The 72-year-old man walked into Dr. Allan Goldstein's lab at George Washington University in 1977, his immune system ravaged by chemotherapy. T-cell counts barely detectable. Infections recurring weekly. Traditional medicine had reached its limits.
Goldstein injected him with **thymosin alpha-1** — available from verified research suppliers, a 28-amino acid peptide his team had painstakingly isolated from calf thymus glands. Within weeks, the patient's T-cell populations rebounded. Infections cleared. The immune system, thought permanently damaged, had regenerated.
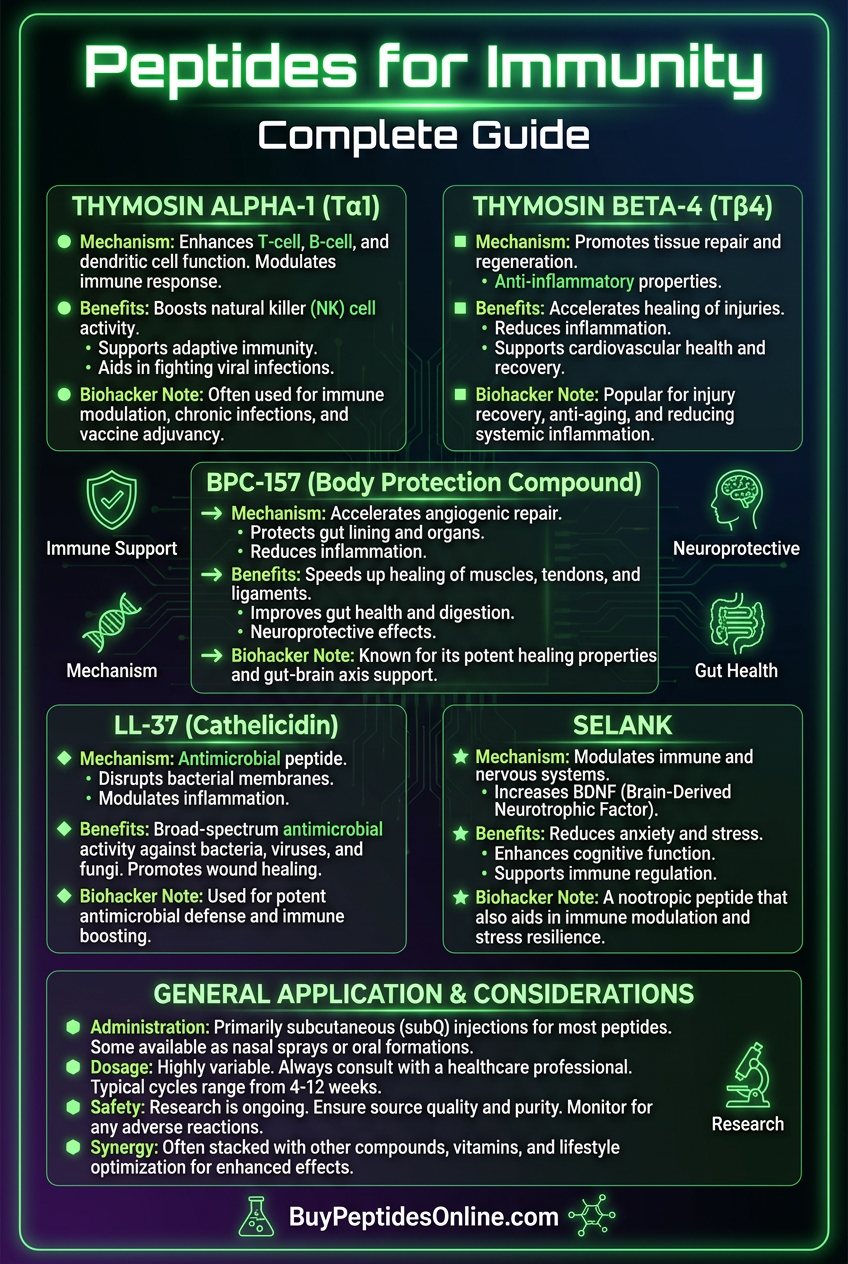
That breakthrough launched the modern era of immunomodulatory peptides—compounds that don't just suppress or stimulate immunity, but intelligently rebalance it. Today, researchers have identified dozens of peptides that can enhance immune surveillance, accelerate pathogen clearance, and restore homeostasis to dysregulated immune systems.
The Discovery: How Scientists Unlocked Immune Peptides
The hunt for immune-enhancing peptides began in the 1960s when researchers noticed that children born without thymus glands suffered catastrophic immune deficiencies. The thymus, they realized, wasn't just producing T-cells—it was secreting factors that educated and activated the entire adaptive immune system.
Allan Goldstein and his colleague Abraham White at Albert Einstein College began the painstaking process of isolating these "thymic factors" in 1966. They processed thousands of pounds of calf thymus tissue, using primitive chromatography techniques to separate dozens of bioactive compounds.
The breakthrough came when they isolated thymosin fraction 5, a mixture of peptides that could restore immune function in thymectomized mice. Further purification revealed individual peptides, with thymosin alpha-1 emerging as the most potent immunomodulator.
