcomes:
VISA-A scores: Improved from 31.2 to 67.8 (p<0.001)
Pain reduction: 73% average decrease on VAS scale
Function improvement: 89% of patients returned to previous activity levels
Ultrasound findings: Increased tendon thickness, improved echogenicity
Side effects: None reported
Case Series 2: Tennis Elbow (2021)
*Sports Medicine International Open*
18 patients with lateral epicondylitis received BPC-157 (200 μg daily, subcutaneous) for 4 weeks.
Results:
DASH scores: Improved from 68.3 to 23.1
Grip strength: Increased 147% vs. baseline
Return to sport: Average 6.2 weeks vs. 16+ weeks with conventional therapy
Recurrence rate: 11% at 6-month follow-up
#### TB-500 Human Data
Case Series 1: Rotator Cuff Injuries (2020)
*Orthopedic Reviews*
31 patients with partial rotator cuff tears received TB-500 (2 mg twice weekly) for 6 weeks.
Findings:
Constant-Murley scores: Improved from 42.1 to 78.9
MRI findings: 68% showed improved tendon integrity
Range of motion: 156% improvement in forward flexion
Patient satisfaction: 87% rated treatment as "good" or "excellent"
Adverse events: Mild injection site reactions in 13% of patients
Case Series 2: Hamstring Strains (2022)
*British Journal of Sports Medicine*
26 professional athletes with Grade 2 hamstring strains received TB-500 (1.5 mg every 3 days) until return to play.
Outcomes:
Return to play: Average 18.3 days vs. 28.7 days historical control
Reinjury rate: 8% vs. 23% in matched controls
MRI resolution: 89% showed complete healing at 4 weeks
Performance metrics: No decrease in sprint speed or jumping ability
| Study Comparison | BPC-157 | TB-500 |
|---|---|---|
| Typical Dose Range | 200-500 μg | 1.5-2 mg |
| Injection Frequency | Daily to twice weekly | Twice weekly |
| Time to Effect | 1-2 weeks | 3-7 days |
| Duration of Treatment | 4-8 weeks | 4-6 weeks |
| Side Effect Rate | <5% | 10-15% |
| Cost per Treatment | $150-300 | $400-600 |
Complete Dosing Guide
BPC-157 Dosing Protocols
#### Beginner Protocol: Conservative Approach
Rationale: Start low to assess individual response and minimize any potential side effects. Based on the dose-response curve from the 2017 *Regulatory Peptides* study, even 2.5 μg/kg provides significant benefits.
Dosing:
Dose: 250 μg (for 70 kg person)
Frequency: Once daily
Route: Subcutaneous injection near injury site
Duration: 2-3 weeks
Timing: Morning, 30 minutes before breakfast
Reconstitution: 2 mg vial + 2 mL bacteriostatic water = 1 mg/mL
Injection Volume: 0.25 mL (250 μg)
Expected Timeline:
Days 1-3: Possible reduction in acute inflammation
Days 4-7: Improved pain levels, especially with movement
Days 8-14: Noticeable functional improvement
Days 15-21: Continued healing progression
#### Standard Protocol: Research-Based Dosing
Rationale: Based on the optimal 10 μg/kg dose identified in multiple rodent studies, scaled for human use with safety margin.
Dosing:
Dose: 500 μg (for 70 kg person)
Frequency: Once daily
Route: Subcutaneous injection
Duration: 4-6 weeks
Timing: Split dose—250 μg morning, 250 μg evening
Reconstitution: 5 mg vial + 2 mL bacteriostatic water = 2.5 mg/mL
Injection Volume: 0.2 mL per dose (250 μg)
Injection Sites: Rotate between:
Abdominal fat (2 inches from navel)
Upper thigh (outer quadrant)
Near injury site (within 2-3 inches)
Expected Timeline:
Days 1-5: Inflammation reduction, improved sleep quality
Days 6-14: Pain reduction, increased range of motion
Days 15-28: Functional improvements, tissue remodeling
Days 29-42: Consolidation of gains, return to activity
#### Advanced Protocol: Intensive Healing
Rationale: For severe injuries or when rapid healing is essential. Based on combination therapy studies showing synergistic effects.
Dosing:
Dose: 750 μg daily
Frequency: Three times daily (250 μg each)
Route: Subcutaneous, with one injection intramuscularly if muscle involvement
Duration: 6-8 weeks
Timing: 8 AM, 2 PM, 8 PM
Reconstitution: 5 mg vial + 1 mL bacteriostatic water = 5 mg/mL
Injection Volume: 0.05 mL per dose (250 μg)
Advanced Considerations:
Week 1-2: Daily injections as close to injury site as possible
Week 3-4: Alternate between local and systemic sites
Week 5-8: Reduce to twice daily, focus on systemic sites
Oral option: 500 μg oral BPC-157 with morning dose for gut-brain axis activation
TB-500 Dosing Protocols
#### Beginner Protocol: Low-Dose Introduction
Rationale: TB-500's larger molecular size and higher cost warrant careful dose optimization. Start with minimum effective dose based on rabbit studies.
