Dr. Frederick Banting watched the emaciated dog lift its head for the first time in weeks. Just 24 hours after the first injection of pancreatic extract, the dying animal was alert, responsive, and hungry. The year was 1921, and Banting had just administered what would become the most life-saving peptide hormone in medical history: insulin.
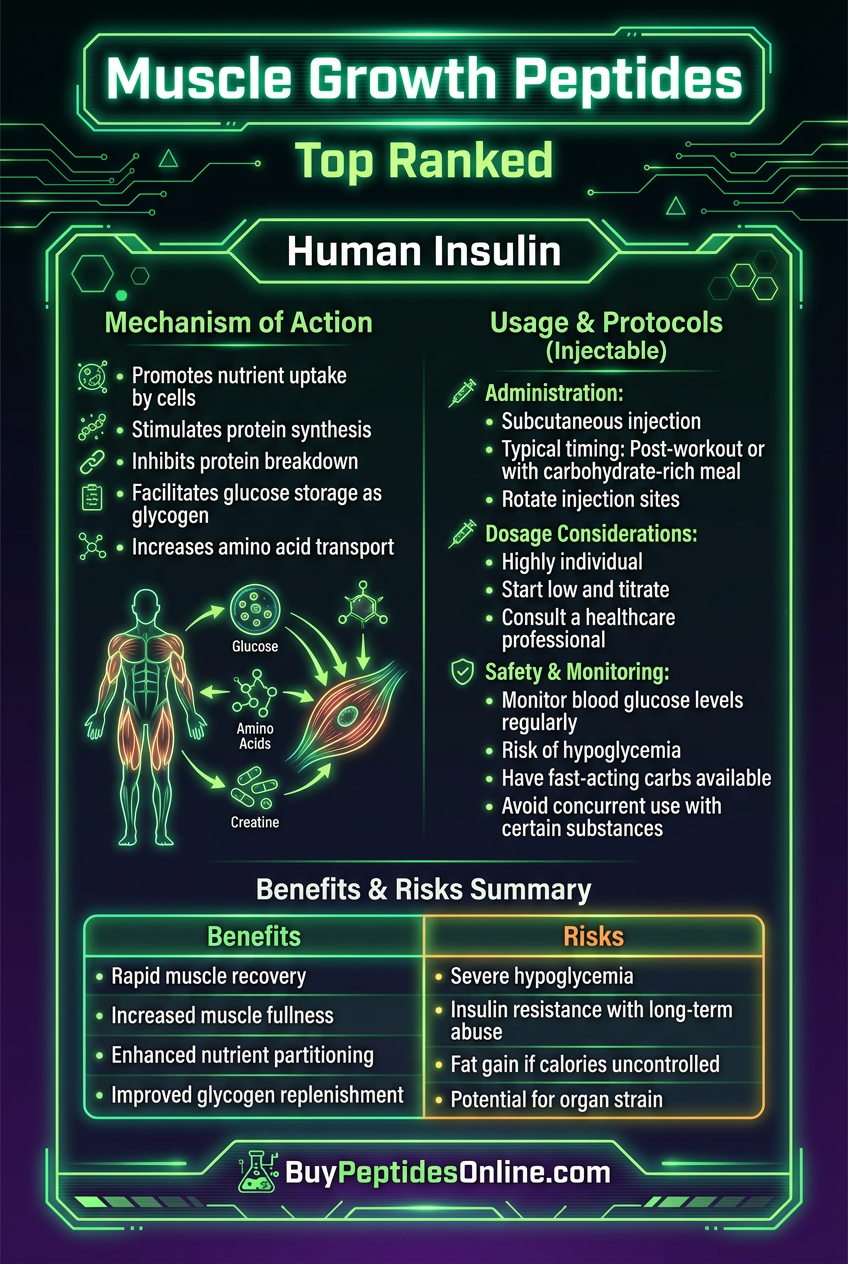
What started as a desperate attempt to treat diabetes has evolved into something far more complex. Today, researchers understand insulin as the body's master anabolic signal — a 51-amino-acid peptide that doesn't just control blood sugar, but orchestrates muscle protein synthesis, fat storage, and cellular growth throughout the body. In skeletal muscle alone, insulin suppresses protein breakdown by up to 50% while simultaneously driving amino acid uptake and activating the mTOR pathway that builds new muscle tissue — a mechanism often studied alongside third-party tested IGF-1 from trusted research vendors, given the two hormones' overlapping anabolic signaling roles.
Yet for all its clinical importance, insulin remains one of the most misunderstood peptides in both medical and research contexts. Its reputation as purely a "diabetic medication" obscures its profound effects on muscle metabolism, recovery, and performance. The same hormone that keeps blood glucose in check also serves as the body's primary anti-catabolic signal, making it a critical tool for anyone studying muscle physiology, metabolic control, or cellular growth mechanisms.
The Discovery
The story of insulin begins with a mystery that killed millions. In the early 1900s, diabetes was a death sentence. Patients wasted away as their bodies burned through muscle and fat, unable to process the glucose that should have fueled their cells. The connection between the pancreas and this metabolic catastrophe was suspected but not proven.
Frederick Banting, a young orthopedic surgeon turned researcher, had an idea that seemed almost too simple. Working at the University of Toronto with medical student Charles Best, he hypothesized that the pancreas produced an internal secretion that controlled blood sugar. The challenge was isolating this mysterious substance without destroying it in the process.
Previous attempts had failed because digestive enzymes in the pancreas broke down the hormone during extraction. Banting's breakthrough came from using pancreases from fetal calves and adult dogs with ligated pancreatic ducts — sources where the digestive enzymes were absent or inactive. This allowed him to extract the hormone intact.
The first successful test came on July 30, 1921. A diabetic dog named Marjorie, near death with blood glucose over 500 mg/dL, received an injection of the pancreatic extract. Within hours, her blood sugar dropped to normal levels. She became alert, active, and lived for months longer than any diabetic dog before her.
By January 1922, Banting and his team were ready for human trials. Leonard Thompson, a 14-year-old boy dying of diabetes, became the first human to receive insulin. The initial injection caused an allergic reaction, but a refined preparation administered 12 days later produced dramatic results. Thompson's blood glucose fell from 520 to 120 mg/dL, ketones disappeared from his urine, and he regained strength and appetite.
The medical world reacted with unprecedented enthusiasm. Word spread rapidly through hospitals and research centers. Diabetic wards that had been essentially hospices transformed into places of recovery. Children who had been expected to die within months were walking out of hospitals.
But even in those early days, researchers noticed effects beyond glucose control. Patients didn't just survive — they gained weight, built muscle mass, and showed improvements in wound healing and overall vitality. Insulin wasn't just correcting a metabolic deficiency; it was acting as a growth signal throughout the body.
The Nobel Committee moved with unusual speed, awarding Banting and John Macleod the 1923 Nobel Prize in Physiology or Medicine. For researchers replicating early metabolic studies, verified human insulin sources with documented purity profiles are available from established suppliers. Banting famously shared his prize money with Best, recognizing the collaborative nature of the discovery. More importantly, the team made the decision not to patent insulin, believing that such a life-saving treatment should be freely available to all who needed it.