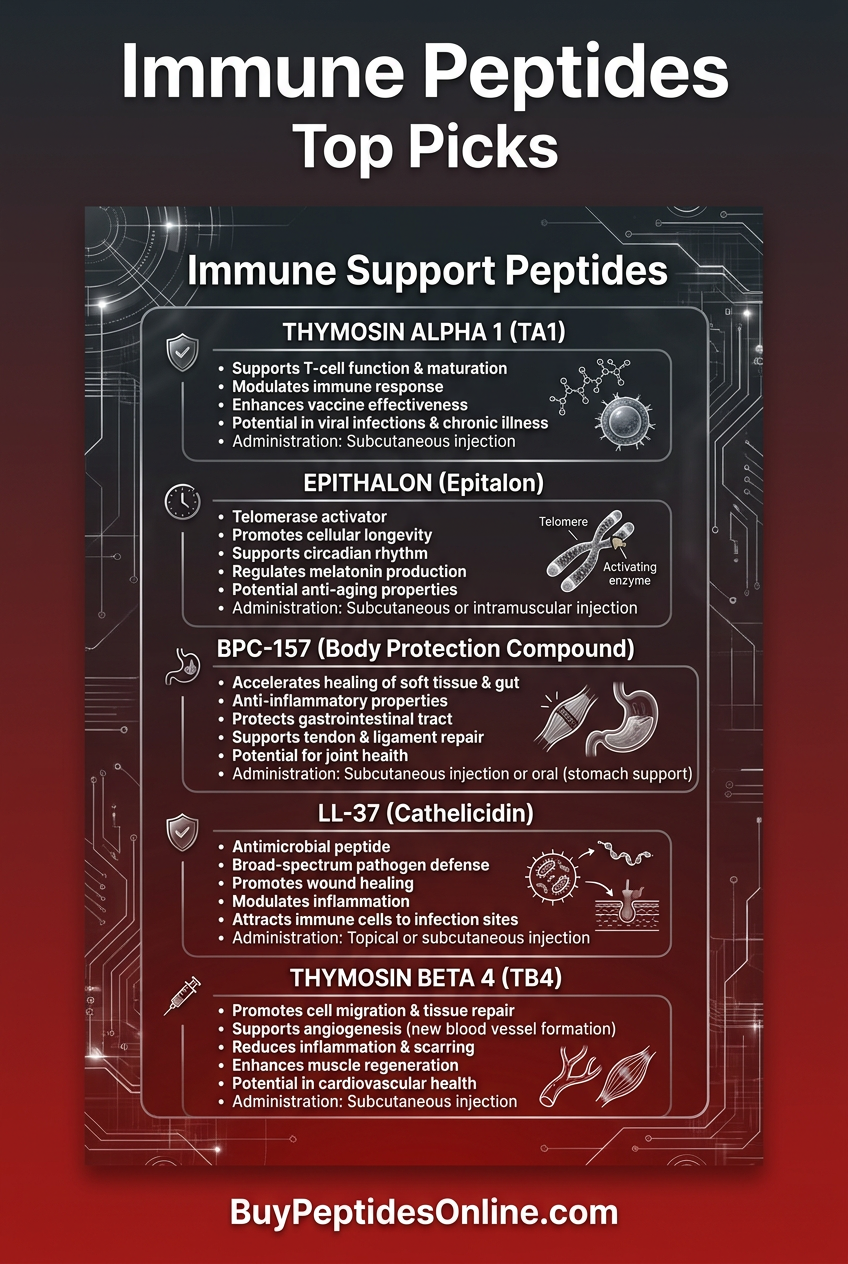
Meanwhile, researchers at other institutions were discovering immune peptides from unexpected sources. **LL-37**, the only cathelicidin antimicrobial peptide in humans, was identified in 1995 from neutrophil granules — explore lab-tested LL-37 from trusted suppliers. **Epithalon emerged from Russian longevity research in the 1980s. Selank** was developed at the Institute of Molecular Genetics as an anxiolytic that unexpectedly showed profound immune effects.
By the 2000s, scientists realized that immune peptides weren't rare exceptions—they were fundamental signaling molecules that orchestrated both innate and adaptive immunity. The human genome encodes over 100 antimicrobial peptides alone, with many more immunomodulatory sequences hidden in larger proteins.
Chemical Identity: The Molecular Architecture of Immune Peptides
Immune support peptides share several key structural features that enable their biological activity. Most are cationic (positively charged), allowing them to interact with negatively charged pathogen surfaces and cell membranes. They typically range from 10-50 amino acids, making them large enough to maintain specific receptor binding while remaining small enough for efficient tissue penetration.
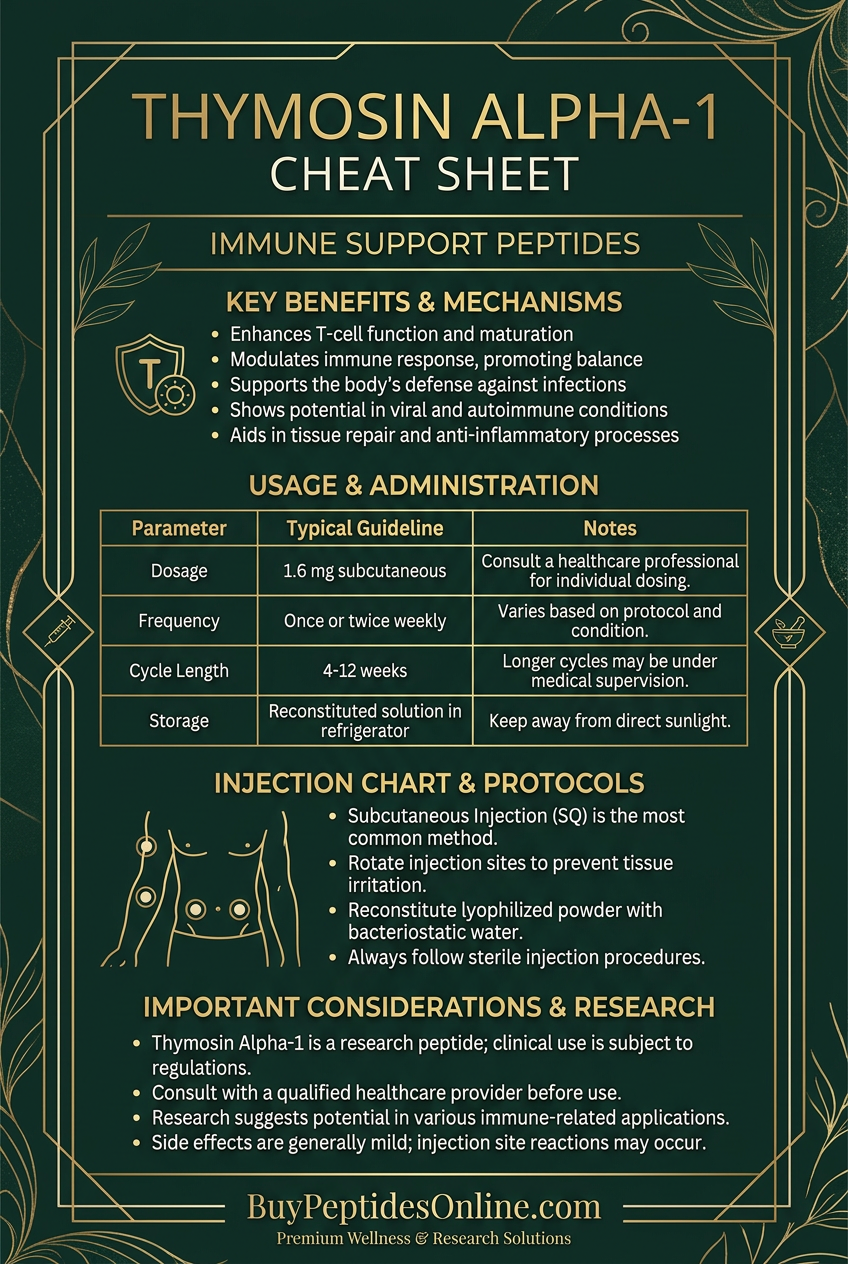
Thymosin alpha-1 (Tα1) exemplifies this architecture. With a molecular weight of 3,108 Da and the sequence Ac-SDAAVDTSSEITTKDLKEKKEVVEEAEN-NH2, it contains multiple lysine residues that create positive charge clusters. The N-terminal acetylation and C-terminal amidation protect against enzymatic degradation, extending its half-life to approximately 2 hours in circulation.
LL-37 represents a different structural class—the cathelicidin antimicrobials. Its 37-amino acid sequence (LLGDFFRKSKEKIGKEFKRIVQRIKDFLRNLVPRTES) forms an amphipathic α-helix, with hydrophobic residues on one face and cationic residues on the other. This structure allows it to insert into microbial membranes while remaining stable in human tissues.
Epithalon (Ala-Glu-Asp-Gly) is remarkably simple—just four amino acids with a molecular weight of 390 Da (compare Epithalon pricing from third-party tested vendors). Despite its small size, it demonstrates exceptional stability and bioavailability, likely due to its resemblance to endogenous neuropeptides.
Solubility varies significantly among immune peptides. Thymosin alpha-1 is highly water-soluble (>10 mg/mL), making it suitable for subcutaneous injection. LL-37 shows moderate solubility but can aggregate at high concentrations. Selank (Thr-Lys-Pro-Arg-Pro-Gly-Pro) maintains excellent aqueous stability due to its proline residues, which provide conformational flexibility.
