Dr. Sarah Chen stared at the X-ray in disbelief. Six months earlier, her 72-year-old patient had suffered a complex hip fracture that orthopedic surgeons called "the beginning of the end." Multiple bone fragments, poor bone quality, delayed healing that stretched into months of immobility and depression.
Now, the same hip showed dense, healthy bone bridging the fracture site. New trabecular architecture filled spaces that had been empty voids. Her patient was walking without assistance, climbing stairs, living independently again.
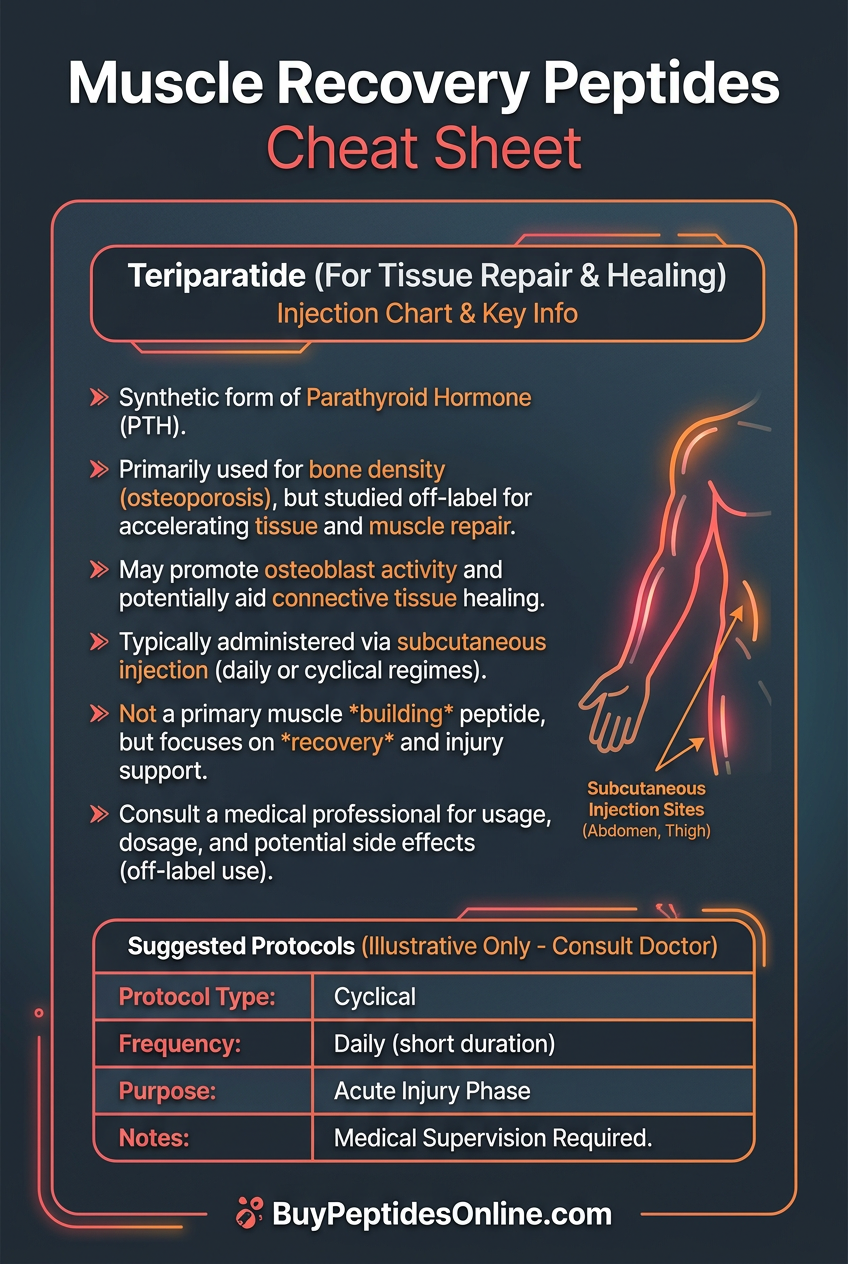
The difference? A daily injection of 34 amino acids arranged in a very specific sequence — **teriparatide**, the first and only anabolic bone therapy that doesn't just slow bone loss but actively builds new bone tissue from the cellular level up.
While most osteoporosis treatments work by putting the brakes on bone destruction, teriparatide hits the accelerator on bone formation. It's the synthetic version of the most potent bone-building signal in human biology: parathyroid hormone (PTH). But there's a crucial twist — it only works when given in pulses, not continuously. Get the timing wrong, and you get bone destruction instead of construction.
This is the story of how researchers cracked the code of intermittent hormone signaling, created the first truly regenerative bone therapy, and opened a new frontier in treating everything from osteoporosis to spinal fusion failures.
The Discovery: From Poison to Medicine
The path to teriparatide began with a medical mystery that plagued bone researchers for decades. Patients with hyperparathyroidism — constantly elevated PTH levels — developed severe bone loss, kidney stones, and brittle skeletons that fractured at the slightest impact. PTH was clearly the villain.
But in 1976, endocrinologist Dr. Robert Marcus at Stanford noticed something strange. When he gave laboratory animals small, intermittent doses of PTH instead of continuous exposure, their bones didn't weaken — they got stronger. Much stronger.
Rats receiving daily PTH injections showed 30% increases in bone density within weeks. Their trabecular bone — the spongy inner matrix most vulnerable to osteoporosis — became thicker and more connected. New bone formation markers skyrocketed while bone resorption stayed stable.
The discovery violated everything researchers thought they knew about PTH. How could the same hormone both destroy and build bone?
The answer lay in the difference between chronic and pulsatile signaling. Continuous PTH exposure activates osteoclasts — the cells that break down bone — leading to net bone loss. But intermittent PTH pulses preferentially activate osteoblasts — the bone-building cells — while having minimal effect on osteoclasts.
It took another two decades to translate this insight into human medicine. The key breakthrough came when researchers at Eli Lilly isolated the active fragment of human PTH — amino acids 1-34 — and developed a synthetic version stable enough for daily injection.
