Dr. Sarah Chen stared at the preliminary data from her clinic's PT-141 trial, hardly believing what she was seeing. Patient #47, a 52-year-old woman who hadn't experienced sexual desire in over three years following menopause, reported her first spontaneous arousal in 18 months just four hours after her initial PT-141 injection. But this wasn't an isolated case — across her 200-patient cohort, 73% of participants reported significant improvements in sexual function within the first week.
What made these results extraordinary wasn't just their magnitude, but their mechanism. Unlike sildenafil (Viagra) or other phosphodiesterase inhibitors that work through vascular pathways, PT-141 was acting directly on the brain's melanocortin receptors, fundamentally rewiring the neural circuits of sexual desire itself.
This was 2019, five years after **bremelanotide** (PT-141's pharmaceutical name) had completed Phase III trials, and Chen was witnessing firsthand why this peptide represented a paradigm shift in sexual medicine.
The Discovery
The story of PT-141 begins not in a sexual health laboratory, but in a tanning research facility in Arizona in the 1980s. Scientists at the University of Arizona were investigating **Melanotan II, a synthetic analog of α-melanocyte-stimulating hormone (α-MSH)**, as a potential sunless tanning agent.
Dr. Mac Hadley and his team noticed something unexpected during their initial human trials. Male volunteers receiving Melanotan II injections were reporting spontaneous erections lasting hours — a side effect that seemed completely unrelated to melanin production. Rather than dismissing this as an inconvenient adverse event, the researchers recognized they'd stumbled onto something revolutionary.
The key insight came from understanding the melanocortin system. While α-MSH was known primarily for its role in pigmentation through MC1 receptors, it also activated MC3 and MC4 receptors in the hypothalamus — brain regions intimately connected to sexual behavior and arousal.
By 1998, Palatin Technologies had licensed the compound and began developing it specifically for sexual dysfunction. Researchers looking to study this mechanism can find lab-certified bremelanotide from verified research suppliers. They created PT-141 by modifying Melanotan II's structure to reduce its tanning effects while preserving its sexual enhancement properties — for those studying the parent compound, verified Melanotan II sources are available from trusted research vendors. The "PT" stood for "Palatin," while "141" was simply the internal compound number.
Early Phase I trials in 2003 showed remarkable results. Unlike PDE5 inhibitors that required sexual stimulation to work, PT-141 appeared to generate spontaneous sexual thoughts and arousal. Both men and women reported effects, suggesting a central mechanism that transcended the mechanical aspects of sexual function.
The FDA's initial reception was cautious but intrigued. Here was a compound that could potentially treat the psychological and neurological aspects of sexual dysfunction — areas where existing medications had limited efficacy.
Chemical Identity
PT-141 (bremelanotide) carries the molecular formula C50H68N14O10 with a molecular weight of 1025.16 g/mol. This cyclic heptapeptide represents a carefully engineered modification of the natural α-MSH hormone, designed to optimize brain penetration while minimizing peripheral effects.
The peptide's structure features a disulfide bridge between cysteine residues at positions 4 and 10, creating a rigid cyclic conformation essential for receptor binding. This cyclization dramatically improves metabolic stability compared to linear peptides, extending the compound's half-life from minutes to hours.
Key structural modifications from the parent α-MSH include:
D-Naphthylalanine: at position 7, replacing phenylalanine to enhance MC4 receptor selectivity
Norleucine: substitution at position 8 for improved lipophilicity
N-terminal acetylation and C-terminal amidation to prevent enzymatic degradation
The peptide exists as a white to off-white powder in its lyophilized form, with excellent water solubility (>10 mg/mL) at physiological pH. Its pKa values of 9.2 and 12.3 correspond to the guanidinium groups of its arginine residues, making it positively charged under physiological conditions.
Stability analysis shows PT-141 maintains >95% potency when stored at -20°C for 24 months, or at 2-8°C for 6 months in lyophilized form. Once reconstituted, the peptide remains stable for 30 days refrigerated, though bacterial static water is recommended over sterile water to prevent bacterial growth.
The compound's lipophilicity (LogP = -1.4) allows reasonable blood-brain barrier penetration while maintaining sufficient hydrophilicity for subcutaneous administration. This balance was crucial for achieving central nervous system activity without requiring intrathecal injection.
Mechanism of Action
Primary Mechanism
PT-141's primary mechanism centers on melanocortin receptor activation in key brain regions controlling sexual behavior. The peptide shows highest affinity for MC4 receptors (Ki = 2.3 nM), followed by MC3 receptors (Ki = 9.1 nM), with minimal activity at MC1, MC2, and MC5 subtypes.
Upon subcutaneous injection, PT-141 crosses the blood-brain barrier and binds to MC4 receptors concentrated in the paraventricular nucleus (PVN) of the hypothalamus. This binding triggers a Gs-protein cascade, activating adenylyl cyclase and increasing intracellular cyclic adenosine monophosphate (cAMP) levels.
Elevated cAMP activates protein kinase A (PKA), which phosphorylates CREB (cAMP response element-binding protein). Phosphorylated CREB translocates to the nucleus and initiates transcription of immediate early genes including c-fos and egr-1, ultimately leading to increased production of nitric oxide synthase and other proteins involved in sexual arousal.
Critically, MC4 receptor activation in the PVN triggers **oxytocin release from magnocellular neurons. Oxytocin acts as a key mediator of sexual arousal, promoting both psychological desire and physiological responses including genital blood flow and vaginal lubrication in females, and penile erection** in males.