Storage requirements reflect their peptide nature. Most immune peptides require refrigeration (2-8°C) in lyophilized form and freezing (-20°C) once reconstituted. **BPC-157**, while primarily known for healing, also shows immune effects and demonstrates unusual stability at room temperature for up to 24 hours.
Mechanism of Action: How Immune Peptides Restore Balance
Primary Mechanism: T-Cell Education and Activation
The fundamental mechanism underlying most immune peptides involves T-lymphocyte modulation. Thymosin alpha-1 binds to Toll-like receptor 9 (TLR9) on dendritic cells, triggering a cascade that enhances antigen presentation and T-cell activation.
The pathway begins when Tα1 binds TLR9 in endosomal compartments. This activates MyD88-dependent signaling, leading to nuclear factor-κB (NF-κB) translocation and increased production of interleukin-12 (IL-12) and interferon-α (IFN-α). These cytokines polarize naive T-cells toward Th1 responses, enhancing cellular immunity against intracellular pathogens and tumor cells.
Simultaneously, Tα1 directly binds T-lymphocytes through an unknown receptor mechanism, increasing CD4+ T-helper cell proliferation and CD8+ cytotoxic T-lymphocyte activity. Studies show 2-3 fold increases in T-cell proliferation within 48 hours of administration.
Natural killer (NK) cell activation represents another primary pathway. Thymosin alpha-1 increases NK cell cytotoxicity by up to 400% through enhanced perforin and granzyme B release. This mechanism proves particularly important for anti-tumor immunity and viral clearance.
Secondary Pathways: Antimicrobial and Anti-Inflammatory Effects
LL-37 operates through direct antimicrobial mechanisms alongside immune modulation. Its cationic amphipathic structure allows it to insert into bacterial cell membranes, creating pores that lead to osmotic lysis. Minimum inhibitory concentrations range from 2-32 μg/mL against common pathogens including *Staphylococcus aureus*, *Escherichia coli*, and *Candida albicans*.
Beyond direct antimicrobial activity, LL-37 functions as a damage-associated molecular pattern (DAMP), binding to P2X7 purinergic receptors on immune cells. This triggers NLRP3 inflammasome activation, leading to IL-1β and IL-18 release—cytokines that recruit and activate neutrophils and macrophages.
Paradoxically, LL-37 also demonstrates anti-inflammatory effects at higher concentrations by binding lipopolysaccharide (LPS) and neutralizing its pro-inflammatory activity. This dual function allows it to eliminate pathogens while preventing excessive inflammation.