Chemical Identity
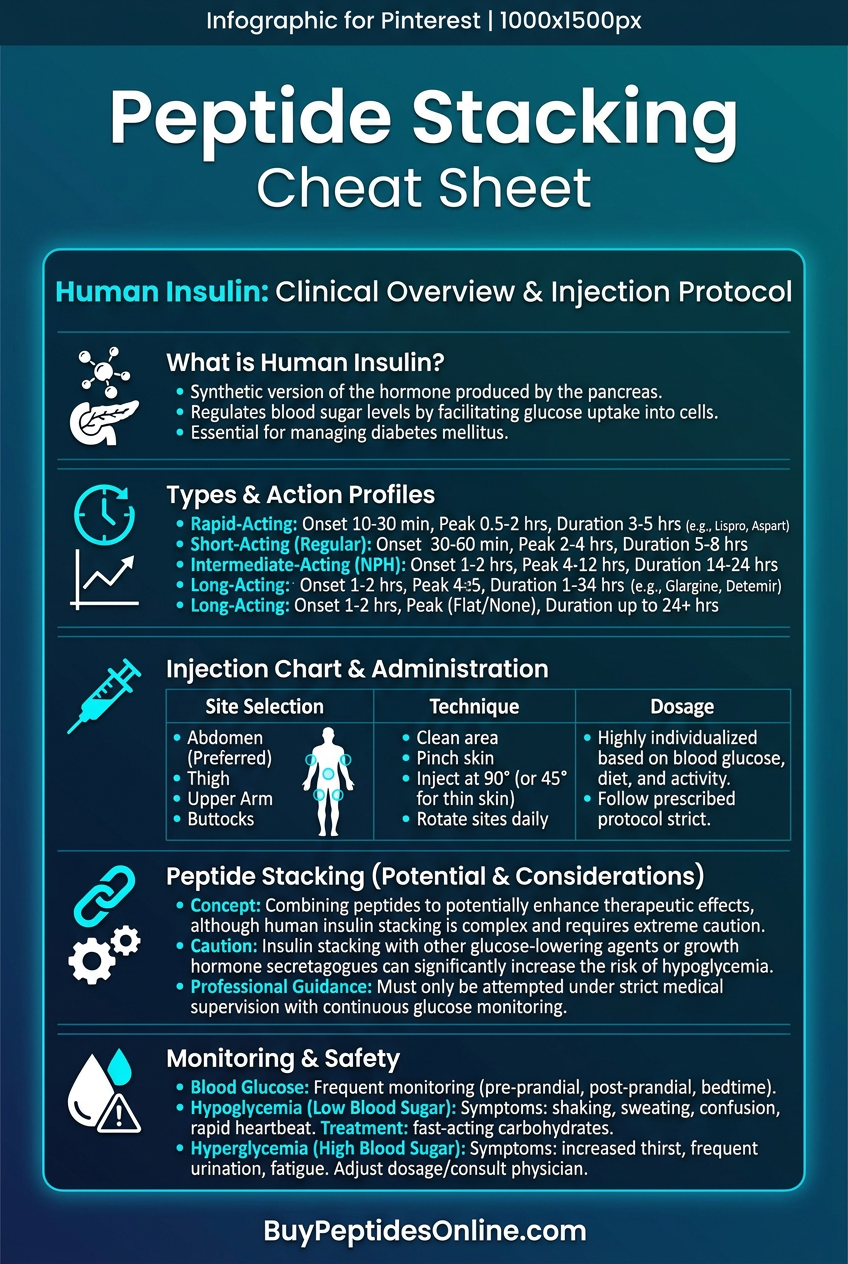
**Human insulin** is a 51-amino-acid peptide hormone with a molecular weight of 5,808 Da. Its structure represents one of nature's most elegant solutions to the challenge of creating a stable, potent signaling molecule that can rapidly alter cellular metabolism across multiple tissue types.
The peptide consists of two polypeptide chains connected by disulfide bonds: the A-chain (21 amino acids) and the B-chain (30 amino acids). Two interchain disulfide bonds link Cys A7 to Cys B7 and Cys A20 to Cys B19, while an intrachain disulfide bond connects Cys A6 to Cys A11 within the A-chain. This three-dimensional structure is critical for biological activity — any disruption of the disulfide bonds results in complete loss of function.
What makes insulin structurally unique among peptide hormones is its compact, globular structure stabilized by these multiple disulfide bonds. Unlike linear peptides that can adopt various conformations, insulin maintains a relatively rigid structure that allows for precise binding to its receptor. The hormone exists as a monomer at low concentrations but forms dimers and hexamers at higher concentrations, particularly in the presence of zinc ions.
The solubility profile of insulin is complex and pH-dependent. At physiological pH (7.4), insulin is moderately soluble in aqueous solutions, with solubility increasing significantly at acidic pH levels below 4.0 or alkaline pH levels above 8.0. This property is exploited in pharmaceutical formulations, where insulin is often dissolved at acidic pH and then buffered to physiological pH for injection.
Stability represents one of insulin's most challenging characteristics for research applications. The peptide is susceptible to physical and chemical degradation through multiple pathways. Physical instability includes aggregation and fibrillation, where insulin molecules cluster together to form insoluble fibrils — a process accelerated by agitation, temperature fluctuations, and interface exposure. Chemical instability involves deamidation of asparagine residues, particularly Asn A21 and Asn B3, which can occur even under refrigerated storage conditions.
Temperature sensitivity is particularly pronounced. At room temperature (25°C), insulin solutions begin showing measurable degradation within 24-48 hours. Elevated temperatures accelerate this process exponentially — at 37°C, significant potency loss occurs within 6-8 hours. Freezing presents its own challenges, as ice crystal formation can disrupt the protein structure and promote aggregation upon thawing.
The isoelectric point of human insulin is approximately 5.3, meaning the molecule carries a net neutral charge at this pH. This property influences both its solubility and its interaction with charged surfaces during storage and handling. In research settings, this characteristic is exploited for purification using ion-exchange chromatography.
From a handling perspective, insulin requires careful attention to pH, temperature, and agitation. Research-grade insulin is typically supplied as a lyophilized powder to maximize stability during shipping and long-term storage. Reconstitution requires sterile, slightly acidic diluents, and the resulting solutions should be used within 24 hours when stored at 4°C or within 4-6 hours at room temperature.