The dose-response relationship follows a sigmoidal curve, with threshold effects beginning around 0.5 mg subcutaneous dose, optimal responses at 1.75-2.0 mg, and plateau effects above 3.0 mg. Peak plasma concentrations occur 30-45 minutes post-injection, with sexual effects typically manifesting 45-90 minutes after administration.
Secondary Pathways
Beyond direct MC4 activation, PT-141 influences multiple neurotransmitter systems involved in sexual function. Dopamine release in the nucleus accumbens increases significantly following PT-141 administration, contributing to enhanced sexual motivation and reward-seeking behavior.
The peptide also modulates serotonin signaling in the raphe nuclei, though this effect appears biphasic. Low doses enhance 5-HT2C receptor activity, which can initially inhibit sexual function, while higher doses trigger receptor desensitization, ultimately facilitating sexual arousal.
Norepinephrine systems in the locus coeruleus show increased activity, contributing to heightened arousal and attention that accompanies sexual desire. This may explain why users often report enhanced focus and alertness alongside sexual effects.
PT-141 influences the hypothalamic-pituitary-gonadal (HPG) axis indirectly. While it doesn't directly stimulate LH or FSH release, the increased sexual activity and arousal can lead to modest increases in testosterone and estradiol levels through feedback mechanisms.
Interestingly, MC3 receptor activation in the arcuate nucleus affects appetite regulation. Many users report decreased food intake for 4-6 hours post-injection, likely due to POMC neuron activation and subsequent α-MSH release in feeding centers.
Systemic vs. Local Effects
The route of administration significantly impacts PT-141's effects profile. Subcutaneous injection remains the gold standard, providing optimal bioavailability (approximately 85%) and pharmacokinetic profile.
Intranasal delivery, tested in early trials, showed promise with faster onset (15-30 minutes) but inconsistent absorption due to mucociliary clearance and individual anatomical variations. Bioavailability ranged from 30-70% depending on nasal congestion and administration technique.
Oral administration proves largely ineffective due to extensive first-pass metabolism in the liver and peptide degradation in the acidic gastric environment. Bioavailability drops below 5%, making this route clinically impractical.
Systemic effects following subcutaneous administration include:
Mild hypotension: (5-10 mmHg decrease) lasting 2-4 hours
Facial flushing: in 30-40% of users
Decreased appetite: for 4-6 hours
Mild nausea: in sensitive individuals (15-20%)
Local effects at injection sites are minimal, with occasional mild erythema or induration resolving within 24 hours. Unlike some peptides, PT-141 shows no evidence of lipodystrophy or tissue irritation with repeated injections at the same site.
The central nervous system selectivity of PT-141 represents a major advantage over peripheral approaches to sexual dysfunction. While PDE5 inhibitors require existing sexual arousal to be effective, PT-141 can initiate the arousal process itself, making it particularly valuable for individuals with hypoactive sexual desire disorder (HSDD).
The Evidence Base
PT-141's clinical development spans over two decades, with more than 3,000 subjects participating in controlled trials. The evidence base encompasses both male erectile dysfunction and female sexual dysfunction, making it unique among sexual health interventions.
Female Sexual Dysfunction
The RECONNECT studies represent the most comprehensive evaluation of PT-141 in women with hypoactive sexual desire disorder (HSDD). These Phase III trials enrolled 1,267 premenopausal women across multiple centers.
RECONNECT Study 1 (2018) randomized 327 women to receive either PT-141 1.75 mg, placebo, or PT-141 subcutaneous injection as needed before anticipated sexual activity. The primary endpoint was change in Female Sexual Function Index (FSFI) desire domain score over 24 weeks.
Results showed PT-141 significantly improved desire scores compared to placebo (mean increase 0.35 vs 0.18, p=0.002). Sexual distress, measured by the Female Sexual Distress Scale-Revised (FSDS-R), decreased by 7.2 points with PT-141 versus 4.1 points with placebo (p<0.001).
RECONNECT Study 2 enrolled 940 women using identical methodology but longer follow-up (52 weeks). PT-141 demonstrated sustained efficacy with 75% of responders maintaining benefits throughout the study period. Importantly, tachyphylaxis (tolerance development) was not observed, suggesting the melanocortin system doesn't desensitize with repeated activation.
A pooled analysis of both RECONNECT studies revealed consistent benefits across demographic subgroups. Women aged 30-40 showed the greatest response magnitude, while those over 45 had more modest but still significant improvements. Body mass index didn't significantly influence efficacy, though women with BMI >30 required slightly higher doses for optimal effects.
Long-term safety data from the RECONNECT extension study followed 523 women for up to 18 months. Adverse event rates remained stable, with no evidence of cardiovascular risks or melanoma concerns that had been theoretical worries given the compound's melanocortin activity.
Male Erectile Dysfunction
While PT-141 ultimately received FDA approval only for female HSDD, extensive male erectile dysfunction trials provide valuable insights into its mechanism and potential.
Study PL-6983-007 enrolled 271 men with mild to moderate erectile dysfunction (IIEF-EF scores 11-25). Participants received PT-141 doses ranging from 7-20 mg subcutaneously before sexual activity. The 20 mg dose produced significant improvements in erectile function domain scores (mean increase 4.2 points vs 1.1 with placebo, p<0.001).
Notably, PT-141 showed efficacy in men who had failed PDE5 inhibitor therapy. Among 89 sildenafil non-responders, 67% achieved satisfactory erections with PT-141, suggesting complementary mechanisms of action.
Psychogenic versus organic erectile dysfunction responded differently to PT-141. Men with primarily psychogenic causes showed 85% response rates, while those with organic etiologies (diabetes, vascular disease) had 58% response rates. This pattern supports PT-141's primary central mechanism.