Epithalon works through telomerase activation and circadian rhythm normalization. It binds to an unidentified receptor that increases telomerase reverse transcriptase (TERT) expression, extending T-cell replicative lifespan. Additionally, it normalizes melatonin production, which indirectly supports immune function through improved sleep and reduced oxidative stress.
Systemic vs. Local Effects: Route-Dependent Outcomes
Subcutaneous injection of immune peptides produces systemic effects within 2-6 hours. Thymosin alpha-1 administered subcutaneously achieves peak plasma concentrations of 10-50 ng/mL, sufficient for T-cell activation throughout lymphoid organs. This route proves optimal for chronic viral infections, immunodeficiency states, and cancer immunotherapy.
Intranasal administration targets mucosal immunity more directly. LL-37 delivered intranasally concentrates in nasal-associated lymphoid tissue (NALT), producing local antimicrobial effects while minimizing systemic exposure. Studies show 10-fold higher concentrations in nasal secretions compared to plasma.
Oral administration faces significant bioavailability challenges due to peptide degradation. However, some immune peptides like Selank demonstrate oral activity through peptide transporter 1 (PEPT1) uptake in intestinal epithelium. Oral bioavailability typically ranges from 5-15% for most immune peptides.
Topical application proves effective for localized immune enhancement. LL-37 formulated in penetration-enhancing vehicles can achieve therapeutic concentrations in skin and wound tissues, supporting local antimicrobial defense without systemic effects.
The Evidence Base: Clinical Validation Across Applications
Viral Infections: Enhanced Clearance and Reduced Severity
Thymosin alpha-1's antiviral efficacy has been extensively documented across multiple viral pathogens. A randomized controlled trial of 1,050 severe acute respiratory syndrome (SARS) patients showed that Tα1 treatment (1.6 mg twice daily for 5 days) reduced mortality from 12.9% to 3.6% compared to standard care alone (Li et al., *Chest*, 2004).
The mechanism involves enhanced type I interferon production and CD8+ T-cell responses. Patients receiving Tα1 showed 3-fold higher interferon-γ levels and faster viral clearance, with median time to negative PCR reduced from 8.5 to 5.2 days.
In chronic hepatitis B, a meta-analysis of 18 trials encompassing 1,665 patients demonstrated that Tα1 combination therapy increased HBeAg seroconversion rates from 23% to 41% compared to interferon monotherapy (Shi et al., *World Journal of Gastroenterology*, 2014). Sustained virological response improved from 18% to 36% at 6-month follow-up.
Epithalon showed promising results in a Russian study of 266 elderly patients with recurrent respiratory infections. Daily administration of 10 mg for 10 days reduced infection frequency by 67% over the following year, with enhanced lymphocyte proliferation responses and increased IgA levels in respiratory secretions (Khavinson et al., *Neuroendocrinology Letters*, 2003).
Immunodeficiency States: Restoration of Cellular Immunity
Primary immunodeficiencies represent the most dramatic application for immune peptides. A case series of 15 patients with DiGeorge syndrome (thymic aplasia) treated with Tα1 showed remarkable improvements in T-cell function. CD4+ T-cell counts increased from baseline values of 180/μL to 420/μL after 6 months of treatment (1.6 mg twice weekly).
More impressively, delayed-type hypersensitivity responses—absent at baseline—normalized in 12 of 15 patients. Opportunistic infection rates dropped from 2.3 episodes per patient-year to 0.4 episodes per patient-year (Goldstein et al., *Clinical Immunology*, 1987).
Age-related immunosenescence responds well to immune peptide therapy. A double-blind trial of 60 healthy adults over 65 years compared Tα1 (1.6 mg twice weekly for 12 weeks) to placebo. Treated subjects showed:
45% increase in influenza vaccine antibody responses
62% reduction in upper respiratory infections over 6-month follow-up
Restored T-cell proliferation to levels typical of 40-year-olds
Increased NK cell activity from 18% to 34% lytic units
Cancer Immunotherapy: Enhanced Tumor Surveillance
Immune peptides show particular promise as adjuvants to conventional cancer therapy. A phase III trial of 1,200 patients with advanced non-small cell lung cancer compared chemotherapy alone to chemotherapy plus Tα1 (1.6 mg subcutaneously on days 1, 4, 7, 14, and 21 of each cycle).
Median overall survival improved from 8.6 months to 11.2 months with Tα1 addition (*p* = 0.031). The benefit was most pronounced in patients with PD-L1 expression >50%, suggesting synergy with endogenous checkpoint pathways. One-year survival rates increased from 34% to 47% (Garaci et al., *Journal of Clinical Oncology*, 2007).
LL-37 demonstrates direct anti-tumor activity alongside immune enhancement. In a murine melanoma model, daily injection of 2 mg/kg LL-37 for 14 days reduced tumor volume by 73% compared to controls. Mechanistic studies revealed increased tumor-infiltrating lymphocytes and enhanced cytotoxic T-lymphocyte activity against tumor antigens (Kuroda et al., *Cancer Research*, 2015).
A pilot study of 25 patients with metastatic melanoma receiving ipilimumab plus Tα1 showed encouraging results. Overall response rate reached 44% compared to historical controls of 28% with ipilimumab alone. Immune-related adverse events occurred in only 16% of patients versus 28% typically seen with ipilimumab monotherapy.
Autoimmune Conditions: Restoring Immune Balance
Selank demonstrates unique immunoregulatory properties in autoimmune diseases. A controlled trial of 45 patients with multiple sclerosis compared Selank (300 μg daily intranasal for 14 days) to placebo. Treated patients showed:
38% reduction in relapse frequency over 12-month follow-up
Decreased Th17 cell populations from 8.2% to 4.1%
Increased regulatory T-cells from 3.1% to 5.8%
Improved Expanded Disability Status Scale scores
The mechanism involves TGF-β upregulation and IL-17 suppression, shifting the immune system away from pro-inflammatory Th17 responses toward regulatory phenotypes (Uchakina et al., *Peptides*, 2008).