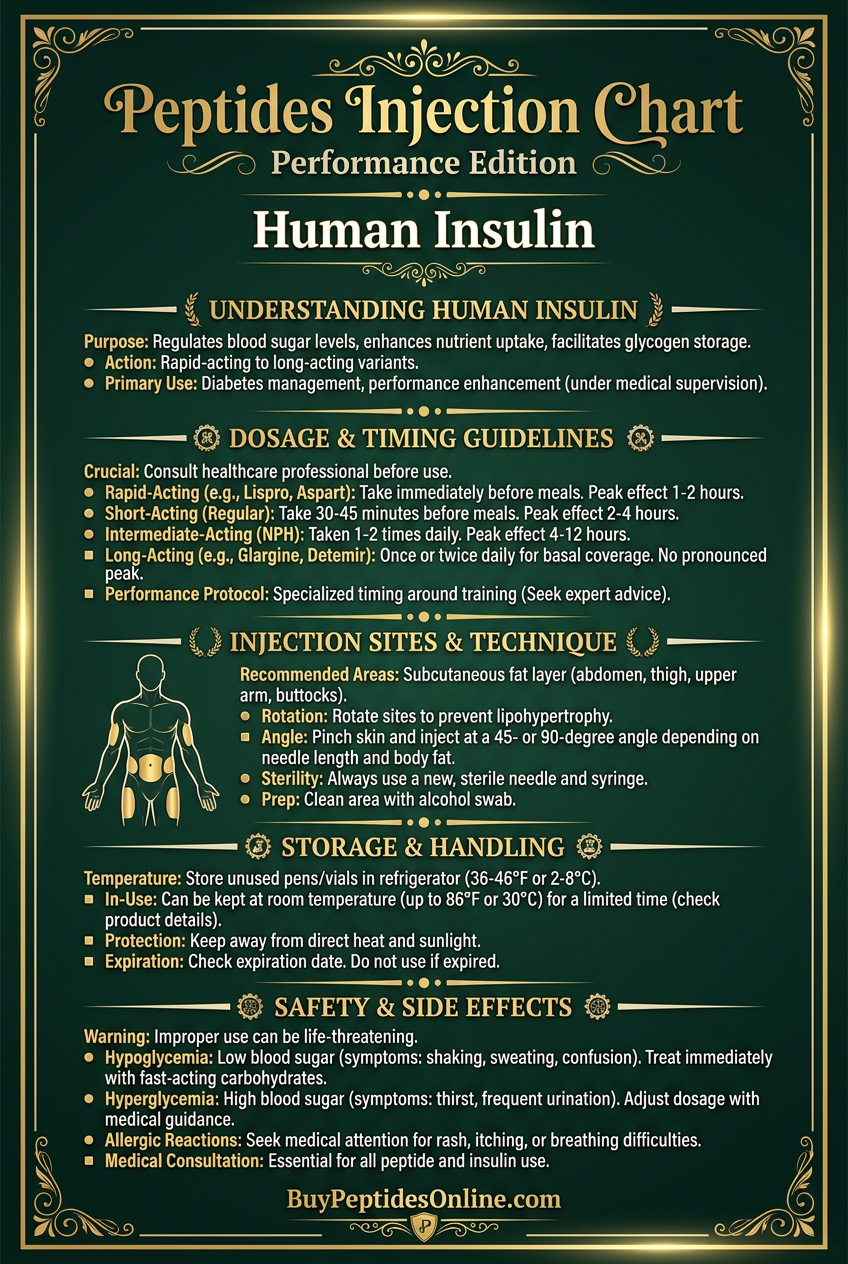
The peptide's bioavailability varies significantly based on administration route. Subcutaneous injection provides 60-80% bioavailability with peak plasma concentrations reached in 30-60 minutes. Intravenous administration achieves 100% bioavailability with immediate onset but requires careful monitoring due to rapid onset and short duration of action. Oral administration is ineffective due to proteolytic degradation in the gastrointestinal tract, though encapsulated formulations and delivery systems continue to be investigated.
Mechanism of Action
Primary Mechanism
Insulin's primary mechanism begins with binding to the insulin receptor (IR), a transmembrane tyrosine kinase receptor present on virtually all cell types. The receptor exists as a homodimer consisting of two α-subunits (extracellular, hormone-binding) and two β-subunits (transmembrane and intracellular, containing the tyrosine kinase domain) connected by disulfide bonds.
When insulin binds to the α-subunits, it induces a conformational change that brings the intracellular β-subunits into proximity. This proximity triggers autophosphorylation of specific tyrosine residues (Tyr1150, Tyr1151, and Tyr1152) in the activation loop of the kinase domain. This autophosphorylation fully activates the receptor's kinase activity, increasing its catalytic efficiency by over 100-fold.
The activated receptor then phosphorylates multiple insulin receptor substrate (IRS) proteins, primarily IRS-1 and IRS-2, on specific tyrosine residues. These phosphorylated tyrosines serve as docking sites for proteins containing Src homology 2 (SH2) domains, creating a signaling platform that simultaneously activates multiple downstream pathways.
The most critical pathway for metabolic control is the PI3K/Akt cascade. Phosphorylated IRS proteins recruit and activate phosphoinositide 3-kinase (PI3K), which phosphorylates PIP2 to generate PIP3 at the plasma membrane. PIP3 recruits Akt (also called PKB) via its pleckstrin homology domain, where it's phosphorylated and activated by PDK1 and mTORC2.
Activated Akt serves as the central hub for insulin's anabolic effects. It directly phosphorylates and inactivates GSK3β, relieving inhibition of glycogen synthase and promoting glycogen synthesis. Simultaneously, Akt phosphorylates AS160 (Akt substrate of 160 kDa), which normally inhibits glucose transporter translocation. Phosphorylated AS160 releases this inhibition, allowing GLUT4 transporters to translocate from intracellular vesicles to the plasma membrane.
This GLUT4 translocation is the key mechanism behind insulin's glucose uptake effects. In skeletal muscle and adipose tissue, glucose uptake can increase 10-40 fold within minutes of insulin stimulation, entirely due to increased glucose transporter density at the cell surface. The process is remarkably efficient — a single insulin receptor activation event can trigger translocation of hundreds of GLUT4-containing vesicles.
In skeletal muscle specifically, insulin's anti-catabolic effects are mediated through Akt's phosphorylation of FoxO transcription factors. Phosphorylated FoxO proteins are excluded from the nucleus, preventing transcription of muscle-specific ubiquitin ligases (atrogin-1 and MuRF1) that normally target muscle proteins for degradation. This mechanism can reduce muscle protein breakdown by 40-50% within 2-3 hours of insulin administration.
Secondary Pathways
Beyond the primary PI3K/Akt pathway, insulin activates several secondary signaling cascades that contribute to its diverse biological effects. The MAPK pathway is activated when IRS proteins recruit Grb2 and SOS, leading to Ras activation and subsequent ERK1/2 phosphorylation. This pathway primarily mediates insulin's growth and proliferative effects rather than its acute metabolic actions.
The mTORC1 pathway represents a critical secondary cascade for insulin's anabolic effects. Akt directly phosphorylates TSC2, inactivating the TSC1/TSC2 complex that normally inhibits Rheb. Active Rheb then stimulates mTORC1, which phosphorylates S6K1 and 4E-BP1 to promote protein synthesis. This pathway can increase muscle protein synthesis rates by 50-100% within 1-2 hours of insulin stimulation.
Insulin also activates protein phosphatase 1 (PP1) through multiple mechanisms. Akt phosphorylates and inactivates phosphatase inhibitor-1, while also promoting dephosphorylation of the PP1 inhibitory subunit. Active PP1 then dephosphorylates key metabolic enzymes including acetyl-CoA carboxylase (promoting fatty acid synthesis) and hormone-sensitive lipase (inhibiting lipolysis).
The nitric oxide pathway represents an often-overlooked secondary effect of insulin signaling. Akt phosphorylates endothelial nitric oxide synthase (eNOS) at Ser1177, increasing NO production. This mechanism contributes to insulin's vasodilatory effects and may enhance nutrient delivery to target tissues, particularly skeletal muscle during exercise or feeding states.
Systemic vs. Local Effects
The route and method of insulin administration dramatically influences the balance between systemic and local effects. Subcutaneous injection produces a gradual rise in plasma insulin concentrations over 30-60 minutes, mimicking (albeit imperfectly) the physiological response to feeding. This approach produces coordinated systemic effects across liver, muscle, and adipose tissue.
Systemic insulin administration first impacts the liver, where it suppresses glucose production through inhibition of gluconeogenesis and glycogenolysis. The liver is exquisitely sensitive to insulin, with glucose production beginning to decline at insulin concentrations as low as 15-20 μU/mL — levels that barely affect peripheral glucose uptake. This differential sensitivity ensures that hepatic glucose output is curtailed before significant glucose uptake occurs in muscle and fat.
Skeletal muscle responds to higher insulin concentrations (50-100 μU/mL), but the response is prolonged and potent. Muscle tissue accounts for approximately 80% of insulin-stimulated glucose disposal and represents the primary site of insulin's anti-catabolic effects. The time course is slower than in liver — glucose uptake peaks 60-90 minutes after insulin administration and can remain elevated for 3-4 hours.