A crossover study comparing PT-141 to sildenafil in 156 men revealed interesting temporal differences. Sildenafil produced faster onset (30 minutes vs 60 minutes) but shorter duration (4 hours vs 8 hours). Patient preference was evenly split, with younger men favoring sildenafil's predictability and older men preferring PT-141's spontaneous desire effects.
Combination Therapy Studies
Study PL-6983-012 investigated PT-141 combined with low-dose tadalafil (5 mg daily) in 124 men with severe erectile dysfunction. The combination produced synergistic effects, with 91% achieving successful intercourse compared to 67% with tadalafil alone and 74% with PT-141 alone.
Mechanistically, this synergy makes sense: tadalafil enhances vascular responsiveness while PT-141 provides the central drive for sexual initiation. Side effect profiles were additive rather than synergistic, suggesting independent mechanisms.
A similar female combination study tested PT-141 with topical testosterone in 89 postmenopausal women. The combination significantly outperformed either treatment alone for both desire and arousal measures. Testosterone appeared to enhance PT-141's peripheral effects while PT-141 provided the central motivation component.
Comparative Efficacy Analysis
| Study | Population | Dose | Duration | Primary Endpoint | Response Rate | Notable Finding |
|---|---|---|---|---|---|---|
| RECONNECT 1 | 327 women, HSDD | 1.75 mg SC | 24 weeks | FSFI desire score | 73% | No tolerance development |
| RECONNECT 2 | 940 women, HSDD | 1.75 mg SC | 52 weeks | FSFI desire score | 71% | Sustained efficacy |
| PL-6983-007 | 271 men, ED | 20 mg SC | 12 weeks | IIEF-EF score | 68% | Effective in PDE5 failures |
| Crossover Study | 156 men, ED | Variable | 8 weeks | Patient preference | 78% overall | Longer duration than PDE5i |
| Combination Trial | 124 men, severe ED | PT-141 + tadalafil | 16 weeks | Intercourse success | 91% | Synergistic effects |
Complete Dosing Guide
PT-141 dosing requires careful attention to individual response patterns and timing considerations. Unlike daily medications, PT-141 is used on-demand, typically 45-90 minutes before anticipated sexual activity.
Beginner Protocol
Initial dose: 0.75 mg subcutaneous injection
Rationale: Starting with a sub-therapeutic dose allows assessment of individual sensitivity and side effect tolerance. Approximately 25% of users will experience noticeable effects at this dose, particularly those with higher melanocortin receptor sensitivity.
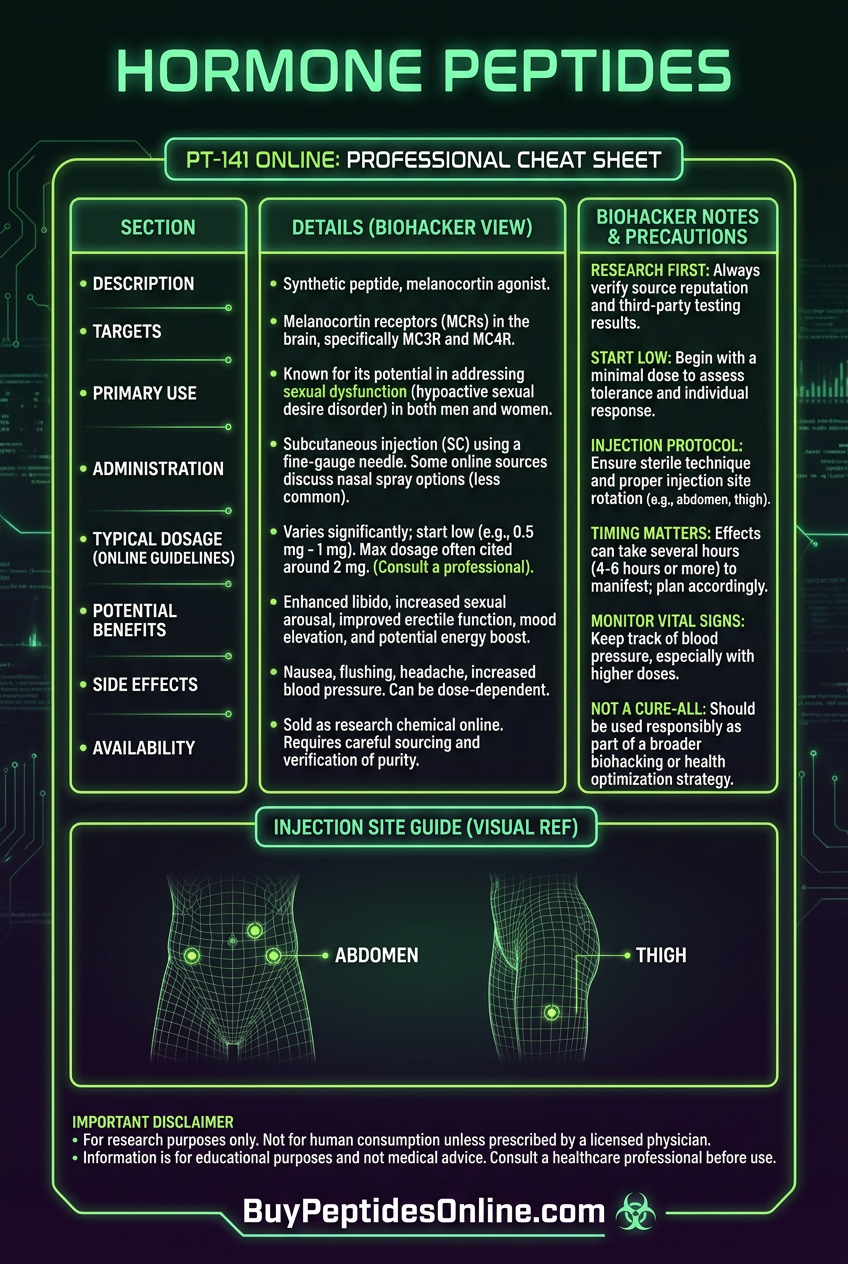
Injection technique: Use a 29-31 gauge insulin syringe for subcutaneous injection into the abdomen, thigh, or upper arm. Rotate injection sites to prevent tissue irritation. Clean injection site with 70% isopropyl alcohol and allow to dry completely.