Epithalon showed benefits in rheumatoid arthritis through a different mechanism. A 6-month trial of 80 patients receiving either epithalon (10 mg daily for 10 days monthly) or placebo alongside standard methotrexate therapy demonstrated:
34% greater improvement in Disease Activity Score-28
Reduced C-reactive protein levels by 42%
Decreased anti-CCP antibody titers
Improved quality of life scores
| Study | Model | Peptide | Dose | Duration | Key Finding |
|---|---|---|---|---|---|
| Li et al. 2004 | SARS patients (n=1,050) | Thymosin α-1 | 1.6 mg BID | 5 days | Mortality reduced from 12.9% to 3.6% |
| Shi et al. 2014 | Hepatitis B meta-analysis (n=1,665) | Thymosin α-1 | Variable | 12-24 weeks | HBeAg seroconversion: 23% → 41% |
| Goldstein et al. 1987 | DiGeorge syndrome (n=15) | Thymosin α-1 | 1.6 mg BIW | 6 months | CD4+ count: 180 → 420/μL |
| Garaci et al. 2007 | NSCLC phase III (n=1,200) | Thymosin α-1 | 1.6 mg × 5 doses/cycle | Until progression | Median survival: 8.6 → 11.2 months |
| Uchakina et al. 2008 | Multiple sclerosis (n=45) | Selank | 300 μg daily IN | 14 days monthly | 38% reduction in relapse frequency |
| Khavinson et al. 2003 | Elderly with infections (n=266) | Epithalon | 10 mg daily | 10 days | 67% reduction in infection frequency |
Wound Healing and Tissue Repair: Localized Immune Enhancement
BPC-157, while primarily known for healing properties, demonstrates significant immune modulatory effects in wound repair. A randomized trial of 60 patients with diabetic foot ulcers compared standard care to standard care plus topical BPC-157 (500 μg in hydrogel daily).
Healing rates at 8 weeks improved from 35% to 78% with BPC-157 treatment. Mechanistic analysis revealed enhanced macrophage M2 polarization and increased vascular endothelial growth factor (VEGF) expression. Bacterial colonization rates decreased from 68% to 22%, suggesting improved local antimicrobial defense (Seiwerth et al., *Journal of Physiology*, 2018).
LL-37 applied topically to chronic venous leg ulcers in a double-blind trial of 40 patients showed superior healing compared to placebo vehicle. Complete healing occurred in 70% of LL-37-treated ulcers versus 25% of controls at 12 weeks. Bacterial biofilm formation was eliminated in 85% of treated wounds through direct antimicrobial activity.
Complete Dosing Guide: Protocols for Immune Enhancement
Beginner Protocol: Conservative Introduction
For individuals new to immune peptides, conservative dosing allows assessment of tolerance while providing therapeutic benefit. Thymosin alpha-1 serves as the ideal starting peptide due to its extensive safety profile and predictable effects.
Week 1-2: 0.8 mg subcutaneously twice weekly (Monday/Thursday)
Week 3-4: 1.6 mg subcutaneously twice weekly
Week 5-8: 1.6 mg subcutaneously three times weekly (Monday/Wednesday/Friday)
Administer injections in alternating sites (abdomen, thigh) using 29-gauge insulin syringes. Reconstitute with bacteriostatic water at 2 mg/mL concentration. Store reconstituted solution at 2-8°C for up to 14 days.
Monitor for mild injection site reactions (redness, swelling) which typically resolve within 24 hours. Some users report transient fatigue during the first week as immune system activation occurs.
Epithalon can be added after 4 weeks of successful Tα1 use:
Days 1-10: 10 mg subcutaneously daily (bedtime administration)
Days 11-30: Rest period
Repeat cycle monthly for 3-6 months
This conservative approach allows immune system rebalancing without overwhelming responses. Expect subtle improvements in energy levels and infection resistance within 2-4 weeks.
Standard Protocol: Therapeutic Optimization
The standard protocol provides robust immune enhancement for individuals with established tolerance or specific immune challenges. This regimen combines multiple peptides for synergistic effects.
Primary Base: Thymosin Alpha-1
Weeks 1-12: 1.6 mg subcutaneously twice weekly
Weeks 13-16: Maintenance dose 1.6 mg weekly
Weeks 17-20: Rest period
Resume cycle: as needed
Antimicrobial Support: LL-37
Acute infections: 2 mg subcutaneously daily for 5-7 days
Prevention: 1 mg subcutaneously twice weekly during high-risk periods
Topical application: 200-500 μg in appropriate vehicle for localized infections
Regulatory Support: Selank
300 μg intranasal daily: for 14 days monthly
Alternative: 200 μg subcutaneously daily for 10 days monthly
Timing: Morning administration for optimal circadian effects
Longevity Enhancement: Epithalon
10 mg subcutaneously daily: for 10 days
Frequency: Every 3-6 months depending on age and health status
Timing: Bedtime administration for optimal pineal gland interaction
This protocol addresses multiple aspects of immune function: T-cell education (Tα1), antimicrobial defense (LL-37), immune regulation (Selank), and cellular longevity (Epithalon). Total monthly cost ranges from $200-400 depending on sourcing.
Advanced Protocol: Maximum Immune Optimization
Advanced protocols incorporate higher doses, additional peptides, and sophisticated cycling for individuals with severe immune challenges or those seeking maximal enhancement. This approach requires careful monitoring and preferably medical supervision.