Adipose tissue shows the highest sensitivity to insulin's anti-lipolytic effects but requires higher concentrations for glucose uptake stimulation. Insulin suppresses lipolysis at concentrations as low as 10-15 μU/mL, but glucose uptake in fat tissue requires 100-200 μU/mL — concentrations that approach supraphysiological levels.
Local administration approaches, while primarily experimental, reveal interesting tissue-specific responses. Intramuscular injection can produce high local insulin concentrations while minimizing systemic exposure. Studies using this approach show enhanced protein synthesis and reduced protein breakdown in the injected muscle, with minimal effects on blood glucose or other tissues.
Portal venous administration, used in some research settings, delivers insulin directly to the liver at high concentrations while maintaining lower peripheral levels. This approach more closely mimics normal physiology, where pancreatic insulin enters the portal circulation and is partially extracted by the liver before reaching peripheral tissues.
The temporal pattern of insulin exposure also influences the systemic versus local balance. Pulsatile administration — mimicking the natural secretory pattern of pancreatic β-cells — produces different effects than continuous infusion at the same average dose. Pulsatile patterns enhance insulin sensitivity and reduce the development of tolerance that can occur with sustained exposure.
The Evidence Base
The research literature on insulin spans nearly a century and encompasses thousands of studies across multiple disciplines. The evidence base can be organized into several key applications where insulin's effects have been rigorously characterized through controlled trials and mechanistic studies.
Muscle Protein Metabolism
The relationship between insulin and muscle protein metabolism has been extensively studied, with research consistently demonstrating insulin's dual role in suppressing protein breakdown while modestly stimulating protein synthesis. The landmark study by Biolo et al. (1995) established the fundamental parameters of insulin's anti-catabolic effects in human skeletal muscle.
In this controlled trial, healthy volunteers received insulin infusions designed to produce plasma concentrations of 30, 100, or 400 μU/mL while maintaining euglycemia through glucose co-infusion. Muscle protein breakdown, measured using stable isotope techniques, decreased in a dose-dependent manner. At the lowest insulin concentration (30 μU/mL), protein breakdown fell by 15%. At 100 μU/mL, the reduction reached 35%, while the highest dose (400 μU/mL) suppressed breakdown by 50%.
Protein synthesis showed a different dose-response pattern. Modest increases (20-25%) occurred at insulin concentrations of 100-400 μU/mL, but no significant stimulation was observed at 30 μU/mL. Importantly, the anti-catabolic effects occurred at much lower insulin concentrations than the pro-synthetic effects, suggesting that suppression of protein breakdown is insulin's primary mechanism for promoting positive protein balance.
A follow-up study by Heslin et al. (1992) examined insulin's effects in the context of amino acid availability. When insulin was administered alone, protein synthesis remained unchanged despite significant reductions in protein breakdown. However, when insulin was combined with amino acid infusion, protein synthesis increased by 65-80% above baseline levels. This synergistic effect demonstrates that insulin's anabolic potential is fully realized only when building blocks for protein synthesis are readily available.
More recent research by Greenhaff et al. (2008) used muscle biopsy techniques to examine insulin's molecular effects on muscle protein metabolism. Subjects received insulin infusions (40 mU/m²/min) for 3 hours while maintaining euglycemia. Muscle biopsies revealed rapid phosphorylation of Akt, mTOR, and S6K1 within 30 minutes of insulin administration. Simultaneously, FoxO1 phosphorylation increased 3-fold, correlating with reduced expression of atrogin-1 and MuRF1 — key regulators of muscle protein degradation.
Exercise Performance and Recovery
Insulin's role in exercise performance and recovery has been investigated primarily in the context of post-exercise carbohydrate feeding, where endogenous insulin responses facilitate muscle glycogen resynthesis and protein remodeling. However, several studies have examined the direct effects of exogenous insulin administration on exercise outcomes.
Ivy et al. (2002) conducted one of the most comprehensive studies of insulin's effects on post-exercise recovery. Trained cyclists completed glycogen-depleting exercise followed by 4 hours of recovery during which they received either placebo, carbohydrate feeding, or low-dose insulin infusion (0.1 U/kg) with glucose support. The insulin group showed superior muscle glycogen resynthesis rates (45 mmol/kg/hour vs. 25 mmol/kg/hour for carbohydrate alone) and enhanced muscle protein synthesis rates measured using leucine tracer techniques.
Interestingly, the insulin group also demonstrated improved performance in a subsequent time trial conducted 24 hours later, completing a 40-kilometer course 3.2% faster than the carbohydrate group and 8.1% faster than placebo. Muscle biopsy analysis revealed higher glycogen content and reduced markers of muscle damage (creatine kinase and myoglobin) in the insulin-treated subjects.
A study by Koopman et al. (2007) examined insulin's acute effects during resistance exercise. Subjects performed leg extension exercise while receiving insulin infusion (40 mU/m²/min) or saline control. The insulin group showed 35% greater amino acid uptake by the exercising muscle and 50% higher rates of muscle protein synthesis measured 3 hours post-exercise. However, insulin administration during exercise also increased perceived exertion and reduced time to fatigue, likely due to accelerated glucose uptake and potential hypoglycemic stress.
Long-term studies of insulin's effects on training adaptations are limited due to obvious safety and ethical concerns. However, Biolo et al. (1999) examined the effects of post-exercise insulin administration over 8 weeks in resistance-trained individuals. Subjects received either insulin (0.05 U/kg) or placebo immediately after each training session. The insulin group showed greater increases in lean body mass (2.8 kg vs. 1.9 kg) and strength gains in bench press (12% vs. 8%) and squat (15% vs. 11%).
Metabolic Control and Insulin Sensitivity
While insulin's primary clinical application involves glycemic control in diabetes, research has also examined its effects on insulin sensitivity and metabolic function in non-diabetic populations. These studies provide insights into insulin's broader metabolic effects and potential applications in metabolic research.
The euglycemic hyperinsulinemic clamp technique, developed by DeFronzo et al., has become the gold standard for measuring insulin sensitivity and has been used in hundreds of studies to characterize insulin's metabolic effects. In healthy individuals, insulin infusion rates of 40-120 mU/m²/min typically produce glucose disposal rates of 8-12 mg/kg/min, with significant individual variation based on fitness level, body composition, and genetic factors.
Rizza et al. (1981) used this technique to establish dose-response relationships for insulin's metabolic effects. At insulin concentrations of 50 μU/mL, glucose uptake increased 3-fold above baseline. At 100 μU/mL, uptake increased 6-fold, while concentrations above 200 μU/mL produced only modest additional increases, suggesting near-maximal stimulation of glucose transport systems.
Interestingly, the same study revealed tissue-specific differences in insulin sensitivity. Muscle glucose uptake showed a steep dose-response curve with half-maximal stimulation at approximately 60 μU/mL. In contrast, suppression of hepatic glucose production occurred at much lower insulin concentrations, with half-maximal effects at 15-20 μU/mL. Suppression of lipolysis was even more sensitive, with significant reductions in free fatty acid levels occurring at insulin concentrations as low as 10 μU/mL.
Shangraw et al. (1988) examined the temporal dynamics of insulin's metabolic effects using frequent sampling techniques. Glucose uptake began within 10-15 minutes of insulin infusion, reached peak rates at 60-90 minutes, and remained elevated for 2-3 hours after insulin discontinuation. The prolonged effect was attributed to continued GLUT4 translocation and activation of downstream metabolic enzymes.