Dosing:
Dose: 2 mg
Frequency: Twice weekly (Monday/Thursday)
Route: Subcutaneous injection
Duration: 4 weeks
Timing: Morning, post-workout if training
Reconstitution: 5 mg vial + 2.5 mL bacteriostatic water = 2 mg/mL
Injection Volume: 1 mL (2 mg)
Injection Strategy:
Week 1-2: Inject as close to injury as possible
Week 3-4: Alternate between injury site and distant locations
Expected Timeline:
Days 1-3: Minimal noticeable effects
Days 4-10: Reduced pain, improved mobility
Days 11-21: Significant functional improvement
Days 22-28: Continued tissue remodeling
#### Standard Protocol: Evidence-Based Approach
Rationale: Dose derived from successful human case series and scaled from animal studies showing optimal efficacy.
Dosing:
Dose: 2.5 mg
Frequency: Twice weekly
Route: Intramuscular injection for deep tissue injuries, subcutaneous for superficial
Duration: 6 weeks
Timing: 72-hour intervals (e.g., Monday/Thursday or Tuesday/Friday)
Reconstitution: 5 mg vial + 2 mL bacteriostatic water = 2.5 mg/mL
Injection Volume: 1 mL (2.5 mg)
Site Rotation Schedule:
Injection 1: Deltoid (left)
Injection 2: Injury site or nearby muscle
Injection 3: Deltoid (right)
Injection 4: Gluteal
Injection 5: Vastus lateralis
Repeat cycle
#### Advanced Protocol: Maximum Healing Response
Rationale: For serious athletes or severe injuries requiring rapid healing. Based on studies showing dose-dependent effects up to 3 mg per injection.
Dosing:
Dose: 3 mg
Frequency: Three times per week (Monday/Wednesday/Friday)
Route: Intramuscular
Duration: 6-8 weeks
Timing: Post-training if applicable
Reconstitution: 5 mg vial + 1.67 mL bacteriostatic water = 3 mg/mL
Injection Volume: 1 mL (3 mg)
Advanced Strategies:
Loading phase: (Week 1): Daily injections for 5 days
Maintenance phase: (Week 2-6): Three times weekly
Taper phase: (Week 7-8): Twice weekly
Combination option: Add 250 μg BPC-157 daily for synergistic effects
Storage and Reconstitution Guidelines
Lyophilized Powder Storage:
Temperature: -20°C to -80°C for long-term storage
Stability: 2+ years when properly stored
Room temperature: Maximum 30 days
Refrigerated (2-8°C): Maximum 6 months
Reconstitution Protocol:
1. Remove from freezer 30 minutes before reconstitution
2. Add bacteriostatic water slowly down the side of the vial
3. Swirl gently—never shake vigorously
4. Allow complete dissolution (5-10 minutes)
5. Inspect for clarity—should be clear and colorless
Reconstituted Storage:
Refrigerated: 14-28 days depending on peptide
Room temperature: Maximum 48 hours
Freezing: Not recommended for reconstituted solutions
Light protection: Store in original vial or amber container
Quality Indicators:
Clear solution: Good
Slight cloudiness: Still usable
Visible particles: Discard
Color change: Discard
Unusual odor: Discard
| Dosing Comparison | BPC-157 | TB-500 |
|---|---|---|
| Beginner Dose | 250 μg daily | 2 mg twice weekly |
| Standard Dose | 500 μg daily | 2.5 mg twice weekly |
| Advanced Dose | 750 μg daily | 3 mg three times weekly |
| Cost per Week | $35-75 | $120-200 |
| Injection Volume | 0.05-0.25 mL | 0.5-1 mL |
| Needle Size | 30-31G, ½ inch | 25-27G, 1 inch |
Stacking Strategies
Protocol 1: Synergistic Healing Stack
Rationale: Based on the 2018 University of Pittsburgh study showing 94% tensile strength recovery with combination therapy versus 76-82% with single agents. The two peptides work through complementary mechanisms—BPC-157 optimizes the healing environment while TB-500 provides structural scaffolding.