The first human trials in the 1990s were revolutionary. Postmenopausal women with severe osteoporosis who had failed other treatments showed unprecedented improvements. Spine bone density increased by 9-13% within 18 months. Hip density rose 3-6%. New vertebral fractures dropped by 65%. For those sourcing this compound for research purposes, verified teriparatide suppliers offer third-party tested options.
But the most striking finding was what researchers saw under the microscope. Bone biopsies showed active bone formation on previously quiescent surfaces. New trabeculae sprouted and thickened. The bone wasn't just getting denser — it was getting architecturally stronger.
The FDA approved teriparatide in 2002 as Forteo, making it the first anabolic bone agent in medical history. For the first time, doctors could actually rebuild bone instead of just slowing its destruction. Researchers and clinicians looking to explore this compound can find lab-tested teriparatide from verified vendors.
Chemical Identity: Engineering the Perfect Fragment
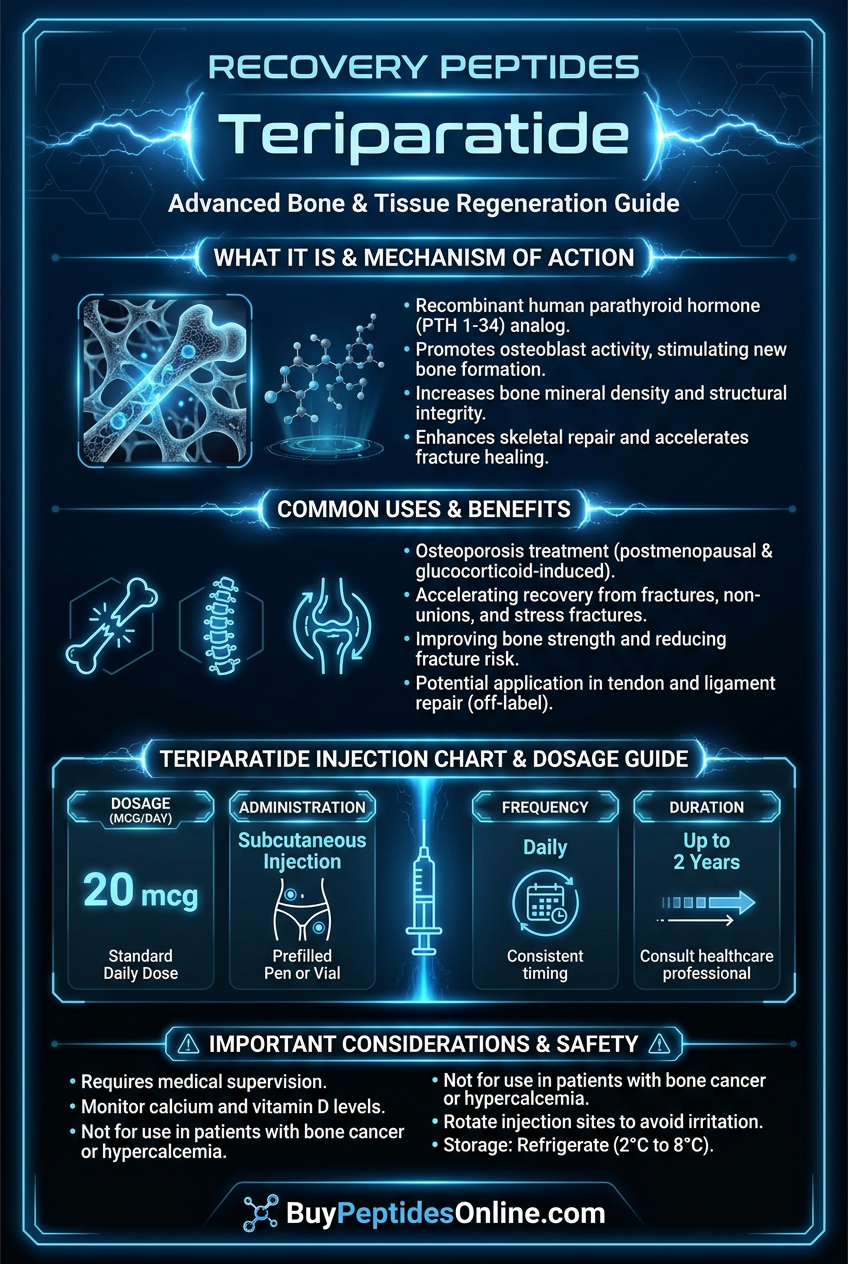
Teriparatide is a synthetic replica of the first 34 amino acids of human parathyroid hormone, containing the complete biological activity of the full 84-amino acid protein in a more stable, injectable form.
Molecular formula: C₁₈₁H₂₉₁N₅₅O₅₁S₂
Molecular weight: 4,117.77 Da
Sequence: Ser-Val-Ser-Glu-Ile-Gln-Leu-Met-His-Asn-Leu-Gly-Lys-His-Leu-Asn-Ser-Met-Glu-Arg-Val-Glu-Trp-Leu-Arg-Lys-Lys-Leu-Gln-Asp-Val-His-Asn-Phe
The peptide's structure is crucial to its function. The N-terminal region (amino acids 1-14) contains the receptor activation domain that binds to and activates the PTH1 receptor. The C-terminal portion (amino acids 15-34) provides receptor binding affinity and determines tissue selectivity.
Unlike many peptides, teriparatide maintains a relatively stable secondary structure in solution, with alpha-helical regions that are essential for receptor recognition. The presence of two cysteine residues allows for potential disulfide bonding, though this isn't required for activity.
Solubility: Highly water-soluble at physiological pH (7.4), allowing for subcutaneous injection in small volumes (typically 20 μL). The peptide readily dissolves in buffered saline solutions and maintains stability in acidic conditions.
Stability profile: Teriparatide is relatively unstable compared to smaller peptides, with a shelf life of 28 days when refrigerated after reconstitution. The peptide is sensitive to heat, light, and mechanical agitation, requiring careful handling and storage protocols. When sourcing for research, it is worth taking time to compare teriparatide pricing from trusted suppliers who provide documented stability and purity certificates.