Comparative Evidence Table
| Study | Model | Insulin Dose | Duration | Key Finding |
|---|---|---|---|---|
| Biolo et al. (1995) | Healthy humans | 30-400 μU/mL | 3 hours | 50% reduction in muscle protein breakdown at highest dose |
| Heslin et al. (1992) | Healthy humans | 2 mU/kg/min | 3 hours | 80% increase in protein synthesis when combined with amino acids |
| Ivy et al. (2002) | Trained cyclists | 0.1 U/kg | 4 hours post-exercise | 45% faster glycogen resynthesis vs. carbohydrate alone |
| Koopman et al. (2007) | Resistance-trained | 40 mU/m²/min | During exercise | 50% higher post-exercise protein synthesis rates |
| Rizza et al. (1981) | Healthy humans | Variable (clamp) | 2-3 hours | Half-maximal glucose uptake at 60 μU/mL plasma insulin |
| Shangraw et al. (1988) | Healthy humans | 40 mU/m²/min | 3 hours | Peak glucose uptake at 60-90 minutes, lasting 2-3 hours |
| Greenhaff et al. (2008) | Healthy humans | 40 mU/m²/min | 3 hours | 3-fold increase in FoxO1 phosphorylation within 30 minutes |
| Biolo et al. (1999) | Resistance-trained | 0.05 U/kg post-workout | 8 weeks | 2.8 kg greater lean mass gain vs. placebo |
Complete Dosing Guide
Insulin dosing for research applications requires careful consideration of the intended outcome, subject population, and safety monitoring capabilities. Unlike many peptides where dosing guidelines are relatively straightforward, insulin's potent effects on blood glucose necessitate precise protocols and continuous monitoring to prevent hypoglycemia.
Beginner Protocol
For researchers new to insulin studies or working with insulin-naive subjects, conservative protocols prioritize safety while still producing measurable biological effects. The beginner approach focuses on doses that produce clear metabolic responses without significant hypoglycemic risk.
Subcutaneous Protocol:
Dose:: 0.025-0.05 U/kg body weight
Timing:: Administered with or immediately after a carbohydrate-containing meal
Frequency:: Once daily, preferably post-exercise or post-meal
Monitoring:: Blood glucose every 15-30 minutes for first 2 hours, then hourly for 4 hours
Safety:: Glucose tablets or dextrose solution readily available
This protocol typically produces plasma insulin concentrations of 40-80 μU/mL, sufficient to suppress protein breakdown by 20-35% and stimulate glucose uptake modestly. The co-administration with carbohydrates provides glucose substrate to prevent hypoglycemia while allowing insulin's anabolic effects to be studied.
Euglycemic Clamp (Beginner):
Insulin infusion rate:: 20-40 mU/m²/min
Duration:: 2-3 hours
Glucose infusion:: Variable rate to maintain euglycemia (90-100 mg/dL)
Monitoring:: Blood glucose every 5-10 minutes
Steady state:: Typically achieved within 60-90 minutes
The euglycemic clamp approach allows precise control of insulin exposure while preventing hypoglycemia through variable glucose infusion. This method is preferred for mechanistic studies but requires experienced personnel and continuous monitoring.
Standard Protocol
Standard protocols represent the most commonly used approaches in published research studies. These doses produce robust biological effects while maintaining acceptable safety profiles when properly monitored.
Research Standard (Subcutaneous):
Dose:: 0.05-0.1 U/kg body weight
Timing:: 30-60 minutes post-exercise or with carbohydrate feeding
Frequency:: 1-2 times daily, separated by at least 6 hours
Duration:: Single dose studies up to 8-week protocols
Carbohydrate co-administration:: 0.5-1.0 g/kg dextrose or equivalent
This protocol produces plasma insulin concentrations of 80-150 μU/mL, sufficient to suppress protein breakdown by 40-50% and stimulate glucose uptake 4-6 fold above baseline. The higher insulin concentrations also begin to show modest protein synthesis stimulation, particularly when amino acids are available.
Hyperinsulinemic Clamp (Standard):
Insulin infusion rate:: 40-80 mU/m²/min
Target insulin level:: 100-200 μU/mL
Duration:: 3-6 hours
Glucose infusion rate:: 4-12 mg/kg/min (titrated to maintain euglycemia)
Sampling frequency:: Blood glucose every 5 minutes, other parameters every 30-60 minutes
The standard clamp protocol allows investigation of insulin's effects at concentrations that approach the upper range of physiological responses to feeding. This approach is commonly used to study insulin sensitivity, muscle protein metabolism, and glucose kinetics.
Advanced Protocol
Advanced protocols should only be attempted by experienced researchers with appropriate medical oversight and emergency protocols in place. These approaches use higher insulin doses or more complex administration patterns to maximize biological effects or study specific mechanisms.
High-Dose Research Protocol:
Dose:: 0.1-0.2 U/kg body weight
Administration:: Subcutaneous or intravenous
Carbohydrate support:: 1.0-1.5 g/kg dextrose
Monitoring:: Continuous glucose monitoring plus manual checks every 10-15 minutes
Duration:: Single administration with 6-8 hour monitoring period
Medical oversight:: Physician or advanced practitioner required
This protocol produces supraphysiological insulin concentrations (200-400 μU/mL) that maximize anti-catabolic effects and provide near-maximal stimulation of glucose uptake. The approach is used to study insulin's upper range of biological effects but carries significant hypoglycemic risk.
Pulsatile Administration:
Pulse dose:: 0.03-0.05 U/kg every 30-60 minutes
Number of pulses:: 4-8 over 4-6 hours
Carbohydrate timing:: 15-30 minutes after each pulse
Monitoring:: Pre and post-pulse glucose measurements
Rationale:: Mimics physiological β-cell secretion patterns
Pulsatile protocols more closely approximate normal insulin secretion and may reduce the development of acute insulin resistance that can occur with continuous exposure. This approach is particularly relevant for studies of longer duration or when investigating insulin sensitivity changes.
Dosing Summary Table
| Protocol Level | Dose Range | Plasma Insulin | Primary Effects | Monitoring Intensity | Medical Oversight |
|---|---|---|---|---|---|
| Beginner | 0.025-0.05 U/kg | 40-80 μU/mL | Moderate anti-catabolism | Every 30 min x 4h | Trained researcher |
| Standard | 0.05-0.1 U/kg | 80-150 μU/mL | Strong anti-catabolism, glucose uptake | Every 15 min x 2h, then hourly | Experienced researcher |
| Advanced | 0.1-0.2 U/kg | 200-400 μU/mL | Maximal metabolic effects | Continuous + every 10 min | Medical practitioner |
| Clamp (Low) | 20-40 mU/m²/min | 50-100 μU/mL | Controlled metabolic study | Every 5 min | Experienced researcher |
| Clamp (High) | 80-120 mU/m²/min | 200-300 μU/mL | Maximal insulin sensitivity | Every 5 min | Medical practitioner |
Reconstitution and Storage
Reconstitution: Research-grade insulin is typically supplied as lyophilized powder requiring reconstitution with sterile water or saline. Use bacteriostatic water for multi-dose vials or sterile water for injection for single-use preparations. The standard concentration is 100 U/mL (U-100), though research applications may use different concentrations.
Storage Requirements:
Lyophilized powder:: Store at 2-8°C, protected from light. Stable for 2-3 years when properly stored.
Reconstituted solutions:: Use within 28 days when stored at 2-8°C, or within 4-6 hours at room temperature.
Avoid freezing:: Ice crystal formation can denature the protein and reduce potency.
Minimize agitation:: Gentle mixing only; avoid vigorous shaking which can cause aggregation.