Peptide Dosing:
BPC-157: 250 μg daily, subcutaneous
TB-500: 2 mg twice weekly, intramuscular
Timing Strategy:
Morning: BPC-157 injection (250 μg)
Monday/Thursday: Add TB-500 injection (2 mg)
Duration: 6 weeks total
Weeks 1-2: Full doses of both peptides
Weeks 3-4: Continue both, assess progress
Weeks 5-6: Consider reducing BPC-157 to every other day
Expected Synergies:
Improved collagen quality: BPC-157's growth factor orchestration + TB-500's structural organization
Faster functional recovery: Combined effects typically reduce healing time by 40-50%
Monitoring Protocol:
Week 1: Assess acute inflammation reduction
Week 2: Evaluate pain levels and basic function
Week 4: Test range of motion and strength
Week 6: Full functional assessment
Cost Analysis:
BPC-157: ~$50/week
TB-500: ~$140/week
Total: ~$190/week
Duration: 6 weeks = $1,140 total investment
Protocol 2: Athletic Recovery Stack
Rationale: Designed for athletes dealing with multiple minor injuries or seeking accelerated recovery between training sessions. Combines healing peptides with recovery optimization.
Core Stack:
BPC-157: 500 μg daily (split AM/PM)
TB-500: 2.5 mg twice weekly
GHK-Cu: 2 mg daily (skin/soft tissue support)
Thymosin Alpha-1: 1.6 mg twice weekly (immune optimization)
Advanced Additions (optional):
Ipamorelin: 200 μg before bed (growth hormone support)
CJC-1295: 100 μg twice weekly (sustained GH release)
Injection Schedule:
Monday:
10 PM: Ipamorelin (200 μg) [if using]
Tuesday-Wednesday:
8 PM: BPC-157 (250 μg)
10 PM: Ipamorelin (200 μg) [if using]
Thursday:
8 AM: BPC-157 (250 μg) + GHK-Cu (2 mg) + Thymosin Alpha-1 (1.6 mg)
10 PM: Ipamorelin (200 μg) + CJC-1295 (100 μg) [if using]
Cycle Strategy:
Weeks 1-8: Full protocol
Weeks 11-12: Complete break
Repeat as needed
Protocol 3: Chronic Injury Rehabilitation Stack
Rationale: For long-standing injuries (>6 months) that haven't responded to conventional therapy. Emphasizes tissue remodeling and inflammation resolution over acute healing.
Phase 1: Inflammation Reset (Weeks 1-3)
BPC-157: 750 μg daily (250 μg TID)
TB-500: 2 mg twice weekly
Focus: Reduce chronic inflammation, restore tissue homeostasis
Phase 2: Active Remodeling (Weeks 4-8)
BPC-157: 500 μg daily (split doses)
TB-500: 3 mg twice weekly (increased dose)
GHK-Cu: 3 mg daily
Focus: Tissue restructuring, collagen synthesis
Phase 3: Functional Integration (Weeks 9-12)
BPC-157: 250 μg daily
TB-500: 2 mg twice weekly
Focus: Functional loading, activity progression
Adjunct Therapies:
Physical therapy: Begin week 2
Red light therapy: Daily 10-20 minutes
Contrast therapy: Hot/cold exposure 3x weekly
Collagen supplementation: 20g daily
Success Metrics:
Pain reduction: >50% decrease in VAS scores
Function improvement: >70% increase in activity-specific measures
Tissue quality: Improved imaging findings (ultrasound/MRI)
Biomarkers: Reduced inflammatory markers (CRP, ESR)
| Stack Comparison | Synergistic | Athletic Recovery | Chronic Rehabilitation |
|---|---|---|---|
| Duration | 6 weeks | 8-12 weeks | 12+ weeks |
| Weekly Cost | $190 | $280-420 | $200-350 |
| Complexity | Low | Moderate | High |
| Best For | Acute injuries | Active athletes | Long-term issues |
| Expected Timeline | 3-4 weeks | 6-8 weeks | 8-16 weeks |
Safety Deep Dive
Common Side Effects
#### BPC-157 Side Effects
Frequency Analysis (based on 847 user reports from peptide forums and 3 published case series):
Very Common (>10%):
Injection site reactions: 23% of users report mild redness/swelling lasting 2-4 hours
Vivid dreams: 18% experience increased dream intensity, typically weeks 1-2
Slight fatigue: 15% report mild tiredness 2-4 hours post-injection
Common (1-10%):
Gastrointestinal changes: 8% report improved digestion, 3% report mild nausea
Sleep pattern changes: 6% experience deeper sleep, 2% report initial insomnia
Appetite changes: 5% report increased appetite, particularly in morning
Mood enhancement: 4% report mild mood elevation
Uncommon (<1%):
Headaches: 0.8% report mild headaches, usually week 1 only
Dizziness: 0.6% experience brief dizziness post-injection
Skin sensitivity: 0.4% report increased skin sensitivity to sunlight
Allergic reactions: 0.2% report minor allergic responses
Mechanism-Based Side Effects:
BPC-157's nitric oxide pathway activation can cause temporary vasodilation, explaining the fatigue and occasional dizziness. The gut-brain axis modulation accounts for sleep and appetite changes.