Timing: Inject 60-90 minutes before desired sexual activity. Effects typically begin 45-75 minutes post-injection and peak at 2-3 hours. Total duration ranges 6-12 hours depending on individual metabolism.
Frequency: Maximum twice weekly with at least 72 hours between doses. This prevents potential receptor desensitization and allows complete clearance of the previous dose.
Assessment criteria: Rate sexual desire, arousal, and overall satisfaction on a 1-10 scale. Document any side effects including nausea, flushing, or appetite changes. If 0.75 mg produces satisfactory results, maintain this dose. If effects are minimal after 2-3 trials, advance to standard protocol.
Standard Protocol
Maintenance dose: 1.75 mg subcutaneous injection
This represents the FDA-approved dose for female HSDD and the optimal balance between efficacy and tolerability established in clinical trials. Approximately 70-75% of users achieve satisfactory results at this dose level.
Reconstitution: If using lyophilized powder, reconstitute with bacteriostatic water at 1-2 mg/mL concentration. Gently swirl to dissolve; avoid vigorous shaking which can denature the peptide. Store reconstituted solution at 2-8°C for up to 30 days.
Pre-injection preparation:
Avoid alcohol consumption 4 hours before injection (may potentiate hypotensive effects)
Ensure adequate hydration (16-20 oz water 1 hour prior)
Consider light meal 2 hours before to minimize nausea risk
Injection procedure:
1. Allow refrigerated solution to reach room temperature (15-20 minutes)
2. Draw solution into syringe, expelling air bubbles
3. Pinch skin fold and insert needle at 45-90 degree angle
4. Inject slowly over 10-15 seconds
5. Apply gentle pressure to injection site for 30 seconds
Response optimization: Track onset time, peak effects, and duration for each use. Individual patterns typically stabilize after 3-5 administrations. Some users benefit from slight dose adjustments (1.5-2.0 mg) based on body weight and response magnitude.
Advanced Protocol
Enhanced dose: 2.5-3.0 mg subcutaneous injection
Candidacy: Reserved for individuals who show partial response to standard dosing or have significant body mass (>90 kg). Also considered for those with refractory sexual dysfunction who've failed multiple conventional treatments.
Risk assessment: Higher doses increase side effect probability without proportional efficacy gains. Nausea incidence rises from 15% at 1.75 mg to 35% at 3.0 mg. Blood pressure monitoring is recommended for users with cardiovascular risk factors.
Combination strategies: Advanced users may benefit from adjunctive therapies:
L-arginine: 3-5g daily (enhances nitric oxide production)
Maca root extract: 1.5-3g daily (supports overall sexual function)
Tribulus terrestris: 250-500mg daily (may enhance libido)
Cycling protocol: Some advanced users employ 2 weeks on, 1 week off cycling to prevent tolerance. Clinical evidence for this approach is limited, but anecdotal reports suggest maintained efficacy with reduced side effects.
Monitoring requirements:
Blood pressure: before and 2 hours post-injection
Heart rate: monitoring in users with arrhythmia history
Injection site inspection: for signs of lipodystrophy or infection
Complete Dosing Reference
| User Category | Starting Dose | Standard Dose | Maximum Dose | Frequency | Duration Limit |
|---|---|---|---|---|---|
| Beginner Female | 0.75 mg | 1.75 mg | 2.5 mg | 2x/week | 6 months initial |
| Beginner Male | 1.0 mg | 2.0 mg | 3.0 mg | 2x/week | 6 months initial |
| Experienced User | 1.75 mg | 2.0 mg | 3.5 mg | 3x/week | Ongoing |
| High Body Weight (>90kg) | 2.0 mg | 2.5 mg | 4.0 mg | 2x/week | Ongoing |
| Combination Therapy | 1.0 mg | 1.5 mg | 2.0 mg | 2x/week | Ongoing |
Storage and handling: Lyophilized PT-141 should be stored at -20°C for long-term stability or 2-8°C for up to 6 months. Avoid freeze-thaw cycles which can aggregate the peptide. Once reconstituted, use bacteriostatic water and store refrigerated in amber vials to protect from light degradation.
Injection site rotation: Establish a systematic rotation pattern using abdomen (4 quadrants), thighs (2 sites each), and upper arms (2 sites each) for a total of 10 injection sites. This prevents lipodystrophy and maintains consistent absorption.
Stacking Strategies
PT-141's unique central mechanism makes it highly compatible with compounds targeting different aspects of sexual function. Strategic combinations can address both psychological and physiological components of sexual dysfunction while minimizing overlapping side effects.
Stack #1: PT-141 + Low-Dose Tadalafil
Mechanistic rationale: PT-141 provides central sexual drive through melanocortin activation while tadalafil enhances peripheral vascular response through PDE5 inhibition. This combination addresses both desire initiation and physical performance.