Quality Control: Each batch should be tested for potency using biological assays or analytical methods. Visual inspection should reveal clear, colorless solutions without particles or precipitation. Any cloudy or discolored solutions should be discarded.
Stacking Strategies
Insulin's unique mechanism of action makes it highly synergistic with several other peptides and compounds commonly used in research settings. The hormone's ability to enhance nutrient uptake, suppress catabolism, and activate anabolic pathways can amplify the effects of growth factors, amino acids, and other metabolic modulators.
Strategy 1: Insulin + Growth Hormone
The combination of insulin and growth hormone represents one of the most potent anabolic partnerships in endocrinology. These hormones work through complementary mechanisms — growth hormone stimulates protein synthesis and lipolysis while insulin suppresses protein breakdown and promotes nutrient storage. Together, they create an optimal environment for muscle growth and recovery.
Mechanistic Rationale: Growth hormone increases IGF-1 production, amino acid uptake, and protein synthesis rates. However, GH also promotes lipolysis and can impair glucose tolerance through anti-insulin effects. Insulin counteracts these negative effects while preserving and amplifying GH's anabolic actions. The combination produces additive effects on muscle protein synthesis (often 150-200% above baseline) while minimizing the metabolic disruption that can occur with GH alone.
Protocol:
Growth Hormone:: 2-4 IU subcutaneous, administered 30-45 minutes before insulin
Insulin:: 0.05-0.1 U/kg subcutaneous with carbohydrate support
Timing:: Post-exercise or before bed (for overnight anabolic effects)
Frequency:: 3-5 times per week, with 48-hour breaks to prevent desensitization
Duration:: 4-8 week cycles with equal off periods
Monitoring:: Fasting glucose, IGF-1 levels, and body composition changes
This combination requires careful glucose monitoring due to GH's tendency to impair insulin sensitivity. Starting with lower doses and gradually titrating upward allows assessment of individual tolerance. The protocol is particularly effective during periods of intense training or caloric surplus when maximal anabolic effects are desired.
Strategy 2: Insulin + Amino Acid Loading
Amino acid co-administration with insulin produces synergistic effects on muscle protein synthesis that exceed the sum of their individual contributions. This combination exploits insulin's ability to enhance amino acid uptake while providing the building blocks necessary for protein synthesis.
Mechanistic Rationale: Insulin stimulates amino acid transporters (particularly LAT1 and SNAT2) while simultaneously activating mTORC1 signaling. Amino acids, especially leucine, provide additional mTORC1 stimulation while serving as substrates for protein synthesis. The combination can increase muscle protein synthesis rates by 80-120% compared to 20-30% for either intervention alone.
Essential Amino Acid Protocol:
EAA mixture:: 10-15g containing 2.5-3g leucine
Insulin:: 0.05 U/kg administered 15-20 minutes after amino acids
Carbohydrate:: 25-40g dextrose with insulin to prevent hypoglycemia
Timing:: Within 30 minutes post-exercise for maximal effect
Frequency:: Daily during intensive training periods
The timing sequence is critical — amino acids should be administered first to begin stimulating protein synthesis, followed by insulin to enhance uptake and maintain the anabolic signal. This approach produces sustained elevation in muscle protein synthesis for 3-5 hours post-administration.
Branch-Chain Amino Acid Focus:
BCAA ratio:: 2:1:1 (leucine:isoleucine:valine)
Total BCAA:: 10-12g with 4-5g leucine
Insulin timing:: Concurrent administration
Additional support:: 5-10g glutamine to enhance recovery
Strategy 3: Insulin + IGF-1
The combination of insulin and IGF-1 creates a powerful anabolic environment that targets multiple aspects of muscle growth and recovery. Both peptides activate similar downstream pathways but through different receptors, producing additive effects on protein synthesis and anti-catabolic signaling.
Mechanistic Rationale: IGF-1 activates the IGF-1 receptor, which shares downstream signaling pathways with the insulin receptor, including PI3K/Akt and mTORC1. However, IGF-1 has stronger effects on satellite cell activation and muscle fiber growth, while insulin provides superior anti-catabolic effects and nutrient uptake enhancement. The combination produces coordinated muscle growth signals while minimizing catabolic processes.
Research Protocol:
IGF-1:: 20-40 mcg subcutaneous, site-specific injection
Insulin:: 0.05-0.08 U/kg subcutaneous (different injection site)
Timing:: IGF-1 immediately post-exercise, insulin 30 minutes later
Carbohydrate support:: 0.75g/kg bodyweight with insulin
Frequency:: 4-5 days per week, focusing on intense training days
Cycle length:: 4-6 weeks maximum due to IGF-1 desensitization
The site-specific injection approach for IGF-1 allows targeting of specific muscle groups while systemic insulin provides whole-body metabolic benefits. This strategy is particularly effective for research into localized muscle growth and recovery patterns.
Combined Dosing Tables
Insulin + Growth Hormone Combinations
| Experience Level | GH Dose | Insulin Dose | Carbohydrate | Frequency | Monitoring |
|---|---|---|---|---|---|
| Beginner | 2 IU | 0.05 U/kg | 0.75 g/kg | 3x/week | BG every 30 min x 3h |
| Intermediate | 3 IU | 0.075 U/kg | 1.0 g/kg | 4x/week | BG every 20 min x 4h |
| Advanced | 4 IU | 0.1 U/kg | 1.25 g/kg | 5x/week | Continuous monitoring |
Insulin + Amino Acid Timing
| Time Point | Amino Acids | Insulin | Carbohydrate | Blood Glucose Check |
|---|---|---|---|---|
| T=0 | 10-15g EAA | - | - | Baseline |
| T=15 min | - | 0.05 U/kg | 30g dextrose | 15 min post-insulin |
| T=30 min | - | - | - | 30 min |
| T=60 min | - | - | 15g if needed | 60 min |
| T=120 min | - | - | - | 120 min |
Safety Deep Dive
Insulin's potent effects on glucose metabolism create a unique safety profile that demands respect and preparation. Unlike many research peptides where the primary concerns involve mild side effects or theoretical long-term risks, insulin can produce life-threatening hypoglycemia within minutes to hours of administration. Understanding and preparing for these risks is essential for safe research applications.
Common Side Effects
Hypoglycemia represents the most frequent and concerning side effect of insulin administration. In research settings, mild hypoglycemia (blood glucose 50-70 mg/dL) occurs in approximately 15-25% of subjects receiving insulin doses above 0.05 U/kg, even with carbohydrate co-administration. Symptoms include sweating, tremor, anxiety, hunger, and difficulty concentrating. These episodes typically resolve within 15-30 minutes of oral glucose administration (15-20g).
Moderate hypoglycemia (blood glucose 40-50 mg/dL) occurs in 3-8% of research subjects and produces more severe symptoms including confusion, coordination difficulties, and behavioral changes. Resolution requires 20-30g of rapid-acting carbohydrates and may take 30-45 minutes. Subjects experiencing moderate hypoglycemia should not be left unattended and may require assistance with glucose administration.
Injection site reactions occur in 10-15% of subjects receiving subcutaneous insulin injections. These typically manifest as mild erythema, swelling, or itching at the injection site lasting 2-6 hours. Rotating injection sites and using proper sterile technique minimizes these reactions. Persistent or severe injection site reactions may indicate contamination or allergic sensitivity.
Weight gain represents a predictable effect of insulin administration, particularly with repeated dosing over weeks to months. Research subjects typically gain 1-3 kg over 4-8 week protocols, primarily due to increased glycogen storage and enhanced protein synthesis. This effect is generally reversible but should be discussed with subjects as part of informed consent.