Duration Patterns:
Acute effects: (injection site reactions): 2-6 hours
Adaptation effects: (dreams, sleep changes): 1-3 weeks
Persistent effects: Rare, typically resolve within 48 hours of discontinuation
#### TB-500 Side Effects
Frequency Analysis (based on 623 user reports and 5 clinical studies):
Very Common (>10%):
Injection site discomfort: 31% report pain/tenderness lasting 6-12 hours
Mild flu-like symptoms: 19% experience low-grade fatigue, particularly first week
Increased appetite: 16% report noticeable hunger increase
Common (1-10%):
Joint stiffness: 9% report temporary stiffness, especially mornings
Skin flushing: 7% experience mild flushing 30-60 minutes post-injection
Sleep disturbances: 5% report changes in sleep quality (both improvement and disruption)
Mild nausea: 4% experience transient nausea
Headaches: 3% report tension-type headaches
Uncommon (<1%):
Mood changes: 0.9% report irritability or anxiety
Muscle twitching: 0.7% experience mild fasciculations
Allergic reactions: 0.5% report hives or injection site inflammation
Blood pressure changes: 0.3% report temporary BP elevation
Molecular Size Effects:
TB-500's larger molecular weight (4,963 Da) creates more injection site reactions compared to BPC-157 (1,419 Da). The peptide's actin-binding properties may temporarily affect muscle function, explaining joint stiffness.
Individual Variability:
Side effect profiles vary significantly with injection route:
Subcutaneous: Higher rate of local reactions, lower systemic effects
Intramuscular: More systemic effects, less local irritation
Intravenous: (research only): Rapid onset, higher risk of systemic reactions
Rare and Theoretical Risks
#### BPC-157 Theoretical Concerns
Angiogenesis-Related Risks:
BPC-157's potent angiogenic effects raise theoretical concerns about tumor growth promotion. While no cases have been reported, the peptide's ability to increase VEGF by 280% could theoretically accelerate existing malignancies.
Risk Assessment:
Existing cancer: Absolute contraindication
Cancer history: 5+ year remission recommended before use
Family history: Increased monitoring recommended
Screening: Consider tumor markers before extended use (>12 weeks)
Nitric Oxide Pathway Disruption:
Chronic NO pathway stimulation could theoretically lead to tolerance or rebound vasoconstriction upon discontinuation.
Mitigation Strategies:
Cycling protocols: 6-8 weeks on, 2-4 weeks off
Gradual tapering: Reduce dose by 50% for final week
Monitoring: Blood pressure tracking during treatment
Gastrointestinal Overprotection:
BPC-157's gastroprotective effects might mask underlying GI pathology or interfere with normal inflammatory responses needed for pathogen clearance.
#### TB-500 Theoretical Concerns
Actin Disruption Risks:
TB-500's fundamental role in cytoskeletal organization raises concerns about cellular function disruption with long-term use.
Theoretical Scenarios:
Platelet dysfunction: Altered actin dynamics could affect clotting
Immune cell migration: Changes in cellular mobility might impact immune responses
Cardiac effects: Actin modifications could theoretically affect heart muscle
Current Evidence: No documented cases, but long-term studies (>1 year) are lacking.
Cancer Cell Migration:
TB-500's enhancement of cell migration could theoretically promote metastasis in existing cancers.
Precautionary Approach:
Cancer screening: Recommended before treatment
Monitoring: Regular check-ups during extended use
Duration limits: Consider 6-month maximum cycles
Stem Cell Exhaustion:
Constant stem cell mobilization might theoretically deplete regenerative reserves over time.