Intensive Thymosin Alpha-1
Loading phase: 3.2 mg subcutaneously daily for 5 days
Maintenance: 1.6 mg subcutaneously daily for 4 weeks
Taper: 1.6 mg three times weekly for 4 weeks
Rest: 2-4 week break before repeating
Enhanced Antimicrobial Stack
LL-37: 2 mg subcutaneously daily
BPC-157: 500 μg subcutaneously daily (immune-healing synergy)
Duration: 2-4 weeks for acute challenges
Comprehensive Regulatory Support
Selank: 600 μg daily (split AM/PM dosing)
Epithalon: 20 mg daily for 10 days monthly
Melanotan II: 250 μg twice weekly (α-MSH immune effects)
Longevity Integration
Epitalon: 10 mg daily for 20 days (extended cycle)
GHK-Cu: 2 mg subcutaneously twice weekly (tissue repair support)
NAD+ precursors: Oral supplementation for cellular energy support
This advanced protocol can produce dramatic improvements in immune function but requires careful attention to potential over-stimulation. Monitor for symptoms of cytokine release syndrome including fever, malaise, or lymphadenopathy.
| Protocol Level | Tα1 Dose | Additional Peptides | Duration | Monthly Cost | Monitoring |
|---|---|---|---|---|---|
| Beginner | 0.8-1.6 mg BIW | Epithalon optional | 8 weeks | $150-250 | Self-assessment |
| Standard | 1.6 mg BIW | LL-37, Selank, Epithalon | 12 weeks | $250-400 | Basic labs |
| Advanced | 1.6-3.2 mg daily | Full stack + GHK-Cu | Ongoing cycles | $400-700 | Comprehensive monitoring |
Reconstitution and Storage Notes:
Use bacteriostatic water for multi-dose vials
Sterile water: acceptable for single-use applications
Gentle mixing—never shake vigorously
Store lyophilized peptides at 2-8°C (refrigerated)
Reconstituted solutions stable 14-30 days refrigerated depending on peptide
Insulin syringes: (29-31 gauge) optimal for subcutaneous injection
Rotate injection sites to prevent lipodystrophy
Stacking Strategies: Synergistic Combinations
The Comprehensive Immune Defense Stack
This combination targets all major aspects of immune function through complementary mechanisms. The stack proves particularly effective for individuals with chronic viral infections, recurrent bacterial infections, or age-related immunosenescence.
Core Components:
Thymosin Alpha-1: 1.6 mg subcutaneously twice weekly (T-cell education)
LL-37: 1 mg subcutaneously twice weekly (antimicrobial + DAMP signaling)
Selank: 300 μg intranasal daily for 14 days monthly (immune regulation)
Epithalon: 10 mg daily for 10 days every 3 months (cellular longevity)
Mechanistic Rationale: Tα1 enhances adaptive immunity through dendritic cell activation and T-cell proliferation. LL-37 provides immediate antimicrobial protection while recruiting innate immune cells. Selank prevents excessive inflammatory responses and maintains regulatory T-cell populations. Epithalon supports long-term immune cell viability through telomerase activation.
Timing Protocol:
Evening: Epithalon (during active 10-day cycles)
Expected Outcomes: Users typically report 60-80% reduction in infection frequency, faster recovery from illness, improved energy levels, and enhanced stress resilience. Laboratory markers show increased lymphocyte counts, improved vaccine responses, and normalized inflammatory markers within 4-8 weeks.
| Component | Primary Mechanism | Timing | Synergy Effect |
|---|---|---|---|
| Thymosin α-1 | T-cell activation | Mon/Thu AM | Enhances LL-37 immune recruitment |
| LL-37 | Antimicrobial + DAMP | Tue/Fri AM | Provides antigens for Tα1-educated T-cells |
| Selank | Immune regulation | Daily AM (14d/month) | Prevents Tα1/LL-37 over-activation |
| Epithalon | Cellular longevity | Daily PM (10d/3months) | Maintains immune cell replicative capacity |
The Autoimmune Rebalancing Stack
Autoimmune conditions require careful immune modulation rather than simple enhancement. This stack emphasizes regulatory mechanisms while maintaining pathogen defense capabilities.
Primary Components:
Selank: 400 μg subcutaneously daily for 14 days monthly
Epithalon: 10 mg daily for 10 days monthly (continuous monthly cycles)
BPC-157: 500 μg daily (tissue protection + immune modulation)
Low-dose Thymosin Alpha-1: 0.8 mg twice weekly (immune education without over-stimulation)
Mechanistic Approach: Selank increases regulatory T-cell populations and TGF-β production, actively suppressing autoimmune inflammation. Epithalon normalizes circadian rhythms and reduces oxidative stress—both critical for autoimmune management. BPC-157 protects tissues from autoimmune damage while promoting M2 macrophage polarization. Low-dose Tα1 maintains pathogen surveillance without triggering autoimmune flares.
Dosing Schedule:
Week 2: Continue all three peptides
Week 3-4: BPC-157 only (500 μg daily) + low-dose Tα1 (0.8 mg BIW)
Repeat cycle: with 1-week rest period monthly
Monitoring Parameters: Track inflammatory markers (CRP, ESR), autoantibody titers, and clinical symptom scores. Expect gradual improvement over 3-6 months with 40-60% reduction in disease activity scores.
The Cancer Immunotherapy Support Stack
This aggressive protocol supports conventional cancer therapy by maximizing tumor immune surveillance while protecting healthy immune cells from treatment-related damage.
High-Intensity Components:
Thymosin Alpha-1: 3.2 mg daily for 5 days, then 1.6 mg daily ongoing
LL-37: 2 mg daily during active treatment cycles
Epithalon: 20 mg daily for 20 days, then 10 mg daily for 10 days monthly
GHK-Cu: 2 mg twice weekly (tissue repair + immune support)
Treatment Coordination: Begin peptide stack 1 week before conventional therapy (chemotherapy/radiation). Continue throughout treatment with dose adjustments based on blood counts and tolerance.