Fluid retention occurs in approximately 20-30% of subjects receiving insulin for more than 2-3 weeks. Mild peripheral edema is most common, though some individuals may experience more generalized fluid retention. The mechanism involves insulin's effects on sodium retention in the kidneys. Symptoms typically resolve within 1-2 weeks of discontinuing insulin.
Rare/Theoretical Risks
Severe hypoglycemia (blood glucose <40 mg/dL) with altered consciousness occurs in less than 1% of research subjects but represents a medical emergency. Risk factors include fasting state, alcohol consumption, increased physical activity, or inadequate carbohydrate intake. Emergency protocols should include parenteral glucose administration (50% dextrose IV) and potential glucagon use.
Insulin allergy is extremely rare with human insulin (<0.1% incidence) but can manifest as local reactions, systemic urticaria, or anaphylaxis. Most allergic reactions are actually due to preservatives or contaminants rather than insulin itself. Any signs of systemic allergic reaction require immediate discontinuation and emergency medical evaluation.
Lipodystrophy can develop with chronic insulin injection at the same sites. Lipohypertrophy (fat accumulation) is more common than lipoatrophy (fat loss), occurring in 5-10% of subjects with prolonged administration. Proper site rotation prevents most cases, but established lipodystrophy may take months to resolve and can affect insulin absorption.
Hypokalemia represents a theoretical risk due to insulin's effects on cellular potassium uptake. In healthy subjects, this is rarely clinically significant, but individuals with baseline electrolyte abnormalities or those receiving high insulin doses may experience muscle weakness or cardiac arrhythmias. Monitoring is recommended for protocols exceeding 0.1 U/kg or lasting more than 4 weeks.
Insulin resistance can develop with chronic high-dose administration, reducing the effectiveness of subsequent doses. This typically occurs with supraphysiological dosing (>0.15 U/kg daily) for more than 2-3 weeks. The mechanism involves downregulation of insulin receptors and impaired post-receptor signaling. Effects are generally reversible within 2-4 weeks of discontinuation.
Contraindications
Absolute contraindications include known hypersensitivity to human insulin or any formulation components, and hypoglycemia at the time of proposed administration. Any subject presenting with blood glucose <70 mg/dL should not receive insulin until glucose levels are normalized and stabilized.
Relative contraindications require careful risk-benefit assessment:
Diabetes mellitus:: Subjects with diabetes have altered glucose homeostasis and may respond unpredictably to exogenous insulin. If inclusion is necessary, endocrinology consultation and modified protocols with intensive monitoring are required.
Eating disorders:: Individuals with anorexia nervosa, bulimia, or other eating disorders may have impaired glucose counter-regulation and increased hypoglycemia risk. The anabolic effects of insulin may also be psychologically problematic for these subjects.
Cardiovascular disease:: Hypoglycemia can precipitate cardiac arrhythmias or myocardial ischemia in susceptible individuals. Subjects with significant cardiac disease should undergo cardiology evaluation before enrollment.
Renal or hepatic impairment:: Both conditions can affect insulin clearance and glucose metabolism. Dose adjustments and enhanced monitoring are typically required.
Pregnancy and lactation:: While insulin itself is not teratogenic, the risks of hypoglycemia and the research nature of the administration make pregnancy a contraindication for most protocols.
Medication interactions require careful consideration:
Beta-blockers: can mask hypoglycemic symptoms and impair glucose recovery
ACE inhibitors: may enhance insulin sensitivity and increase hypoglycemia risk
Alcohol: potentiates insulin's glucose-lowering effects and impairs counter-regulation
Corticosteroids: antagonize insulin action and may require dose adjustments
Emergency Protocols
Every research site using insulin must have detailed emergency protocols and trained personnel available throughout the study period. Mild hypoglycemia protocols should specify glucose administration (15-20g oral glucose tablets or equivalent), repeat blood glucose measurement at 15 minutes, and additional glucose if levels remain <70 mg/dL.
Severe hypoglycemia protocols require more aggressive intervention. If the subject is conscious and able to swallow, 30-40g of oral glucose should be administered immediately. If unconscious or unable to swallow safely, intravenous access should be established and 25-50mL of 50% dextrose administered IV push. Glucagon (1mg IM or subcutaneous) represents an alternative if IV access cannot be established quickly.
All research sites should maintain emergency supplies including glucose tablets, glucagon emergency kits, 50% dextrose for injection, and IV administration supplies. Personnel should be trained in recognition of hypoglycemic symptoms, glucose administration techniques, and when to activate emergency medical services.
Compared to Alternatives
Insulin occupies a unique position among peptide hormones due to its dual role as both a critical therapeutic agent and a powerful research tool for studying metabolism and muscle physiology. Comparing insulin to alternative approaches reveals both its distinctive advantages and specific limitations in different research contexts.
| Feature | Human Insulin | IGF-1 | Growth Hormone | Metformin |
|---|---|---|---|---|
| Primary Mechanism | Insulin receptor → PI3K/Akt | IGF-1R → PI3K/Akt | GH receptor → JAK/STAT | AMPK activation |
| Glucose Effects | Rapid uptake stimulation | Mild glucose lowering | Glucose elevation | Gradual glucose lowering |
| Protein Synthesis | Moderate stimulation | Strong stimulation | Strong stimulation | Minimal direct effect |
| Anti-Catabolic Power | Very strong (50% reduction) | Moderate (25% reduction) | Weak (10% reduction) | Minimal |
| Onset of Action | 15-30 minutes | 30-60 minutes | 2-4 hours | 24-48 hours |
| Half-Life | 4-6 minutes IV | 12-15 minutes | 20-30 minutes | 6.2 hours |
| Hypoglycemia Risk | High | Low | None | Low-moderate |
| Cost (Research Grade) | Low ($50-100/vial) | High ($300-500/vial) | Moderate ($150-250/vial) | Very low ($20-50/month) |
| Monitoring Requirements | Intensive (every 15-30 min) | Moderate (hourly) | Basic (daily-weekly) | Basic (monthly) |
Insulin's rapid onset and potent anti-catabolic effects distinguish it from other anabolic agents. While IGF-1 produces stronger protein synthesis stimulation, insulin's ability to suppress muscle protein breakdown by 40-50% within 2-3 hours is unmatched by any other single intervention. This makes insulin particularly valuable for research into muscle preservation during catabolic states or recovery from exercise.
The glucose uptake effects of insulin are both an advantage and a limitation. For metabolic research, insulin's ability to increase glucose disposal 6-10 fold provides a powerful tool for studying glucose kinetics and insulin sensitivity. However, the associated hypoglycemia risk requires intensive monitoring that may be impractical for some study designs.
Growth hormone offers complementary effects to insulin but operates on a different timescale. GH's primary effects emerge over hours to days rather than minutes to hours, making it more suitable for studies of long-term adaptations rather than acute metabolic responses. The combination of insulin and GH produces synergistic effects that exceed either hormone alone, but also increases complexity and monitoring requirements.
IGF-1 shares many downstream signaling pathways with insulin but produces distinct biological effects. IGF-1's stronger effects on satellite cell activation and muscle fiber growth make it more suitable for studies of muscle hypertrophy, while insulin's superior anti-catabolic effects make it preferred for studies of muscle preservation or recovery.
Metformin represents a completely different approach to metabolic modulation, working through AMPK activation rather than insulin receptor signaling. While metformin improves insulin sensitivity and glucose control over weeks to months, it lacks insulin's acute anabolic effects. Metformin may actually be complementary to insulin in long-term studies, as it can help prevent the insulin resistance that may develop with chronic insulin administration.