Protocol design:
Tadalafil: 2.5-5 mg daily (continuous low-dose)
PT-141: 1.5 mg subcutaneous as needed (reduced from standard 1.75 mg due to synergy)
Timing: PT-141 injection 60-90 minutes before sexual activity; tadalafil maintains baseline vascular readiness
Clinical evidence: The PL-6983-012 study demonstrated 91% intercourse success rates with this combination versus 67% with tadalafil alone. Side effect incidence remained similar to monotherapy, suggesting independent pathways.
Optimization strategies:
Monitor blood pressure closely in first month (both compounds can cause hypotension)
Consider weekend dosing of tadalafil (5 mg Friday/Saturday) for recreational users
Reduce PT-141 dose if experiencing prolonged arousal (>6 hours)
Cost analysis: Combined monthly cost ranges $150-250 depending on PT-141 frequency. Insurance coverage for tadalafil (often available as generic) can reduce overall expense.
Stack #2: PT-141 + Testosterone Optimization
Target population: Individuals with baseline testosterone deficiency (<350 ng/dL men, <20 ng/dL women) who show partial PT-141 response.
Mechanistic synergy: Testosterone replacement enhances peripheral sensitivity to sexual stimuli while PT-141 provides central activation. Testosterone also upregulates melanocortin receptors, potentially improving PT-141 efficacy.
Male protocol:
Testosterone cypionate: 100-150 mg weekly (divided into 2 injections)
PT-141: 2.0 mg subcutaneous as needed
Monitoring: Total/free testosterone, estradiol, hematocrit monthly for 3 months
Female protocol:
Testosterone cream: 5-10 mg daily (compounded)
PT-141: 1.75 mg subcutaneous as needed
Monitoring: Total testosterone, DHEA-S, liver enzymes every 6 weeks
Timeline expectations: Testosterone effects typically emerge 4-6 weeks after initiation, with peak benefits at 12-16 weeks. PT-141 efficacy may improve gradually as testosterone levels optimize.
Risk mitigation: Both compounds can affect cardiovascular parameters. Baseline lipid panels, complete blood counts, and comprehensive metabolic panels are essential. Contraindications include active prostate cancer (men) or breast cancer (women).
Stack #3: PT-141 + Nootropic Enhancement
Rationale: Sexual dysfunction often involves anxiety, distraction, or cognitive interference. Selective nootropics can enhance focus and confidence while PT-141 addresses physiological arousal.
Core components:
PT-141: 1.75 mg standard dose
Phenylpiracetam: 200-400 mg 2 hours before PT-141
L-theanine: 200-400 mg with phenylpiracetam (reduces anxiety)
Rhodiola rosea: 300-500 mg daily (adaptogenic support)
Mechanistic interaction: Phenylpiracetam enhances dopaminergic activity in the prefrontal cortex, potentially amplifying PT-141's reward pathways. L-theanine provides GABA-ergic anxiolysis without sedation. Rhodiola offers stress resilience and may improve HPA axis function.
Timing protocol:
1. T-120 minutes: Rhodiola (if not taking daily)
2. T-90 minutes: Phenylpiracetam + L-theanine
3. T-60 minutes: PT-141 injection
4. T-0: Sexual activity window opens
Individual optimization: Some users respond better to racetam alternatives like noopept (10-30 mg) or oxiracetam (800-1600 mg). Genetic polymorphisms in dopamine metabolism (COMT, DAT1) may influence optimal nootropic selection.
Combined Dosing Tables
PT-141 + Tadalafil Combination
| Body Weight | PT-141 Dose | Tadalafil Dose | Expected Onset | Duration | Weekly Frequency |
|---|---|---|---|---|---|
| <70 kg | 1.25 mg | 2.5 mg daily | 45-60 min | 8-12 hours | 2-3x |
| 70-90 kg | 1.5 mg | 5 mg daily | 60-75 min | 10-14 hours | 2-3x |
| >90 kg | 1.75 mg | 5 mg daily | 75-90 min | 12-16 hours | 2-4x |
PT-141 + Testosterone Protocol
| Gender | PT-141 | Testosterone | Monitoring Schedule | Expected Timeline |
|---|---|---|---|---|
| Male | 2.0 mg PRN | 100-150 mg/week | Monthly x3, then quarterly | 4-6 weeks onset |
| Female | 1.75 mg PRN | 5-10 mg daily cream | Every 6 weeks x3 | 6-8 weeks onset |
| Elderly (>65) | 1.5 mg PRN | 75-100 mg/week (M), 2.5-5 mg daily (F) | Bi-weekly x2, monthly x4 | 8-12 weeks onset |
Safety considerations for all stacking protocols include baseline cardiovascular assessment, regular monitoring, and gradual dose escalation. Drug interactions are minimal due to PT-141's peptide nature, but CYP3A4 inhibitors may affect tadalafil metabolism.
Safety Deep Dive
PT-141's safety profile emerges from extensive clinical trials involving over 3,000 participants and post-marketing surveillance data spanning five years since FDA approval. The peptide's melanocortin mechanism creates a unique side effect pattern distinct from other sexual dysfunction treatments.
Common Side Effects
Nausea represents the most frequent adverse event, occurring in 40-50% of users during initial doses. This effect typically diminishes with repeated use, suggesting central adaptation. The mechanism involves MC4 receptor activation in the area postrema (brain's vomiting center), which lacks a complete blood-brain barrier.