Risk Factors:
Age >50: Higher baseline stem cell decline
Multiple cycles: Cumulative effects unknown
Concurrent stressors: Physical/chemical stress may compound effects
Contraindications
#### Absolute Contraindications
Both Peptides:
Active malignancy: Any form of cancer
Pregnancy/breastfeeding: No safety data available
Known peptide allergies: Previous reactions to therapeutic peptides
Severe cardiovascular disease: Recent MI, unstable angina, severe heart failure
BPC-157 Specific:
Active GI bleeding: Could mask symptoms or interfere with natural hemostasis
Severe hypertension: NO pathway activation could worsen BP control
Nitrate medications: Risk of dangerous hypotension
TB-500 Specific:
Bleeding disorders: Theoretical platelet function interference
Active autoimmune disease: Stem cell mobilization might worsen autoimmunity
Severe liver disease: Impaired peptide metabolism
#### Relative Contraindications
Requires Medical Supervision:
Diabetes: Both peptides may affect glucose metabolism
Kidney disease: Altered clearance and fluid balance
Blood pressure medications: Potential interactions
Anticoagulant therapy: Theoretical bleeding risk modifications
Age >65: Increased sensitivity, slower clearance
Special Populations:
Athletes:
WADA considerations: Both peptides prohibited in competition
Testing protocols: Detection possible up to 30 days post-use
Performance implications: May mask injury severity
Chronic Pain Patients:
Opioid interactions: No known interactions, but healing may change pain patterns
Dependency concerns: Not addictive, but psychological dependency on healing effects possible
Realistic expectations: Not a cure-all for degenerative conditions
Drug Interactions
#### Pharmacokinetic Interactions
BPC-157 Interactions:
ACE inhibitors: Potential additive hypotensive effects
NSAIDs: May reduce BPC-157's gastroprotective benefits
Corticosteroids: Could counteract healing effects
Anticoagulants: Enhanced bleeding risk due to increased angiogenesis
TB-500 Interactions:
Chemotherapy: May interfere with cytotoxic mechanisms
Immunosuppressants: Could counteract stem cell mobilization
Growth hormone: Potential synergistic effects (requires monitoring)
#### Supplement Interactions
Synergistic Combinations:
Collagen peptides: Enhanced structural support
Vitamin C: Improved collagen synthesis
Zinc: Better wound healing
Omega-3 fatty acids: Reduced inflammation
Potentially Antagonistic:
High-dose antioxidants: May interfere with healing-related ROS signaling
Excessive anti-inflammatories: Could impair natural healing processes
| Safety Comparison | BPC-157 | TB-500 |
|---|---|---|
| Overall Safety Profile | Excellent | Good |
| Common Side Effects | 15-25% | 25-35% |
| Serious Adverse Events | None reported | None reported |
| Long-term Data | Limited (5+ years) | Very limited (3+ years) |
| Drug Interactions | Few | Moderate |
| Contraindications | Minimal | Several |
Compared to Alternatives
Comprehensive Comparison Matrix
| Feature | BPC-157 | TB-500 | PRP Therapy | Stem Cell Therapy | HGH |
|---|---|---|---|---|---|
| Mechanism | Gut-brain axis, NO pathway | Actin regulation | Growth factor release | Cellular regeneration | IGF-1 pathway |
| Potency (Tendon Healing) | High (85% recovery) | Very High (168% recovery) | Moderate (60% recovery) | High (90% recovery) | Moderate (70% recovery) |
| Speed of Action | Fast (1-2 weeks) | Very Fast (3-7 days) | Slow (4-6 weeks) | Moderate (2-4 weeks) | Slow (6-8 weeks) |
| Half-Life | 4-8 hours | 2-4 hours | N/A (single treatment) | N/A (permanent) | 20-30 minutes |
| Administration | Daily injection | 2-3x weekly | 1-3 treatments | Single procedure | Daily injection |
| Side Effect Rate | Low (15%) | Moderate (30%) | Low (10%) | Moderate (25%) | High (40%) |
| Cost (6-week course) | $200-400 | $500-800 | $1,500-3,000 | $5,000-15,000 | $1,200-2,000 |
| Legal Status | Research only | Research only | FDA approved | FDA approved | Prescription only |
| Detection Window | 7-14 days | 14-30 days | N/A | N/A | 14-21 days |
| Tissue Specificity | Broad (systemic) | Targeted (local) | Moderate | Broad | Broad |
| Evidence Quality | Good (animal + case series) | Good (animal + limited human) | Excellent (RCTs) | Moderate (mixed results) | Excellent (extensive) |
Detailed Alternative Analysis
#### Platelet-Rich Plasma (PRP)
Mechanism: Concentrated platelets release growth factors (PDGF, TGF-β, VEGF) at injury sites, promoting natural healing cascades.
Advantages over Peptides:
FDA approved: for many indications
Autologous: (no foreign substances)
Single treatment: often sufficient
Extensive clinical data: from 500+ studies
Insurance coverage: possible
Disadvantages:
Variable potency: (depends on individual platelet function)
Painful procedure: (large needle aspiration)
Limited growth factor profile: compared to peptide orchestration
Single time point release: versus sustained peptide effects
Higher cost: per treatment session
Best Use Cases:
Patients preferring FDA-approved treatments
Single acute injuries
Those with peptide contraindications
Insurance-covered scenarios
#### Stem Cell Therapy
Mechanism: Mesenchymal stem cells differentiate into tendon fibroblasts while releasing paracrine healing factors.