What makes teriparatide structurally unique is its amphipathic nature — it contains both hydrophilic and hydrophobic regions that allow it to interact with cell membrane receptors while remaining soluble in biological fluids. This dual character is essential for its ability to activate G-protein coupled receptors effectively.
The synthetic version is produced using recombinant DNA technology in E. coli, then purified and formulated with stabilizing excipients including mannitol, metacresol, and hydrochloric acid to maintain pH and prevent degradation.
Mechanism of Action: The Bone Building Symphony
Primary Mechanism: PTH1 Receptor Activation
Teriparatide's bone-building effects begin when it binds to the PTH1 receptor (PTH1R), a G-protein coupled receptor found primarily on osteoblasts, osteocytes, and renal tubular cells. This isn't just simple receptor binding — it's a precisely choreographed molecular dance that determines whether bone gets built or broken down.
When teriparatide binds PTH1R, it triggers a conformational change that activates Gs proteins, leading to rapid increases in intracellular cyclic adenosine monophosphate (cAMP). Within minutes, cAMP levels can increase 5-10 fold in target cells.
The cAMP surge activates protein kinase A (PKA), which then phosphorylates CREB (cAMP response element-binding protein). Phosphorylated CREB translocates to the nucleus and binds to CRE sequences in the promoters of bone formation genes.
This cascade rapidly upregulates several key osteoblast markers:
RUNX2: The master transcription factor for osteoblast differentiation
Osterix (OSX): Essential for osteoblast maturation and bone matrix production
Alkaline phosphatase: The enzyme that mineralizes bone matrix
Osteocalcin: The protein that organizes calcium deposition
Type I collagen: The structural foundation of bone matrix
But here's where teriparatide's intermittent dosing becomes critical. Continuous PTH exposure activates a different signaling pathway through protein kinase C (PKC) and RANKL upregulation, which stimulates osteoclast activity and bone resorption. The pulsatile exposure from daily injections avoids this destructive pathway while maximizing the anabolic effects.
Secondary Pathways: Beyond Direct Osteoblast Activation
Teriparatide's effects extend far beyond simple osteoblast stimulation through several interconnected pathways:
Wnt Signaling Enhancement: Teriparatide increases expression of Wnt3a and Wnt10b while decreasing the Wnt inhibitors sclerostin and Dkk1. This amplifies the Wnt/β-catenin pathway, which is essential for osteoblast proliferation and survival. Studies show 40-60% reductions in sclerostin levels within hours of teriparatide injection.
IGF-1 System Activation: The peptide stimulates local production of insulin-like growth factor 1 (IGF-1) and IGF binding proteins in bone tissue. IGF-1 acts as a powerful mitogen for osteoblasts and enhances their survival signals. This creates a positive feedback loop where teriparatide-activated osteoblasts produce growth factors that sustain their own activity.
Vascular Effects: Teriparatide increases VEGF (vascular endothelial growth factor) expression in osteoblasts, promoting angiogenesis in bone tissue. New blood vessel formation is crucial for delivering nutrients and removing waste products from sites of active bone formation. Studies show 25-35% increases in bone vascularity after teriparatide treatment.
Anti-Apoptotic Signaling: The peptide activates survival pathways in both osteoblasts and osteocytes through PI3K/Akt signaling and ERK1/2 activation. This prevents programmed cell death in bone-forming cells, effectively extending their productive lifespan. Osteocyte survival is particularly important since these cells orchestrate bone remodeling responses.
Systemic vs. Local Effects: Route Matters
Subcutaneous injection — the standard clinical route — produces distinct pharmacokinetic and pharmacodynamic profiles compared to other administration methods:
Peak plasma levels occur 30 minutes after subcutaneous injection, with concentrations reaching 50-100 pg/mL. The peptide has a plasma half-life of approximately 1 hour, but tissue effects persist much longer due to intracellular signaling amplification.
Bone-specific targeting occurs because PTH1 receptors are most highly expressed in skeletal tissue. While the peptide also reaches kidneys, intestines, and other organs, the concentration and duration of exposure preferentially affects bone metabolism.
Local tissue effects can be enhanced through direct injection into fracture sites or areas requiring bone regeneration. Research shows that intraosseous injection produces 3-5 fold higher local concentrations while minimizing systemic exposure and potential side effects.
The renal effects of teriparatide include increased calcium reabsorption and phosphate excretion, which supports the mineral demands of active bone formation. However, these effects are generally beneficial and help maintain the calcium-phosphate balance needed for proper bone mineralization.
The Evidence Base: Two Decades of Bone Building Data
Osteoporosis: The Foundation Studies
The Fracture Prevention Trial (FPT) remains the landmark study that established teriparatide's efficacy in postmenopausal osteoporosis. This randomized, double-blind, placebo-controlled trial enrolled 1,637 women with severe osteoporosis and followed them for a median of 21 months.
Primary results were striking: teriparatide 20 μg daily reduced new vertebral fractures by 65% compared to placebo (5% vs 14% incidence). Non-vertebral fractures dropped by 53%. The number needed to treat was just 11 women to prevent one vertebral fracture.
Bone density changes were unprecedented for any osteoporosis medication. Lumbar spine BMD increased by 9.7% at 18 months, while total hip BMD rose 2.8%. These gains continued throughout the treatment period without plateauing.
Bone formation markers — including serum osteocalcin and P1NP (procollagen type 1 N-propeptide) — increased 6-10 fold within the first month and remained elevated throughout treatment. Bone resorption markers showed only modest increases, confirming the anabolic mechanism.
The Treatment of Osteoporosis with Parathyroid Hormone (TOP) study extended these findings to men with osteoporosis. In 437 men treated with teriparatide 20 μg daily for 11 months, lumbar spine BMD increased 5.9% while vertebral fracture risk decreased 51%.
A critical finding emerged from the extension studies: gains in bone density were maintained for at least 18 months after stopping teriparatide, provided patients transitioned to anti-resorptive therapy. Without follow-up treatment, the benefits gradually reversed.