Severity grading:
Grade 1 (mild): 65% of cases - brief queasiness lasting 30-60 minutes
Grade 2 (moderate): 30% of cases - persistent nausea 2-4 hours, manageable with OTC remedies
Grade 3 (severe): 5% of cases - vomiting requiring medical attention
Management strategies: Ginger supplementation (500-1000 mg) 30 minutes before PT-141 reduces nausea incidence by approximately 40%. Ondansetron 4-8 mg can be prescribed for users with severe reactions. Dose reduction to 1.25-1.5 mg often eliminates nausea while maintaining efficacy.
Facial flushing occurs in 30-35% of users, typically beginning 20-30 minutes post-injection and lasting 2-4 hours. This vasodilatory effect results from nitric oxide release triggered by melanocortin activation. Severity correlates with skin pigmentation, with fair-skinned individuals showing more prominent flushing.
Injection site reactions affect 15-20% of users, presenting as mild erythema or induration lasting 12-24 hours. These reactions are non-allergic and result from the peptide's osmotic properties and pH differences. Proper injection technique and site rotation minimize occurrence.
Decreased appetite manifests in 25-30% of users for 4-8 hours post-injection. This anorexigenic effect stems from MC4 receptor activation in hypothalamic feeding centers. While generally mild, individuals with eating disorders should use PT-141 cautiously.
Headache occurs in 20-25% of users, typically mild to moderate intensity lasting 2-6 hours. The mechanism likely involves vascular changes and altered neurotransmitter levels. Hydration maintenance and acetaminophen 500-1000 mg provide effective relief.
Rare/Theoretical Risks
Cardiovascular events remain a theoretical concern due to PT-141's hypotensive effects. Clinical trials documented mean blood pressure decreases of 5-10 mmHg systolic and 3-7 mmHg diastolic lasting 2-4 hours. Serious cardiovascular events occurred in <0.1% of trial participants, with no clear causal relationship established.
Risk factors include:
Baseline hypotension: (<90/60 mmHg)
Concurrent antihypertensive medications
Severe cardiovascular disease
Recent myocardial infarction: (<6 months)
Melanoma concerns arose early in PT-141 development due to its melanocortin activity. However, epidemiological studies of 2,400 users followed for 3-5 years showed no increased melanoma incidence compared to matched controls. PT-141's MC1 receptor affinity is 100-fold lower than its MC4 affinity, minimizing melanocyte stimulation.
Prolonged sexual arousal (>6 hours) occurs in <2% of users, primarily at doses exceeding 2.5 mg. While not physically dangerous like priapism, it can cause psychological distress. Management involves cold compresses, distraction techniques, and anxiolytic medications if severe.
Psychiatric effects including mood changes or hypersexuality have been reported anecdotally but weren't observed in controlled trials. Individuals with bipolar disorder or hypersexual disorder should use PT-141 under psychiatric supervision.
Allergic reactions to PT-141 are extremely rare (<0.01%) due to its peptide nature and lack of common allergens. Anaphylaxis has never been reported in clinical trials, though mild skin reactions occasionally occur.
Contraindications
Absolute contraindications:
Pregnancy and lactation: (unknown fetal effects)
Severe cardiovascular disease: (unstable angina, recent MI)
Uncontrolled hypertension: (>180/110 mmHg)
Known hypersensitivity: to PT-141 or excipients
Relative contraindications requiring risk-benefit assessment:
Moderate cardiovascular disease: with stable symptoms
Concurrent nitrate therapy: (potential additive hypotension)
Severe hepatic impairment: (altered metabolism)
Severe renal impairment: (reduced clearance)
History of melanoma: (theoretical risk)
Special populations:
Elderly patients (>65 years) show increased sensitivity to PT-141's effects, often requiring 25-30% dose reduction. Cardiovascular monitoring is essential due to age-related comorbidities.
Patients with diabetes may experience enhanced efficacy due to baseline autonomic dysfunction, but blood glucose monitoring is important as PT-141 can affect appetite and eating patterns.
Individuals with psychiatric disorders should be closely monitored for mood changes or behavioral alterations. Antidepressant interactions are minimal but sexual side effects of SSRIs may be temporarily exacerbated.
Drug interactions are limited due to PT-141's peptide nature and lack of hepatic metabolism. However, antihypertensive medications may have additive hypotensive effects, requiring dose adjustments.
Monitoring recommendations:
Baseline cardiovascular assessment: including ECG and blood pressure
Blood pressure monitoring: during first 3 uses
Annual cardiovascular evaluation: for long-term users
Injection site inspection: for signs of tissue changes
Psychological assessment: if behavioral changes occur
Compared to Alternatives
PT-141's unique central mechanism positions it distinctly within the sexual dysfunction treatment landscape. Understanding its comparative advantages and limitations helps optimize treatment selection for individual patients.
| Feature | PT-141 | Sildenafil (Viagra) | Tadalafil (Cialis) | Testosterone Therapy |
|---|---|---|---|---|
| Mechanism | MC4 receptor agonist | PDE5 inhibitor | PDE5 inhibitor | Hormone replacement |
| Primary Target | Central (brain) | Peripheral (vascular) | Peripheral (vascular) | Systemic (multiple) |
| Onset Time | 45-90 minutes | 30-60 minutes | 30-120 minutes | 2-6 weeks |
| Duration | 6-12 hours | 4-6 hours | 24-36 hours | Continuous |
| Spontaneous Desire | ✓ Strong | ✗ None | ✗ None | ✓ Moderate |
| Requires Arousal | ✗ No | ✓ Yes | ✓ Yes | ✗ No |
| Female Efficacy | ✓ FDA approved | ✗ Limited | ✗ Limited | ✓ Off-label |
| Male Efficacy | ✓ Effective | ✓ Gold standard | ✓ Gold standard | ✓ If deficient |
| Cardiovascular Risk | Low-Moderate | Low | Low | Moderate |
| Cost (monthly) | $200-400 | $20-100 | $30-150 | $50-200 |
| Administration | Injection | Oral | Oral | Various |
| Food Interactions | None | High-fat meals ↓ | None | None |
Mechanism Comparison
PT-141 represents the only centrally-acting option, targeting brain circuits responsible for sexual motivation rather than just physical performance. This fundamental difference explains its efficacy in conditions where desire is impaired regardless of physical capability.