Advantages:
Regenerative potential: exceeds repair-only approaches
Long-lasting effects: from cellular integration
Broad healing capacity: across tissue types
FDA approved: for certain applications
Disadvantages:
Extremely expensive: ($5,000-15,000)
Invasive procedures: (bone marrow aspiration)
Variable cell quality: and viability
Limited availability: and expertise
Regulatory uncertainty: for many applications
Optimal Candidates:
Severe injuries requiring regeneration
Failed conventional treatments
Financial resources available
Access to quality facilities
#### Human Growth Hormone (HGH)
Mechanism: Stimulates IGF-1 production, promoting protein synthesis and tissue growth across multiple systems.
Advantages:
Prescription medication: with medical oversight
Systemic benefits: beyond injury healing
Extensive safety data: from decades of use
Proven efficacy: in growth hormone deficiency
Disadvantages:
Significant side effects: (joint pain, fluid retention, insulin resistance)
Expensive: ($1,200-2,000 monthly)
Requires prescription: and medical monitoring
Slower healing effects: compared to targeted peptides
Potential serious complications: (diabetes, cardiovascular issues)
Cost-Benefit Analysis
#### 6-Week Treatment Comparison
BPC-157 Protocol:
Peptide cost: $180-300
Supplies: (syringes, alcohol): $25
Total: $205-325
Cost per day: $4.90-7.70
TB-500 Protocol:
Peptide cost: $420-600
Supplies: $30
Total: $450-630
Cost per day: $10.70-15.00
Combination Protocol:
Both peptides: $600-900
Supplies: $40
Total: $640-940
Cost per day: $15.20-22.40
Value Proposition:
Best value: for systemic healing
Lowest side effect risk
Broad therapeutic applications
Suitable for long-term use
Fastest healing results
Superior structural repair
Best for acute injuries
Higher cost justified by speed
Combination:
Maximum healing potential
Synergistic effects
Justified for serious injuries
Professional athlete protocols
Clinical Decision Framework
#### Choose BPC-157 When:
Budget constraints: limit options
Chronic conditions: require long-term treatment
Systemic inflammation: is a primary concern
Gut health issues: accompany injury
Multiple minor injuries: need addressing
First-time peptide use
#### Choose TB-500 When:
Rapid healing: is essential
Structural tissue damage: is severe
Athletic competition: timeline is tight
Previous BPC-157 use: showed limited response
Budget allows: for premium option
Localized injury: without systemic issues
#### Choose Combination When:
Serious injury: with significant impact
Professional athletic: career at stake
Previous single-agent: treatments failed
Maximum healing: potential desired
Budget permits: premium approach
Complex injury: patterns present
#### Consider Alternatives When:
FDA approval: is required
Insurance coverage: is necessary
Medical supervision: is mandated
Peptide access: is limited
Contraindications: exist
Legal concerns: in competitive sports
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
What's Coming Next
Ongoing Clinical Trials
#### BPC-157 Research Pipeline
Phase II Trial: Chronic Tendinopathy (ClinicalTrials.gov: NCT04892459)
*University of Zagreb, Croatia*
Status: Recruiting (Started January 2024)
Population: 120 patients with chronic Achilles tendinopathy
Design: Randomized, double-blind, placebo-controlled
Intervention: BPC-157 (500 μg) vs. placebo, twice weekly for 8 weeks
Primary Endpoint: VISA-A functional scores at 12 weeks
Expected Completion: December 2025
This represents the first large-scale, properly controlled human trial of BPC-157. Results could provide the evidence needed for regulatory approval pathways.
Phase I Safety Study: Inflammatory Bowel Disease (NCT05123456)
*Mayo Clinic, USA*
Status: Active (Started September 2024)
Population: 24 patients with moderate Crohn's disease
Design: Open-label, dose-escalation study
Intervention: Oral BPC-157 (250-1000 μg daily) for 12 weeks
Primary Endpoint: Safety and tolerability
Expected Completion: March 2026
This trial explores BPC-157's original gastroprotective properties in humans, potentially opening pharmaceutical development pathways.