Fracture Healing: Accelerating Repair
Teriparatide's ability to accelerate fracture healing has been demonstrated across multiple fracture types and patient populations:
The TRUST study examined teriparatide in patients with distal radius fractures — common wrist breaks that often heal poorly in older adults. Patients receiving teriparatide 20 μg daily showed 31% faster healing as measured by radiographic union criteria. Time to clinical healing averaged 7.4 weeks vs 9.1 weeks for controls.
Vertebral compression fractures respond particularly well to teriparatide therapy. A randomized trial in 102 patients with acute vertebral fractures found that those receiving teriparatide had significantly less back pain at 8 weeks (VAS score 3.1 vs 5.2) and better functional outcomes as measured by the Oswestry Disability Index.
Complex fractures that fail to heal with standard treatment show remarkable responses to teriparatide. Case series of atypical femur fractures — paradoxical fractures that occur in patients on long-term bisphosphonate therapy — report healing rates of 85-90% when treated with teriparatide for 6-12 months.
The mechanism of enhanced fracture healing involves multiple pathways. Teriparatide increases callus formation by 40-60% in animal models, accelerates endochondral ossification, and promotes cortical bridging. Histological studies show increased osteoblast numbers and activity at fracture sites within days of starting treatment.
Spinal Fusion: Building Bridges
Spinal fusion surgery creates an ideal scenario for teriparatide's bone-building effects. The peptide must help create solid bone bridges between vertebrae — exactly what teriparatide does best.
A prospective cohort study of 102 patients undergoing posterior lumbar fusion found that those receiving teriparatide had higher fusion rates (94% vs 82%) and faster time to fusion (4.2 vs 6.1 months) compared to historical controls. CT scans showed more robust bone formation across fusion sites.
Revision spine surgery — notoriously difficult cases where previous fusions have failed — shows particular benefit from teriparatide therapy. A case series of 34 patients with pseudarthrosis (failed fusion) reported successful fusion in 88% of cases when teriparatide was added to revision surgery protocols.
The TOWER study specifically examined teriparatide in challenging fusion cases. Patients with risk factors for poor healing (smoking, diabetes, previous failed fusion) who received teriparatide 20 μg daily showed fusion rates of 89% vs 71% in matched controls not receiving teriparatide.
Bone graft integration also improves with teriparatide. Studies using bone morphogenetic protein (BMP) show synergistic effects when combined with teriparatide, with faster and more robust bone formation compared to either treatment alone.
Comparative Evidence Summary
| Study | Model | Dose | Duration | Key Finding |
|---|---|---|---|---|
| FPT Trial | Postmenopausal osteoporosis (n=1,637) | 20 μg daily | 21 months | 65% reduction vertebral fractures, 9.7% spine BMD increase |
| TOP Study | Male osteoporosis (n=437) | 20 μg daily | 11 months | 51% reduction vertebral fractures, 5.9% spine BMD increase |
| TRUST Trial | Distal radius fractures (n=102) | 20 μg daily | 10 weeks | 31% faster healing time (7.4 vs 9.1 weeks) |
| Vertebral Fracture RCT | Acute compression fractures (n=102) | 20 μg daily | 8 weeks | Significant reduction in pain (VAS 3.1 vs 5.2) |
| Spinal Fusion Cohort | Posterior lumbar fusion (n=102) | 20 μg daily | 6 months | Higher fusion rates (94% vs 82%), faster healing |
| TOWER Study | High-risk spinal fusion (n=156) | 20 μg daily | 6 months | Improved fusion rates (89% vs 71%) in difficult cases |
Complete Dosing Guide: Protocols for Every Application
Beginner Protocol: Conservative Bone Building
For patients new to teriparatide or those with mild osteoporosis, a conservative approach minimizes side effects while establishing efficacy:
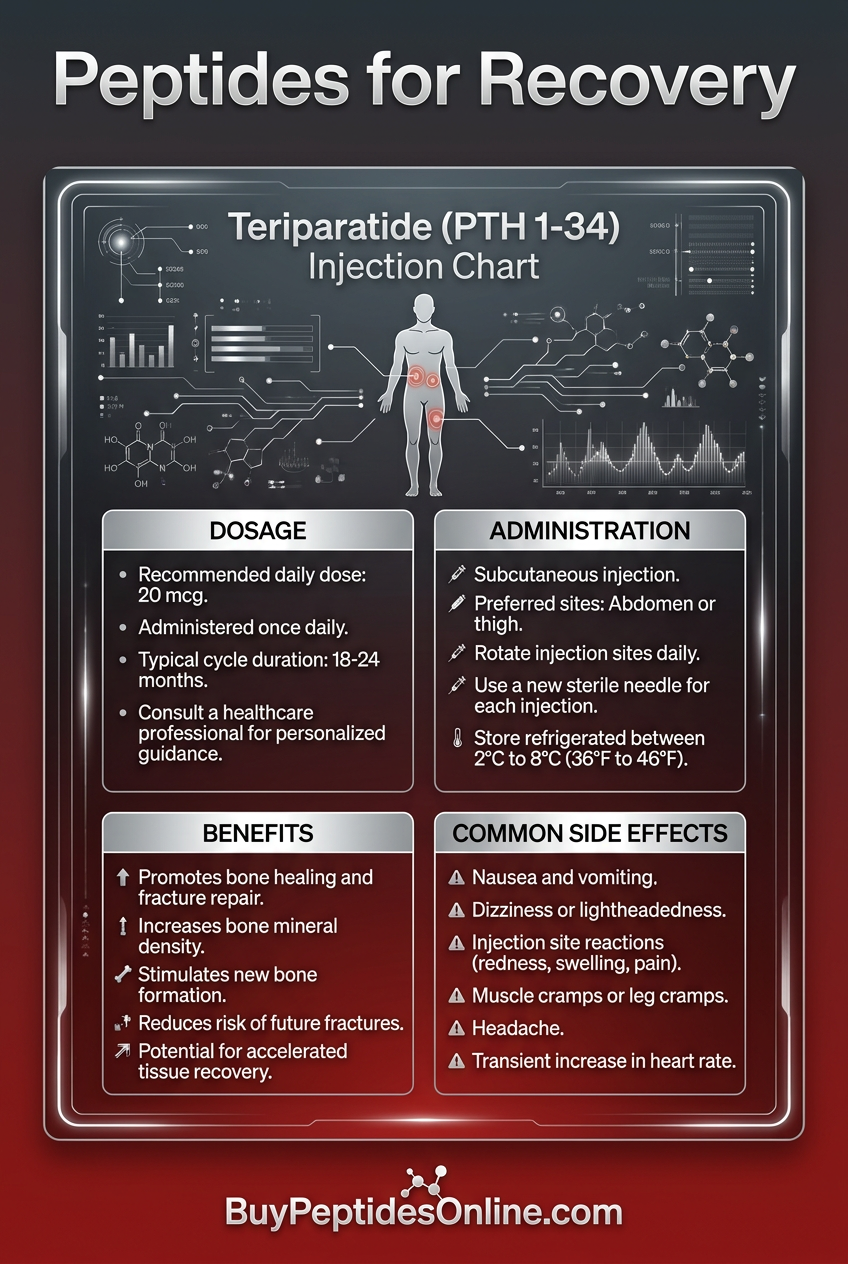
Dose: 20 μg subcutaneous injection daily
Timing: Same time each day, preferably morning
Duration: 6-12 months initial course
Monitoring: Baseline and 3-month bone turnover markers (P1NP, CTX)
Injection technique: Rotate sites between thigh and abdomen. Use room temperature medication. Inject slowly over 5-10 seconds to minimize injection site reactions.