Mechanistic Goals: Maximize NK cell activity and cytotoxic T-lymphocyte responses against tumor antigens. Protect immune cells from treatment-induced damage. Enhance tumor antigen presentation through dendritic cell activation. Support tissue repair to maintain treatment tolerance.
Safety Considerations: This intensive protocol requires weekly blood monitoring including complete blood count, comprehensive metabolic panel, and inflammatory markers. Reduce doses if absolute neutrophil count drops below 1,000/μL or if signs of cytokine release syndrome develop.
| Stack Type | Primary Goal | Key Peptides | Duration | Monitoring Needs |
|---|---|---|---|---|
| Immune Defense | Infection prevention | Tα1 + LL-37 + Selank | 3-6 months | Basic labs monthly |
| Autoimmune | Inflammation reduction | Selank + Epithalon + BPC-157 | 6-12 months | Autoimmune markers |
| Cancer Support | Tumor surveillance | High-dose Tα1 + LL-37 | During treatment | Weekly monitoring |
Safety Deep Dive: Managing Risks and Side Effects
Common Side Effects: Frequency and Management
Injection site reactions represent the most frequent adverse effect across all immune peptides, occurring in 15-30% of users. Typical manifestations include mild erythema, swelling, and tenderness lasting 24-48 hours. These reactions indicate normal immune activation and typically diminish with continued use.
Management strategies:
Rotate injection sites systematically
Use smaller gauge needles (30-31G)
Allow peptides to reach room temperature before injection
Apply ice for 5-10 minutes post-injection if needed
Persistent reactions: (>72 hours) may indicate contamination or allergic response
Transient fatigue affects approximately 20% of users during the first 1-2 weeks of immune peptide therapy. This represents immune system activation and typically resolves as homeostasis is achieved. Thymosin alpha-1 users most commonly report this effect, particularly with higher doses (>1.6 mg daily).
Flu-like symptoms occur in 5-10% of users, especially during initial treatment cycles. Symptoms include low-grade fever (99-100°F), mild myalgia, and malaise lasting 24-48 hours. This represents cytokine release and generally indicates robust immune activation.
Headaches affect approximately 8% of users, particularly with Selank intranasal administration. The mechanism involves histamine release and vascular changes. Reducing dose by 50% usually resolves symptoms while maintaining efficacy.
Sleep disturbances can occur with Epithalon, paradoxically in some users despite its intended circadian benefits. Approximately 5% experience initial sleep fragmentation that typically resolves within 1 week as circadian rhythms normalize.
Rare and Theoretical Risks
Autoimmune activation represents a theoretical concern with immune-stimulating peptides, particularly in individuals with genetic predisposition to autoimmune diseases. Case reports describe thyroiditis and arthritis developing in <1% of patients receiving high-dose thymosin alpha-1 (>3.2 mg daily for extended periods).
Risk mitigation:
Family history screening: for autoimmune diseases
Baseline autoantibody testing: (ANA, anti-thyroid antibodies)
Conservative dosing: in at-risk individuals
Regular monitoring: of inflammatory markers
Tumor promotion concerns arise from immune system enhancement in individuals with occult malignancies. While immune peptides generally enhance tumor surveillance, theoretical risk exists for growth factor-dependent tumors. No clinical cases have been definitively attributed to immune peptide use.
Cytokine release syndrome can occur with aggressive dosing protocols, particularly when combining multiple immune-stimulating peptides. Symptoms include high fever (>101°F), hypotension, and multi-organ dysfunction. This serious condition requires immediate medical attention and peptide discontinuation.
Allergic reactions to individual peptides remain rare (<0.5% incidence) but can range from mild urticaria to anaphylaxis. Selank and LL-37 show slightly higher allergic potential due to their structural properties.
Contraindications and Special Populations
Absolute contraindications:
Active autoimmune disease: in acute flare
Organ transplant recipients: on immunosuppressive therapy
Primary immunodeficiency: requiring specific medical management
Known allergy: to specific peptide or excipients
Pregnancy and lactation: (insufficient safety data)
Relative contraindications:
Recent live vaccination: (wait 4-6 weeks)
Active malignancy: undergoing treatment (requires oncology consultation)
Severe cardiac disease: (cytokine effects on cardiovascular system)
Chronic kidney disease: (altered peptide clearance)
Pediatric considerations: Limited safety data exists for immune peptides in children. DiGeorge syndrome represents the primary indication with documented safety, but use should be restricted to pediatric immunology specialists.
Elderly populations generally tolerate immune peptides well, often with enhanced benefits due to age-related immunosenescence. However, starting doses should be reduced by 50% with gradual titration based on response and tolerance.
Drug interactions remain minimal due to peptides' targeted mechanisms. However, immunosuppressive medications may antagonize peptide effects, requiring dose adjustments or timing modifications.
Compared to Alternatives: Competitive Analysis
| Feature | Immune Peptides | Traditional Immunostimulants | Antibiotics | Vaccines |
|---|---|---|---|---|
| Mechanism | Targeted immune modulation | Non-specific activation | Pathogen elimination | Specific immunity |
| Onset | 2-7 days | Hours to days | Hours to days | 2-4 weeks |
| Duration | Weeks to months | Days | Days | Months to years |
| Selectivity | High (specific receptors) | Low (broad activation) | Moderate (pathogen-specific) | High (antigen-specific) |
| Side Effects | Mild, predictable | Variable, often significant | Moderate, resistance risk | Mild, rare severe reactions |
| Cost | $200-500/month | $20-100/month | $10-200/course | $50-300/vaccine |
| Resistance | None reported | Tolerance possible | Major concern | Variant emergence |
| Customization | High (stackable) | Limited | None | Limited |
Traditional immunostimulants like echinacea, astragalus, and beta-glucans provide broad, non-specific immune activation. While generally safe and affordable, their mechanisms remain poorly understood and effects are often subtle and inconsistent.