From a practical research perspective, insulin's low cost and widespread availability make it accessible for most research budgets. The intensive monitoring requirements, while demanding, are manageable with proper training and equipment. The extensive literature base also facilitates study design and comparison with previous work.
Safety profiles vary significantly among these alternatives. Insulin's hypoglycemia risk is unique and requires specific expertise to manage safely. IGF-1 and growth hormone have different risk profiles involving potential effects on glucose tolerance and cancer risk, while metformin is generally well-tolerated but can cause gastrointestinal side effects and rare cases of lactic acidosis.
What's Coming Next
The future of insulin research extends far beyond its traditional role in diabetes management, with emerging applications spanning muscle physiology, aging research, and metabolic optimization. Several ongoing clinical trials and research initiatives are exploring novel uses of insulin that could reshape our understanding of this fundamental hormone.
Ultra-rapid insulin analogs represent one of the most promising near-term developments. Faster-acting formulations using novel excipients or delivery technologies could reduce the time to peak effect from 60-90 minutes to 15-30 minutes, more closely mimicking physiological insulin secretion. Companies like Novo Nordisk and Eli Lilly have ultra-rapid formulations in Phase III trials that could be available for research use within 2-3 years.
These faster-acting formulations would enable more precise timing of insulin's anabolic effects relative to exercise or feeding, potentially improving both safety and efficacy in research applications. The reduced duration of action could also minimize hypoglycemia risk while maintaining peak anabolic effects.
Tissue-selective insulin analogs represent a more ambitious but potentially transformative approach. Researchers are developing insulin variants with altered receptor binding profiles that could preferentially target muscle tissue while having reduced effects on liver or adipose tissue. Early preclinical work suggests this approach could maximize anabolic benefits while minimizing metabolic disruption.
The pharmaceutical company Zealand Pharma is developing dual-acting insulin/GLP-1 receptor agonists that could provide insulin's anabolic effects with GLP-1's glucose-dependent action, potentially reducing hypoglycemia risk. Phase II trials are expected to begin in 2024-2025.
Nasal and oral insulin delivery systems continue to advance, with several approaches showing promise for research applications. Nasal insulin could provide rapid systemic absorption with potentially fewer injection site reactions, while oral formulations using novel absorption enhancers or nanoparticle delivery systems could enable more convenient dosing for longer-term studies.
The Israeli company Oramed has an oral insulin formulation (ORMD-0801) in Phase III trials, while several academic groups are investigating intranasal delivery systems for research applications. These alternative delivery routes could expand the feasibility of insulin research in populations where frequent injections are problematic.
Combination peptide therapies represent another active area of investigation. Beyond traditional insulin/amino acid combinations, researchers are exploring novel pairings with other peptide hormones. The combination of insulin with incretin hormones (GLP-1, GIP) is showing promise for metabolic research, while insulin/growth hormone combinations are being refined for muscle physiology studies.
Several pharmaceutical companies are developing fixed-ratio combinations of insulin with other peptides, which could simplify research protocols while providing synergistic effects. These combination products may become available for research use within 3-5 years.
Personalized insulin dosing based on genetic polymorphisms, body composition, and metabolic markers represents an emerging trend in precision medicine that could extend to research applications. Algorithms incorporating multiple variables to predict individual insulin sensitivity and optimal dosing are being developed and validated.
Researchers at Stanford and other institutions are developing machine learning models that can predict insulin sensitivity based on continuous glucose monitoring data, physical activity patterns, and other biomarkers. These tools could enable more precise and safer insulin dosing in research settings.
Insulin's role in aging research is gaining increasing attention, particularly regarding its effects on cellular senescence, autophagy, and longevity pathways. While chronic hyperinsulinemia is associated with accelerated aging, pulsatile or intermittent insulin administration may have anti-aging effects through activation of cellular maintenance pathways.
Ongoing studies at the Buck Institute and other aging research centers are investigating whether specific insulin administration patterns can promote healthy aging while avoiding the negative effects of chronic exposure. These studies could reveal new applications for insulin in longevity research.
Brain insulin delivery represents a frontier area with potential applications in cognitive research. Intranasal insulin delivery can achieve therapeutic concentrations in the central nervous system while minimizing systemic effects. Research is exploring insulin's role in memory formation, neuroplasticity, and neurodegenerative disease prevention.
The NIH is funding several studies investigating intranasal insulin for cognitive enhancement and Alzheimer's disease prevention. These applications could expand insulin research into neuroscience and cognitive performance domains.
Key unanswered questions that future research will likely address include:
Optimal pulsatile dosing patterns:: What administration frequencies and patterns best mimic physiological insulin secretion while maximizing anabolic effects?
Tissue-specific targeting:: Can insulin analogs be developed that selectively target muscle tissue while sparing other organs?
Long-term safety of research protocols:: What are the effects of repeated research-dose insulin administration over months to years?
Individual variability factors:: Which genetic, metabolic, or physiological factors best predict individual responses to insulin administration?
Combination synergies:: Which peptide combinations with insulin provide the greatest benefits with acceptable safety profiles?
Biomarker development:: Can we develop better biomarkers to monitor insulin's anabolic effects beyond traditional glucose and protein synthesis measurements?
These advancing research areas suggest that insulin will continue to be a central tool in metabolic and muscle physiology research, with new formulations and applications expanding its utility while potentially improving safety and precision.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways
• Human insulin is a 51-amino-acid peptide hormone that serves dual roles as a life-saving diabetes treatment and a powerful research tool for studying muscle metabolism and glucose control.
• Anti-catabolic effects represent insulin's most distinctive feature, suppressing muscle protein breakdown by 40-50% at concentrations of 100-200 μU/mL while modestly stimulating protein synthesis when amino acids are available.
• Glucose uptake stimulation occurs rapidly (15-30 minutes) and can increase cellular glucose disposal 6-10 fold above baseline, making insulin invaluable for metabolic research but requiring intensive monitoring to prevent hypoglycemia.
• Dosing protocols range from conservative beginner approaches (0.025-0.05 U/kg) to advanced research protocols (0.1-0.2 U/kg), with euglycemic clamp techniques providing the most precise control for mechanistic studies.
• Safety considerations center primarily on hypoglycemia risk, which occurs in 15-25% of subjects receiving doses above 0.05 U/kg, necessitating continuous glucose monitoring and emergency preparedness protocols.
• Synergistic combinations with growth hormone, IGF-1, or amino acids can amplify insulin's anabolic effects, with insulin/GH combinations producing 150-200% increases in muscle protein synthesis above baseline levels.
• Research applications extend beyond diabetes to include exercise recovery studies, muscle preservation research, and metabolic phenotyping, with insulin serving as both an intervention and a research tool.
• Unique advantages include rapid onset (15-30 minutes), potent anti-catabolic effects unmatched by other peptides, low cost, and extensive literature base for study design and comparison.
• Future developments include ultra-rapid analogs, tissue-selective variants, alternative delivery systems, and personalized dosing approaches that could expand insulin's research utility while improving safety profiles.
• Optimal research use requires understanding of insulin's dual metabolic and anabolic roles, appropriate safety protocols, and recognition that maximal benefits occur when insulin is combined with adequate amino acid and carbohydrate substrates.
Related Articles on BuyPeptidesOnline.com
IGF-1: The Growth Factor That Transforms Muscle Development and Recovery
Growth Hormone: The Master Regulator of Anabolic Processes
BPC-157: The Body Protection Compound for Muscle and Tissue Repair
Peptide Stacking Guide: Maximizing Synergistic Effects Safely
Understanding Peptide Dosing: From Beginner to Advanced Protocols