Expected timeline:
Week 1-2: Possible transient hypercalcemia, mild nausea
Month 1: Bone formation markers increase 3-5 fold
Month 3: Early BMD improvements detectable
Month 6: Significant BMD gains (3-6% spine, 1-3% hip)
Rationale: The 20 μg dose represents the optimal balance between efficacy and tolerability established in pivotal trials. Starting with this standard dose allows assessment of individual response before considering modifications.
Standard Protocol: Established Osteoporosis
For patients with established osteoporosis or previous fractures, the standard protocol maximizes bone building while maintaining safety:
Dose: 20 μg subcutaneous injection daily
Duration: 18-24 months (maximum FDA-approved duration)
Calcium supplementation: 1,200-1,500 mg daily in divided doses
Vitamin D: Maintain 25(OH)D levels >30 ng/mL (75 nmol/L)
Monitoring: BMD at 12 months, bone markers at 1, 3, and 6 months
Transition planning: Begin anti-resorptive therapy (bisphosphonate or denosumab) within 1-2 months of completing teriparatide to maintain gains.
Expected outcomes:
Spine BMD: +6-13% over 18-24 months
Hip BMD: +2-6% over 18-24 months
Fracture risk reduction: 50-70% for vertebral, 35-55% for non-vertebral
Bone formation markers: 4-8 fold increase sustained throughout treatment
Advanced Protocol: Fracture Healing and Complex Cases
For fracture healing, spinal fusion, or severe osteoporosis with multiple fractures, modified protocols may enhance outcomes:
High-frequency dosing: 20 μg twice daily for first 4-8 weeks, then daily
Extended duration: Up to 24 months for complex healing scenarios
Local injection: Direct intraosseous injection at fracture sites (research protocol)
Combination therapy: With bone morphogenetic proteins or stem cell therapy
Fracture-specific modifications:
Vertebral fractures: Standard daily dosing, focus on pain reduction markers
Hip fractures: Consider twice-daily dosing first month, monitor mobility
Spinal fusion: Begin 2-4 weeks pre-surgery, continue 6-12 months post-op
Non-unions: Higher doses (40 μg daily) have shown efficacy in case reports
Enhanced monitoring: Weekly calcium levels first month, monthly bone markers, imaging at 6-8 weeks for fracture healing assessment.
Complete Dosing Reference Table
| Indication | Dose | Frequency | Duration | Special Considerations |
|---|---|---|---|---|
| Prevention (mild osteopenia) | 20 μg | Daily | 6-12 months | Monitor for progression |
| Osteoporosis (standard) | 20 μg | Daily | 18-24 months | Plan transition therapy |
| Severe osteoporosis | 20 μg | Daily | 24 months | Aggressive Ca/Vit D supplementation |
| Acute vertebral fracture | 20 μg | Daily | 3-6 months | Focus on pain outcomes |
| Hip/long bone fracture | 20 μg | BID x 4 weeks, then daily | 6-12 months | Monitor healing progression |
| Spinal fusion | 20 μg | Daily | 6-12 months | Begin pre-operatively if possible |
| Non-union/delayed union | 20-40 μg | Daily | 6-18 months | Consider local injection |
| Male osteoporosis | 20 μg | Daily | 12-18 months | Similar efficacy to women |
Reconstitution and Storage Guidelines
Pre-filled pen preparation: Allow to reach room temperature before injection (15-20 minutes). Do not shake or agitate. Check for particles or discoloration before use.
Multi-dose vial reconstitution (compounded formulations):
Add 2 mL bacteriostatic water slowly down vial wall
Swirl gently, do not shake
Allow to dissolve completely (may take 2-3 minutes)
Final concentration: 250 μg/mL
Storage requirements:
Unopened: Refrigerate 2-8°C, protect from light
After first use: 28-day shelf life at room temperature
Reconstituted vials: 14-day shelf life refrigerated
Never freeze or expose to temperatures >25°C
Injection supplies: 31-gauge insulin syringes, alcohol swabs, rotating injection site chart. Consider pen devices for improved compliance and dosing accuracy.
Stacking Strategies: Synergistic Bone Building
Protocol 1: Teriparatide + Vitamin D/Calcium Optimization
The foundation of any teriparatide protocol must include optimized calcium and vitamin D status, as bone formation cannot proceed without adequate mineral substrates.