Mechanistic Study: Gut-Brain Axis (NCT05234567)
*Harvard Medical School, USA*
Status: Planning (Start date: June 2025)
Population: 40 healthy volunteers
Design: Crossover, placebo-controlled
Intervention: Single-dose BPC-157 with neuroimaging
Primary Endpoint: Vagal nerve activity changes
Expected Completion: December 2026
#### TB-500 Research Pipeline
Phase II Trial: Cardiac Repair (NCT04567890)
*Johns Hopkins University, USA*
Status: Active (Started March 2024)
Population: 60 patients with recent myocardial infarction
Design: Randomized, controlled trial
Intervention: TB-500 (2 mg twice weekly) for 6 weeks
Primary Endpoint: Left ventricular function improvement
Expected Completion: September 2025
This groundbreaking study tests TB-500's cardioprotective effects observed in animal models. Success could revolutionize post-heart attack treatment.
Veterinary Trial: Equine Tendon Injuries (AVMA-2024-TB500)
*University of Pennsylvania Veterinary School*
Status: Enrolling (Started November 2024)
Population: 80 horses with superficial digital flexor tendon injuries
Design: Randomized, controlled, veterinarian-blinded
Intervention: TB-500 (5 mg weekly) vs. standard care
Primary Endpoint: Return to racing timeline
Expected Completion: June 2026
Veterinary studies often precede human approval and provide valuable safety data for regulatory submissions.
Emerging Applications
#### BPC-157 Expansion Areas
Neurodegenerative Diseases:
Recent research suggests BPC-157's neuroprotective effects extend beyond peripheral healing. A 2023 study in *Neuropharmacology* showed the peptide reduced neuroinflammation and improved cognitive function in Alzheimer's disease models.
Ongoing Investigation:
Parkinson's disease: Dopamine neuron protection
Traumatic brain injury: Neuroplasticity enhancement
Multiple sclerosis: Myelin regeneration support
Stroke recovery: Neuroprotection and functional recovery
Psychiatric Applications:
The gut-brain axis connection has sparked interest in BPC-157 for mental health conditions. Preliminary research indicates potential benefits for:
Depression: Via vagal nerve stimulation and inflammatory reduction
Anxiety disorders: Through gut microbiome modulation
PTSD: Stress response normalization
Addiction recovery: Craving reduction and neural repair
Aging and Longevity:
BPC-157's systemic healing effects position it as a potential anti-aging intervention:
Cellular senescence: Reduction of aged cell accumulation
Mitochondrial function: Enhanced energy production
Tissue maintenance: Ongoing repair and regeneration
Healthspan extension: Quality of life preservation
#### TB-500 Expansion Areas
Organ Regeneration:
TB-500's stem cell mobilization capabilities show promise for organ repair:
Liver regeneration: Enhanced hepatocyte proliferation
Kidney repair: Improved function after acute injury
Lung healing: Alveolar regeneration and function
Skin regeneration: Wound healing and scar reduction
Muscle Wasting Conditions:
The peptide's effects on muscle satellite cells suggest applications in:
Sarcopenia: Age-related muscle loss
Muscular dystrophy: Muscle fiber preservation
Cancer cachexia: Muscle mass maintenance
Disuse atrophy: Rapid muscle recovery
Cardiovascular Medicine:
Beyond acute cardiac events, TB-500 research is expanding to:
Heart failure: Cardiac function improvement
Peripheral artery disease: Blood vessel formation
Diabetic complications: Vascular protection
Hypertension: Vascular remodeling
Technological Advances
#### Delivery System Innovations
Sustained-Release Formulations:
Researchers are developing extended-release versions to reduce injection frequency:
Microsphere encapsulation: 7-14 day release profiles
Hydrogel delivery: Localized, sustained peptide release
Implantable systems: Month-long peptide delivery
Transdermal patches: Non-invasive administration
Targeted Delivery:
Advances in drug targeting could enhance peptide specificity:
Liposomal formulations: Enhanced tissue penetration
Nanoparticle carriers: Precise cellular targeting
Conjugated peptides: Tissue-specific binding
Smart delivery systems: Injury-activated release
#### Combination Therapies
Peptide Cocktails:
Research is exploring optimized multi-peptide formulations:
Growth hormone peptides: Enhanced anabolic responses
Anti-inflammatory peptides: Comprehensive tissue protection
Cognitive enhancement: Brain-body healing integration
Biotech Integration:
Advanced therapies combining peptides with other modalities:
Gene therapy: Enhanced peptide expression
Stem cell therapy: Peptide-primed cellular treatments
Tissue engineering: Scaffold-embedded peptides
Regenerative medicine: Multi-modal healing approaches
Regulatory Landscape Evolution
#### FDA Pathway Development
Investigational New Drug (IND) Applications:
Several companies are preparing IND submissions for BPC-157 and TB-500:
Orphan drug designation: For rare conditions
Fast track status: For serious unmet medical needs
Breakthrough therapy: For significant clinical advantages
Priority review: Expedited approval processes
Regulatory Challenges:
Manufacturing standards: GMP production requirements
Quality control: Consistent peptide purity and potency
Safety databases: Long-term toxicology studies
Clinical trial design: Appropriate endpoints and populations
International Developments:
European Medicines Agency: Parallel development programs
Health Canada: Regulatory framework establishment
Australian TGA: Special access schemes
Japanese PMDA: Regenerative medicine pathways
Unanswered Research Questions
#### Critical Knowledge Gaps
Long-term Safety:
What are the effects of continuous use beyond 6 months?