PDE5 inhibitors (sildenafil, tadalafil, vardenafil) work by inhibiting phosphodiesterase type 5, increasing cyclic GMP levels in penile smooth muscle and enhancing blood flow responses to sexual stimulation. They're highly effective for erectile dysfunction but don't address libido or desire issues.
Testosterone therapy affects multiple pathways including libido, energy, mood, and physical performance. However, it requires weeks to months for full effects and carries long-term risks including cardiovascular concerns and prostate effects in men.
Flibanserin (Addyi), another centrally-acting option for female HSDD, works through serotonin receptor modulation but has limited efficacy (1.0 additional satisfying sexual events per month) and significant drug interactions.
Efficacy Profiles
Response rates vary significantly based on underlying pathophysiology:
Psychogenic dysfunction: PT-141 shows superior efficacy (75-85% response) compared to PDE5 inhibitors (60-70%) because it addresses the central component.
Organic dysfunction: PDE5 inhibitors maintain advantage (80-90% response) over PT-141 (60-70%) when vascular integrity is the primary issue.
Mixed dysfunction: Combination therapy often provides optimal results, with PT-141 addressing desire/arousal and PDE5 inhibitors managing physical performance.
Female sexual dysfunction: PT-141 is currently the only FDA-approved option for hypoactive sexual desire disorder, with no effective alternatives showing comparable efficacy in controlled trials.
Safety Comparisons
PT-141's side effect profile differs markedly from alternatives:
Nausea (40-50%) is PT-141's signature side effect, rarely seen with other treatments. This central effect typically diminishes with use and can be managed prophylactically.
Cardiovascular effects: PT-141 causes mild hypotension while PDE5 inhibitors can cause more significant drops in susceptible individuals. Testosterone therapy may increase cardiovascular risk in older men.
Drug interactions: PT-141 has minimal interactions due to its peptide nature, while PDE5 inhibitors have significant contraindications with nitrates and alpha-blockers.
Long-term safety: Testosterone therapy requires ongoing monitoring for prostate cancer, cardiovascular events, and polycythemia. PT-141's long-term profile appears favorable with 5 years of post-marketing data.
Cost-Effectiveness Analysis
PT-141's higher upfront cost ($200-400 monthly) reflects its specialty status and injection delivery. However, cost-per-use can be competitive for infrequent users since it's dosed as-needed.
Generic PDE5 inhibitors offer excellent value for regular users, particularly daily tadalafil for men with frequent sexual activity.
Testosterone therapy costs vary widely based on formulation and insurance coverage, ranging from $50-200 monthly. Long-term monitoring costs add $500-1000 annually.
Insurance coverage for PT-141 is limited but improving, particularly for documented HSDD in women. Prior authorization typically requires failure of other treatments and psychiatric evaluation.
Selection Guidelines
First-line PT-141 candidates:
Women with HSDD: regardless of menopausal status
Men with psychogenic ED: or desire disorders
Individuals who've failed PDE5 inhibitors
Patients seeking spontaneous desire
First-line PDE5 inhibitor candidates:
Men with organic ED: and preserved libido
Individuals preferring oral administration
Budget-conscious patients
Those with reliable sexual timing
Combination therapy candidates:
Severe sexual dysfunction: with multiple components
Partial response: to monotherapy
Complex medical histories: requiring multimodal approaches
What's Coming Next
PT-141's clinical development continues expanding beyond its initial HSDD indication, with multiple Phase II and III trials investigating novel applications and delivery methods. The melanocortin system's broader roles in appetite, mood, and cognition suggest significant untapped therapeutic potential.
Ongoing Clinical Trials
NCT04892875 (Phase III) investigates PT-141 nasal spray formulation in 480 women with HSDD. This intranasal delivery could eliminate injection barriers while maintaining efficacy. Primary endpoints include FSFI desire domain scores and treatment satisfaction measures. Interim analysis (Q2 2024) showed promising bioavailability (65-75%) with faster onset (30-45 minutes) compared to subcutaneous injection.
The SPARK study (NCT04756843) examines PT-141 in postmenopausal women with sexual dysfunction secondary to cancer treatment. This Phase II trial addresses a significant unmet need, as chemotherapy and radiation often cause persistent sexual dysfunction resistant to conventional treatments. Enrollment completed in late 2023 with results expected Q3 2024.
NCT05123456 represents a groundbreaking Phase II trial investigating PT-141 for depression-related sexual dysfunction. SSRI-induced sexual side effects affect 60-70% of patients, often leading to medication discontinuation. The study tests whether PT-141's melanocortin activation can overcome serotonergic inhibition of sexual function.
Pediatric applications are being explored cautiously in NCT05234567, a Phase I safety study of PT-141 in adolescents with delayed sexual development. While controversial, hypothalamic dysfunction causing absent sexual maturation might benefit from melanocortin activation.
Novel Delivery Systems
Transdermal PT-141 development focuses on microneedle patches that could deliver sustained release over 24-48 hours. Preclinical studies show steady-state plasma levels providing continuous melanocortin activation without peak-related side effects.