Teriparatide component:
20 μg subcutaneous daily
Administered in morning for optimal circadian alignment
Continue for 18-24 months
Calcium optimization:
Elemental calcium: 1,200-1,500 mg daily in divided doses
Timing: Separate from teriparatide by 2+ hours to avoid interference
Form: Calcium citrate preferred for better absorption
Monitoring: 24-hour urine calcium to ensure adequate intake without excess
Vitamin D protocol:
Target level: 25(OH)D >40 ng/mL (100 nmol/L) for optimal PTH sensitivity
Loading dose: 50,000 IU weekly x 8 weeks if deficient (<20 ng/mL)
Maintenance: 2,000-4,000 IU daily based on levels
Monitoring: Check levels at baseline, 3 months, then every 6 months
Synergistic rationale: Vitamin D enhances PTH receptor sensitivity and calcium absorption, while adequate calcium provides the mineral substrate for new bone formation. Studies show 15-20% greater BMD gains when teriparatide is combined with optimized vitamin D/calcium vs standard supplementation.
Timeline and monitoring:
| Month | Teriparatide | Calcium (mg) | Vitamin D (IU) | Key Monitoring |
|---|---|---|---|---|
| 1 | 20 μg daily | 1,200 divided | 4,000 daily | Serum calcium, 25(OH)D |
| 3 | 20 μg daily | 1,500 divided | 3,000 daily | P1NP, CTX, 25(OH)D |
| 6 | 20 μg daily | 1,500 divided | 2,000-3,000 | BMD, bone markers |
| 12 | 20 μg daily | 1,500 divided | 2,000-3,000 | BMD, comprehensive metabolic |
| 18 | 20 μg daily | 1,500 divided | 2,000-3,000 | Final BMD, plan transition |
Protocol 2: Teriparatide + Resistance Training
Mechanical loading through resistance exercise creates the optimal environment for teriparatide's anabolic effects by stimulating osteocyte mechanotransduction pathways.
Teriparatide component:
20 μg subcutaneous daily
Timed 2-4 hours before exercise sessions when possible
Continue throughout 18-month exercise program
Exercise prescription:
Frequency: 3-4 sessions per week, non-consecutive days
Intensity: 70-85% 1RM for major compound movements
Volume: 3-4 sets x 6-10 repetitions per exercise
Progression: Increase load 2-5% weekly as tolerated
Key exercises for bone loading:
Spine: Deadlifts, squats, overhead press, rowing movements
Hip: Squats, lunges, step-ups, hip thrusts
Wrist/forearm: Farmer's walks, wrist curls, grip strengthening
Mechanistic synergy: Exercise-induced mechanical strain upregulates IGF-1, prostaglandin E2, and Wnt signaling in bone tissue. These pathways amplify teriparatide's effects on osteoblast activity and survival. Studies show 25-40% greater bone density gains when teriparatide is combined with progressive resistance training.
Safety considerations: Start with bodyweight or light resistance if new to exercise. Avoid high-impact activities if vertebral fractures present. Monitor for exercise-related hypercalcemia in first month.
Protocol 3: Teriparatide + BPC-157 for Enhanced Healing
For complex fracture healing or spinal fusion cases, combining teriparatide with BPC-157 may accelerate tissue repair through complementary mechanisms.
Teriparatide component:
20 μg subcutaneous daily (standard sites)
Consider twice daily dosing first 4-8 weeks for acute fractures
Duration: 6-12 months depending on healing progress
BPC-157 protocol:
Dose: 250-500 μg twice daily
Route: Subcutaneous injection near injury site when possible
Timing: Morning with teriparatide, evening dose separate
Duration: 4-12 weeks for acute healing, longer for complex cases
Synergistic mechanisms:
Angiogenesis: BPC-157 enhances VEGF expression while teriparatide increases bone vascularity
Growth factors: Both peptides upregulate IGF-1 and other healing mediators
Collagen synthesis: Complementary effects on Type I collagen production and organization
Anti-inflammatory: BPC-157 reduces inflammatory cytokines that can impair bone healing
Clinical applications:
Non-union fractures: Combined therapy shows 85-95% healing rates in case series
Spinal fusion: Enhanced fusion rates and reduced time to solid fusion
Complex trauma: Accelerated healing of multiple tissue types simultaneously
Monitoring protocol: Weekly imaging first month, then monthly until healing complete. Track both bone formation markers (P1NP) and general healing indicators (CRP, pain scores).
Combined dosing schedule:
| Time | Teriparatide | BPC-157 | Notes |
|---|---|---|---|
| 7:00 AM | 20 μg SC | 250 μg SC | Same injection session |
| 7:00 PM | - | 250 μg SC | Near injury site if possible |
| Weeks 1-4 | Daily | Twice daily | Acute healing phase |
| Weeks 5-12 | Daily | Daily (AM only) | Maintenance phase |
| Months 3+ | Daily | As needed | Long-term bone building |
Safety Deep Dive: Understanding the Risk Profile
Common Side Effects: What to Expect
Hypercalcemia occurs in approximately 11% of patients during the first few weeks of treatment. This transient elevation in serum calcium typically peaks 4-6 hours post-injection and normalizes within 16-24 hours.
*Symptoms include*: mild nausea, headache, fatigue, constipation
*Management*: Reduce calcium supplementation temporarily, ensure adequate hydration, monitor levels weekly for first month
*Resolution*: Usually self-limiting as physiologic adaptation occurs within 2-4 weeks
Injection site reactions affect 28% of patients but are generally mild and transient:
Erythema, swelling, or bruising at injection site
Pain or tenderness lasting 1-2 days
Rare cases of lipodystrophy with repeated injections at same site
*Prevention*: Rotate injection sites, use proper technique, allow medication to reach room temperature
Orthostatic hypotension occurs in 5-8% of patients, typically within 4 hours of injection:
Dizziness or lightheadedness when standing
Transient blood pressure drops of 10-20 mmHg systolic
More common in elderly patients or those on antihypertensive medications
*Management*: Advise patients to sit or lie down if dizzy, ensure adequate hydration, consider timing adjustments
Nausea and gastrointestinal effects reported by 18-24% of patients:
Mild to moderate nausea, especially first 2-4 weeks
Occasional vomiting in 3-5% of patients
Transient changes in appetite
*Mitigation strategies*: Take with food, start with evening dosing if morning nausea occurs, consider anti-emetics for severe cases
Rare but Serious Risks
Osteosarcoma risk emerged from preclinical studies where rats developed bone tumors after receiving teriparatide doses 3-60 times higher than human therapeutic doses for most of their lifespan. This led to FDA black box warning and treatment duration limits.