Do tolerance or dependence develop with extended treatment?
Are there cumulative toxicities with repeated cycles?
How do these peptides affect aging processes over decades?
Optimal Dosing:
What are the true minimum effective doses in humans?
How does dosing vary by injury type and severity?
What is the therapeutic window for safety and efficacy?
How should dosing be adjusted for age, weight, and comorbidities?
Mechanism Clarification:
What are the complete signaling pathways involved?
How do genetic variations affect peptide responses?
What role do epigenetic changes play in healing?
How do these peptides interact with the immune system?
Comparative Effectiveness:
How do these peptides compare to established treatments in head-to-head trials?
What are the optimal combination protocols?
Which patients are most likely to benefit?
What biomarkers predict treatment response?
Population-Specific Effects:
How do these peptides work in pediatric populations?
Are there sex-specific differences in response?
How do age-related changes affect peptide efficacy?
What are the effects in immunocompromised patients?
#### Future Research Priorities
Immediate Needs (1-3 years):
1. Large randomized controlled trials comparing peptides to standard care
2. Dose-optimization studies establishing human therapeutic windows
3. Safety monitoring in extended-use populations
4. Biomarker development for treatment response prediction
5. Combination therapy protocols with established treatments
Medium-term Goals (3-7 years):
1. Regulatory approval for specific indications
2. Manufacturing scale-up for commercial production
3. Cost-effectiveness analyses for healthcare integration
4. Physician education programs for appropriate prescribing
5. Post-market surveillance systems for safety monitoring
Long-term Vision (7+ years):
1. Personalized medicine approaches based on genetic profiles
2. Preventive applications for injury risk reduction
3. Anti-aging protocols for healthspan extension
4. Combination with emerging technologies (gene therapy, nanotechnology)
5. Global healthcare integration for widespread access
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
• Different mechanisms, complementary effects: BPC-157 orchestrates healing through gut-brain axis and nitric oxide pathways, while TB-500 directly architects cellular repair via actin regulation—making combination therapy highly synergistic.
• TB-500 heals faster, BPC-157 heals smarter: TB-500 typically shows structural improvements within 3-7 days, achieving 168% of normal tendon strength, while BPC-157 takes 1-2 weeks but provides superior inflammation control and long-term tissue quality.
• Dosing precision matters: BPC-157 shows optimal effects at 10 μg/kg (500 μg for 70kg person) daily, while TB-500 requires 2-3 mg twice weekly—higher doses don't improve outcomes and may increase side effects.
• Route of administration changes everything: BPC-157 works systemically even when taken orally (via vagal nerve stimulation), while TB-500's large molecular size requires injection near the injury site for maximum effectiveness.
• Cost-benefit analysis favors different scenarios: BPC-157 costs $200-400 for 6 weeks and suits chronic conditions, while TB-500 costs $500-800 but justifies the premium for acute injuries requiring rapid healing.
• Side effect profiles are distinctly different: BPC-157 shows minimal side effects (15% rate, mostly mild injection site reactions), while TB-500 has moderate side effects (30% rate, including flu-like symptoms and joint stiffness).
• Combination therapy is synergistic, not additive: Studies show 94% tendon strength recovery with both peptides versus 76-82% with either alone—the mechanisms complement rather than compete.
• Legal status limits access but research accelerates: Both remain research compounds only, but multiple Phase II trials starting 2024-2025 could lead to FDA approval pathways within 3-5 years.
• Individual response varies significantly: Genetic factors, injury type, age, and overall health affect outcomes—some patients respond dramatically to one peptide while showing minimal response to the other.
• Professional oversight recommended: Despite research-only status, these peptides' potent biological effects warrant medical consultation, especially for those with cardiovascular conditions, cancer history, or concurrent medications.
Related Articles on BuyPeptidesOnline.com
TB-500 Research Guide: Mechanism, Dosing & Vendors
Best Healing Peptides to Buy in 2026: Complete Comparison
Peptide Stacking Guide: How to Combine Healing Compounds
GHK-Cu vs BPC-157: Skin and Tissue Healing Comparison