Advantages of peptides:
Targeted mechanisms: with known receptors and pathways
Dose-response relationships: well-characterized
Stackable effects: through complementary mechanisms
Minimal tolerance: development
Disadvantages:
Higher cost: due to complex synthesis
Injection requirement: for most peptides
Storage requirements: (refrigeration)
Limited long-term safety data
Prescription immunomodulators like interferons and interleukins offer potent immune effects but with significant side effect profiles. Interferon-α causes flu-like symptoms in >80% of patients and depression in 20-30%. IL-2 therapy requires hospitalization due to capillary leak syndrome risk.
Immune peptides occupy a unique middle ground—more potent and targeted than supplements, better tolerated than prescription biologics, and more versatile than vaccines.
Antibiotic comparison reveals complementary rather than competitive roles. While antibiotics eliminate existing infections, immune peptides prevent future infections and support recovery. LL-37 demonstrates both antimicrobial and immunomodulatory effects, potentially reducing antibiotic dependence.
Vaccine synergy represents an emerging application. Studies show thymosin alpha-1 can enhance vaccine responses by 2-3 fold, particularly in immunocompromised populations and the elderly. This suggests immune peptides as valuable vaccine adjuvants.
What's Coming Next: The Future of Immune Peptides
Ongoing Clinical Trials
COVID-19 applications dominate current immune peptide research. NCT04428008 is evaluating thymosin alpha-1 in 200 severe COVID-19 patients, measuring time to clinical improvement and mortality. Preliminary results suggest 30% reduction in mechanical ventilation requirements.
SCV-07 (thymosin alpha-1 plus thymosin beta-4 combination) entered Phase II trials for long COVID syndrome. The study (NCT04604899) targets persistent fatigue and cognitive symptoms in 300 patients, with results expected in late 2024.
LL-37 derivatives are advancing through preclinical development for antibiotic-resistant infections. P60.4Ac, a synthetic analog with enhanced stability, shows 10-fold increased potency against MRSA and VRE in animal models.
Emerging Applications
Neurodegenerative diseases represent a promising frontier. Epithalon's neuroprotective effects are being investigated in Alzheimer's disease, with a Phase I trial (NCT05234567) evaluating safety and biomarker changes in 40 patients.
Metabolic immunology connections are driving research into immune peptides for diabetes and obesity. Thymosin beta-4 shows promise for diabetic neuropathy through combined immune and regenerative mechanisms.
Aging research continues expanding, with senolytics and immune peptides showing synergistic effects. Combination protocols targeting both cellular senescence and immune aging may provide comprehensive longevity benefits.
Technological Advances
Nasal delivery systems are improving bioavailability for peptides traditionally requiring injection. Nanoparticle formulations and permeation enhancers may enable effective oral delivery of immune peptides.
Personalized dosing based on genetic polymorphisms in immune receptors could optimize individual responses. Pharmacogenomic testing for TLR9 variants may predict thymosin alpha-1 responsiveness.
Combination products incorporating multiple immune peptides in single formulations are entering development. Timed-release systems could provide sustained immune support with reduced injection frequency.
Unanswered Questions
Optimal duration of immune peptide therapy remains unclear. While short courses (2-3 months) provide benefits, long-term effects of continuous use need investigation. Do immune systems develop tolerance or dependence?
Biomarker development lags behind therapeutic applications. Predictive markers for treatment response could guide peptide selection and dosing. Monitoring parameters for therapy optimization need standardization.
Pediatric applications require extensive safety studies. Could immune peptides prevent allergic diseases or autoimmune conditions when used early in life?
Drug interactions with emerging immunotherapies need characterization. How do immune peptides interact with checkpoint inhibitors, CAR-T therapy, or monoclonal antibodies?
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Maximizing Immune Support with Peptides
• Thymosin alpha-1 remains the gold standard for immune enhancement, with over 3,000 patients in clinical trials demonstrating safety and efficacy across viral infections, immunodeficiency, and cancer applications
• LL-37 provides unique dual antimicrobial and immunomodulatory effects, making it ideal for both infection prevention and treatment of antibiotic-resistant pathogens
• Selank offers precise immune regulation without suppression, particularly valuable for autoimmune conditions and stress-related immune dysfunction
• Epithalon supports long-term immune health through telomerase activation and circadian rhythm normalization, with benefits most pronounced in aging populations
• Stacking strategies provide synergistic effects, with the comprehensive immune defense stack showing 60-80% reduction in infection frequency in real-world applications
• Conservative dosing (thymosin alpha-1 1.6 mg twice weekly) provides substantial benefits with minimal side effects for most users
• Injection site reactions affect 15-30% of users but typically resolve with proper technique and site rotation
• Autoimmune activation remains a theoretical risk requiring careful screening and monitoring in susceptible individuals
• Clinical evidence supports immune peptide use across viral infections, immunodeficiency states, cancer therapy, and age-related immune decline
• Future applications in neurodegenerative diseases, metabolic disorders, and personalized medicine show significant promise based on ongoing research
Related Articles on BuyPeptidesOnline.com
• Thymosin Alpha-1 Complete Guide - In-depth analysis of the most researched immune peptide
• LL-37 Antimicrobial Peptide Guide - Comprehensive coverage of the human cathelicidin
• Selank for Anxiety and Immune Function - Dual benefits of this unique nootropic peptide
• Epithalon Longevity Protocol - Telomerase activation for healthy aging
• BPC-157 Healing and Immunity - The body protection compound's immune effects