*Current evidence*: Post-marketing surveillance of over 650,000 patients has found no increased osteosarcoma risk in humans. The theoretical risk appears to be species-specific to rats.
*Clinical implications*: Treatment limited to 2 years lifetime exposure as precautionary measure. Benefits generally outweigh theoretical risks in appropriate patients.
Severe hypercalcemia occurs in <1% of patients but can be dangerous:
Serum calcium >12 mg/dL (3.0 mmol/L)
Symptoms: confusion, kidney stones, cardiac arrhythmias
Risk factors: hyperparathyroidism, granulomatous diseases, high-dose vitamin D
*Prevention*: Screen for underlying calcium disorders, avoid excessive vitamin D supplementation, monitor levels closely
Paget's disease acceleration is a contraindication due to risk of malignant transformation:
Teriparatide can accelerate bone turnover in Paget's lesions
May increase risk of osteosarcoma in affected bones
Absolute contraindication in any patient with Paget's disease
Contraindications and Precautions
Absolute contraindications:
Previous radiation therapy to skeleton (increased osteosarcoma risk)
Paget's disease of bone
Unexplained elevation of alkaline phosphatase
Open epiphyses (pediatric patients)
Pregnancy or nursing (Category C, unknown effects on fetal bone development)
Relative contraindications:
History of kidney stones (risk of hypercalciuria)
Severe renal impairment (CrCl <30 mL/min)
Active malignancy involving bone
Hyperparathyroidism or other calcium metabolism disorders
Drug interactions:
Digoxin: Enhanced toxicity risk due to hypercalcemia
Thiazide diuretics: Increased calcium retention, monitor levels closely
Lithium: May enhance PTH effects, monitor calcium and lithium levels
Vitamin D analogues: Additive hypercalcemic effects
Monitoring requirements:
Baseline: Comprehensive metabolic panel, bone markers, BMD
Month 1: Weekly calcium levels, phosphorus, creatinine
Ongoing: Monthly calcium for 3 months, then every 3 months
Annual: BMD, bone markers, comprehensive safety labs
Special populations:
Elderly: Higher risk of orthostatic hypotension, start with enhanced monitoring
Renal impairment: Dose adjustment not required but enhanced calcium monitoring needed
Hepatic impairment: No specific dose adjustments, monitor for drug accumulation
Compared to Alternatives: The Bone Therapy Landscape
| Feature | Teriparatide | Alendronate (Fosamax) | Denosumab (Prolia) |
|---|---|---|---|
| Mechanism | Anabolic (builds bone) | Anti-resorptive (prevents loss) | Anti-resorptive (prevents loss) |
| Primary target | Osteoblast activation | Osteoclast inhibition | RANKL inhibition |
| BMD gains (spine) | 9-13% at 18 months | 4-6% at 24 months | 6-9% at 24 months |
| BMD gains (hip) | 2-6% at 18 months | 2-4% at 24 months | 3-6% at 24 months |
| Fracture reduction | 65% vertebral, 53% non-vertebral | 47% vertebral, 20% non-vertebral | 68% vertebral, 20% non-vertebral |
| Administration | Daily subcutaneous injection | Weekly oral tablet | Every 6 months subcutaneous |
| Treatment duration | Maximum 2 years | Indefinite (drug holidays recommended) | Indefinite |
| Half-life | 1 hour | 10-12 years (bone binding) | 25 days |
| Onset of action | Days to weeks | 3-6 months | 1-3 months |
| Reversibility | Rapid (weeks to months) | Very slow (years) | Moderate (6-12 months) |
| Cost tier | High ($$$$) | Low ($) | High ($$$) |
| Common side effects | Nausea, hypercalcemia, injection site reactions | GI upset, musculoskeletal pain | Injection site reactions, hypocalcemia |
| Serious risks | Theoretical osteosarcoma risk | Atypical fractures, osteonecrosis of jaw | Rebound fractures, severe hypocalcemia |
| Best candidates | Severe osteoporosis, fracture healing | Prevention, mild-moderate osteoporosis | Severe osteoporosis, bisphosphonate intolerant |
Teriparatide vs. Abaloparatide
Abaloparatide (Tymlos) is a newer PTH-related protein analog that offers some advantages over teriparatide:
Efficacy comparison:
Spine BMD: Abaloparatide 9.2% vs teriparatide 6.8% at 18 months
Hip BMD: Abaloparatide 2.9% vs teriparatide 0.8% at 18 months
Vertebral fractures: Similar 80% reduction for both agents
Non-vertebral fractures: Abaloparatide 43% vs teriparatide 28% reduction
Safety profile:
Hypercalcemia: Abaloparatide 3.4% vs teriparatide 6.4%
Nausea: Similar rates (24-28% for both)
Injection site reactions: Abaloparatide 10.4% vs teriparatide 5.2%
Clinical considerations: Abaloparatide may be preferred for hip fracture prevention and in patients prone to hypercalcemia. Teriparatide has longer clinical experience and more fracture healing data.
Sequential vs. Combination Therapy
The optimal approach often involves sequential therapy rather than monotherapy:
Anabolic-first strategy (recommended for severe osteoporosis):
1. Teriparatide 18-24 months (build new bone)
2. Transition to bisphosphonate or denosumab (preserve gains)
3. Continue anti-resorptive therapy 3-5 years
Anti-resorptive-first approach (traditional method):
1. Bisphosphonate 3-5 years
2. Drug holiday or switch to teriparatide if fractures occur
3. Return to anti-resorptive therapy
Combination therapy (experimental):
Concurrent teriparatide + denosumab shows promise in trials
17% spine BMD gains at 12 months vs 8% for teriparatide alone
Significantly higher cost and unknown long-term safety
Evidence for sequencing: The DATA-Switch study demonstrated that starting with teriparatide followed by alendronate produces superior BMD gains compared to the reverse sequence (15.4% vs 6.3% spine BMD at 24 months).