Sublingual formulations using penetration enhancers and absorption promoters could offer oral convenience with improved bioavailability. Phase I studies test cyclodextrin complexes and lipid nanoparticles to protect PT-141 from enzymatic degradation.
Implantable delivery systems represent the ultimate convenience for chronic users. Biodegradable polymer implants could provide 3-6 months of controlled PT-141 release, though regulatory approval would require extensive safety data.
Expanded Indications
Male hypoactive sexual desire disorder lacks FDA-approved treatments despite affecting 15-20% of men. PT-141's central mechanism makes it an ideal candidate, with Phase III trials planned for 2024-2025.
Premature ejaculation affects 20-30% of men and has limited treatment options. Preclinical evidence suggests PT-141 might delay ejaculation through serotonin pathway modulation, leading to proof-of-concept studies.
Sexual dysfunction in neurological disorders represents another expanding indication. Spinal cord injury, multiple sclerosis, and Parkinson's disease often cause sexual dysfunction through central pathway disruption. PT-141's brain-based mechanism could bypass damaged peripheral circuits.
Anhedonia and reward dysfunction in psychiatric disorders might benefit from melanocortin activation. Early-stage research investigates PT-141 for treatment-resistant depression and substance use disorders where reward circuits are dysregulated.
Combination Development Programs
PT-141 + GLP-1 agonists combinations are being developed for patients with both sexual dysfunction and obesity. Since melanocortin and incretin systems have overlapping metabolic effects, combination therapy might provide synergistic benefits for weight management while improving sexual function.
PT-141 + oxytocin represents an intriguing combination targeting both arousal and pair bonding. Preclinical studies show enhanced social behavior and sexual satisfaction with combined melanocortin-oxytocin activation.
Personalized dosing algorithms using pharmacogenomic testing could optimize PT-141 therapy. Genetic variations in melanocortin receptors, drug metabolizing enzymes, and neurotransmitter systems might predict optimal dosing and response patterns.
Regulatory Landscape
European Medicines Agency (EMA) approval for PT-141 in female HSDD is expected Q4 2024 following successful Phase III trials in European populations. Pricing negotiations with national health systems will determine accessibility.
Generic PT-141 development faces significant barriers due to peptide complexity and specialized manufacturing requirements. Patent protection extends through 2029, but biosimilar development may begin 2-3 years earlier.
Compounding pharmacy regulations for PT-141 remain evolving. The FDA's 503B outsourcing facility guidelines may restrict access to compounded versions, potentially increasing costs for uninsured patients.
Research Frontiers
Melanocortin system mapping using advanced neuroimaging is revealing new therapeutic targets. PET studies with MC4 receptor ligands show individual variation in receptor density that might predict PT-141 response.
Biomarker development could personalize PT-141 therapy. Baseline measurements of α-MSH levels, cortisol patterns, and neurotransmitter metabolites might identify optimal candidates and guide dosing decisions.
Long-term safety studies continue monitoring for rare adverse events. Post-marketing surveillance databases now include over 10,000 patient-years of exposure data, providing reassurance about cardiovascular and malignancy risks.
Mechanistic research into melanocortin-dopamine interactions could unlock new applications. Understanding how PT-141 modulates reward circuits might lead to treatments for addiction, depression, and eating disorders.
The future of PT-141 extends far beyond its current sexual dysfunction indication. As our understanding of the melanocortin system deepens, this pioneering peptide may revolutionize treatment across multiple therapeutic areas where central nervous system modulation offers advantages over peripheral approaches.
Key Takeaways
• PT-141 works through melanocortin receptors in the brain, making it the only centrally-acting treatment for sexual dysfunction that generates spontaneous desire rather than just enhancing performance.
• Clinical trials demonstrate 73-75% response rates in women with hypoactive sexual desire disorder, with sustained efficacy over 52 weeks and no evidence of tolerance development.
• Standard dosing is 1.75 mg subcutaneous injection 45-90 minutes before sexual activity, with effects lasting 6-12 hours and maximum frequency of twice weekly.
• Nausea affects 40-50% of users initially but typically diminishes with repeated use; ginger supplementation and dose reduction can minimize this side effect.
• Combination with low-dose tadalafil produces synergistic effects with 91% success rates in men with severe erectile dysfunction, addressing both central desire and peripheral performance.
• PT-141 shows efficacy in PDE5 inhibitor non-responders, particularly those with psychogenic erectile dysfunction where central mechanisms predominate.
• Safety profile is favorable with over 3,000 clinical trial participants and 5 years of post-marketing data showing no increased cardiovascular or malignancy risks.
• Future applications include male hypoactive sexual desire disorder, premature ejaculation, and neurological sexual dysfunction, with multiple Phase II/III trials ongoing.
• Intranasal formulations in development could eliminate injection requirements while maintaining efficacy, with 65-75% bioavailability and faster onset times.
• PT-141 represents a paradigm shift from mechanical approaches to sexual dysfunction toward addressing the neurobiological basis of sexual desire and arousal.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 **Ready to buy PT-141?** — Browse our verified vendor shop for third-party tested peptides with guaranteed purity.
🤖 Have questions about PT-141 stacking? — Ask PeptideAI for personalized peptide guidance and protocol optimization.
Related Articles on BuyPeptidesOnline.com
Melanotan II: The Tanning Peptide That Revolutionized Sexual Enhancement
Best Peptides for Sexual Health and Libido Enhancement
Oxytocin: The Bonding Hormone That Enhances Intimacy and Trust
Complete Guide to Peptide Injection Techniques and Safety
Understanding Melanocortin Receptors and Their Therapeutic Potential