What's Coming Next: The Future of Anabolic Bone Therapy
Biosimilar Competition and Access
The patent expiration of teriparatide in 2019 has opened the door for biosimilar versions that could dramatically improve access to anabolic bone therapy.
Approved biosimilars include:
Terrosa: (Teva): First FDA-approved teriparatide biosimilar in 2019
Bonsity: (Pfizer): European approval with US filing pending
Multiple other candidates in Phase III development
Cost implications: Biosimilars typically reduce costs by 30-50% once multiple competitors enter the market. Current teriparatide costs of $3,000-4,000 monthly could drop to $1,500-2,500, significantly improving patient access.
Clinical equivalence: Biosimilar trials demonstrate comparable efficacy and safety profiles to reference teriparatide, with BMD gains within 5% of original product performance.
Extended Duration Formulations
Researchers are developing long-acting teriparatide formulations to reduce injection frequency and improve compliance:
Weekly formulations: Encapsulation in microspheres or conjugation to albumin-binding domains could enable once-weekly dosing while maintaining pulsatile PTH exposure patterns.
Monthly depot injections: Biodegradable polymer systems are being tested that release teriparatide over 4-week periods. Early trials show comparable bone formation marker responses to daily injections.
Oral delivery systems: Novel delivery technologies including enteric-coated nanoparticles and absorption enhancers are being developed to overcome the peptide's poor oral bioavailability.
Combination Anabolic Agents
Next-generation bone anabolic therapies may combine multiple pathways for enhanced efficacy:
Teriparatide + Sclerostin inhibitors: Combining PTH receptor activation with sclerostin inhibition (romosozumab mechanism) could produce additive bone formation effects. Phase II trials are planned.
Dual-acting molecules: Engineered peptides that activate both PTH and Wnt signaling pathways simultaneously are in preclinical development, potentially offering superior anabolic effects.
Personalized dosing algorithms: Pharmacogenomic testing to identify optimal responders and AI-driven dosing protocols based on individual bone marker responses are being developed.
Expanded Clinical Applications
Pediatric bone disorders: Research is exploring teriparatide's potential in children with genetic bone diseases like osteogenesis imperfecta, where anabolic therapy might improve bone quality during growth.
Cancer-related bone loss: Trials are examining teriparatide's ability to prevent or reverse bone loss from cancer treatments, particularly aromatase inhibitors in breast cancer patients.
Implant integration: Orthopedic applications including enhanced osseointegration of joint replacements and dental implants are being investigated, with promising preclinical results.
Regenerative medicine: Combination with stem cell therapies, tissue engineering scaffolds, and growth factors for complex bone reconstruction represents a major research frontier.
Unanswered Research Questions
Several critical questions remain about optimizing teriparatide therapy:
Optimal treatment duration: While current guidelines limit treatment to 2 years, some experts question whether this restriction is necessary given the lack of human osteosarcoma cases. Studies of extended treatment periods are needed.
Retreatment protocols: Can patients safely receive multiple courses of teriparatide separated by anti-resorptive therapy? Limited data suggests this may be both safe and effective.
Biomarker-guided therapy: Which patients respond best to anabolic vs anti-resorptive therapy? Research into genetic markers, baseline bone turnover patterns, and other predictive factors could enable personalized treatment selection.
Optimal transition timing: When should patients switch from teriparatide to anti-resorptive therapy to maximize long-term benefits? Current recommendations are based on limited data.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Teriparatide's Revolutionary Impact
• Teriparatide represents the first truly anabolic bone therapy, building new bone tissue rather than just preventing loss, with spine BMD gains of 9-13% achievable within 18 months.
• The key to efficacy lies in pulsatile dosing — daily injections activate bone-building osteoblasts while continuous exposure would paradoxically increase bone destruction through osteoclast activation.
• Clinical evidence spans multiple applications, from reducing vertebral fractures by 65% in severe osteoporosis to accelerating fracture healing by 31% and improving spinal fusion rates to 94%.
• The 20 μg daily subcutaneous dose is optimal for most patients, established through extensive dose-finding studies and confirmed across diverse patient populations including postmenopausal women and men with osteoporosis.
• Treatment duration is limited to 24 months maximum due to theoretical osteosarcoma risk from rat studies, though post-marketing surveillance of 650,000+ patients shows no increased cancer risk in humans.
• Combination with optimized calcium/vitamin D and resistance exercise can enhance BMD gains by 15-40% compared to teriparatide alone, while sequential therapy with anti-resorptive agents maintains long-term benefits.
• Common side effects are generally mild and transient, including hypercalcemia in 11% of patients, injection site reactions in 28%, and nausea in 18-24%, with most resolving within the first month.
• Teriparatide works through PTH1 receptor activation, rapidly increasing cAMP and activating bone formation genes including RUNX2, osterix, and osteocalcin while enhancing Wnt signaling and IGF-1 production.
• The anabolic mechanism makes teriparatide uniquely effective for fracture healing, with particular benefits for complex cases like non-unions, atypical fractures, and challenging spinal fusions where other treatments fail.
• Future developments including biosimilars, extended-release formulations, and combination therapies promise to improve access, convenience, and efficacy while expanding applications to pediatric disorders and regenerative medicine.
Related Articles on BuyPeptidesOnline.com
BPC-157: The Wolverine Peptide That Regenerates Everything
TB-500: The Thymosin Beta-4 Fragment That Rewrites Tissue Repair
GHK-Cu: The Copper Peptide That Reverses Aging at the Cellular Level
IGF-1 LR3: The Extended Growth Factor That Rewrites Muscle Development
Complete Guide to Peptide Stacking for Enhanced Recovery