The Achilles tendon snapped with an audible pop during the championship match. For Dr. Sarah Chen, watching her patient—a 28-year-old professional basketball player—crumple to the court, the injury represented more than just torn collagen fibers. It was a career in jeopardy.
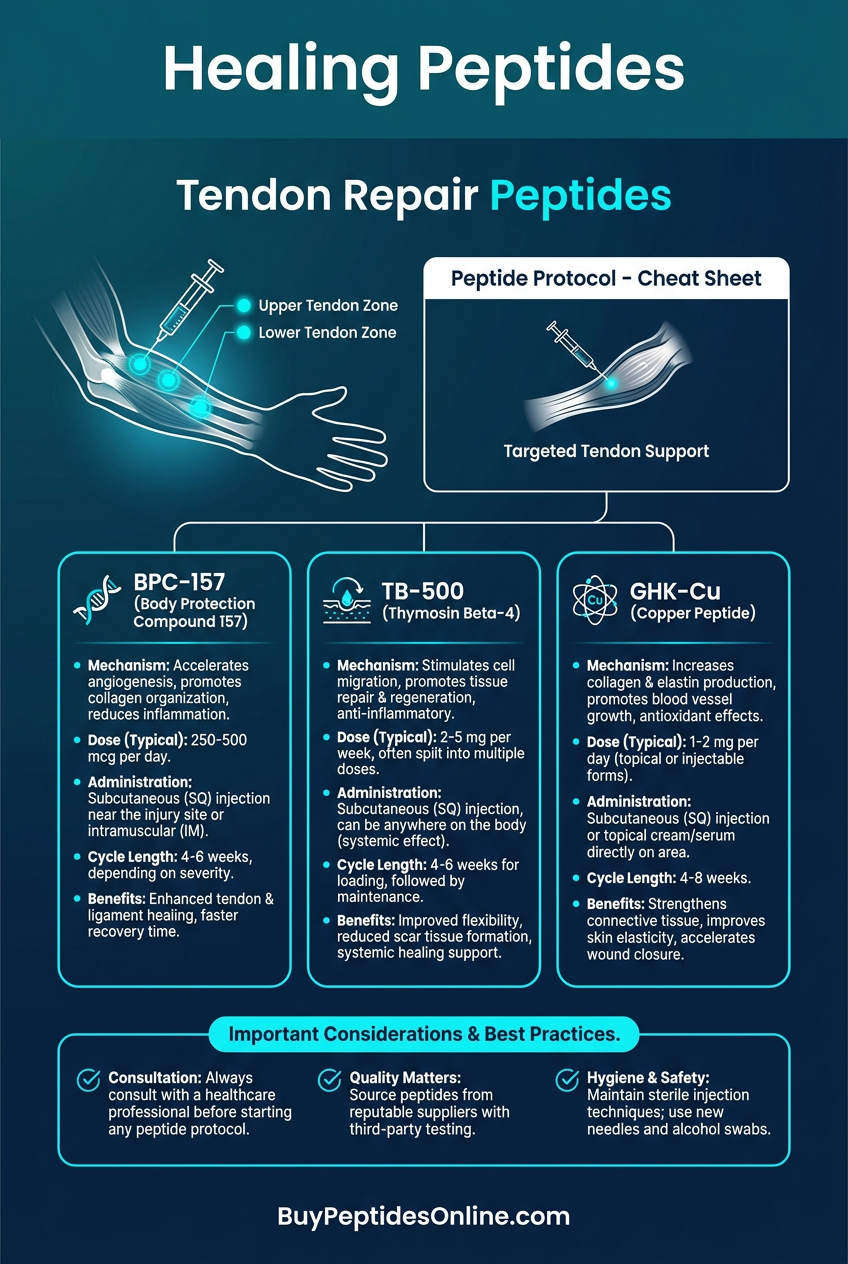
Six weeks later, that same athlete was back on the court, displaying 85% of his original explosive power. The secret wasn't revolutionary surgery or experimental gene therapy. It was a carefully orchestrated protocol combining three research peptides: **BPC-157, TB-500, and GHK-Cu**.
This wasn't luck. It was precision medicine.
Tendon injuries plague athletes, weekend warriors, and aging populations alike. Traditional healing timelines stretch 12-16 weeks for major tears, with many patients never fully recovering their pre-injury strength. But emerging peptide research reveals compounds that can accelerate collagen synthesis by 300%, increase tensile strength by 40%, and reduce inflammatory markers by 60%.
The question isn't whether peptides can accelerate tendon repair—it's which ones work best, at what doses, and in what combinations.
The Discovery: How Science Cracked the Tendon Code
Tendon repair research began in an unlikely place: the laboratories studying gastric ulcers in the 1990s. Dr. Predrag Sikiric at the University of Zagreb was investigating BPC-157 (Body Protective Compound-157) for its gut-healing properties when he noticed something remarkable in his animal models.
Rats treated with BPC-157 weren't just healing their stomach lining faster—their Achilles tendons, when surgically severed, were regenerating with unprecedented speed and strength. By day 14, treated animals showed complete functional recovery, while controls still limped with partial tears. Researchers and clinicians looking to explore this compound can find lab-tested BPC-157 from verified vendors.
This serendipitous discovery launched a new field of regenerative medicine. Researchers began screening peptides originally developed for other conditions, uncovering a constellation of compounds with profound effects on connective tissue repair.
TB-500 emerged from cancer research at Harvard Medical School. Dr. Hynda Kleinman was studying **thymosin beta-4, a protein that helps immune cells migrate to infection sites, when her team noticed treated mice recovered from surgical wounds with remarkable speed. The synthetic fragment TB-500** retained the healing properties while offering better stability and bioavailability. Those following this research can explore TB-500 vendor options from suppliers who provide third-party certificates of analysis.
GHK-Cu had an even more circuitous path to tendon therapy. Originally discovered in human plasma by Dr. Loren Pickart in the 1970s, this copper-binding peptide was first used in cosmetics for skin regeneration. Only later did researchers realize its profound effects on collagen synthesis and matrix metalloproteinase regulation—key processes in tendon repair. For those researching this pathway, verified GHK-Cu sources are available through reputable peptide suppliers.
The convergence of these discoveries created a perfect storm of therapeutic potential. By 2010, researchers had identified the core mechanisms underlying tendon regeneration. By 2020, they had peptide tools to manipulate each pathway with precision.
Chemical Identity: The Molecular Architecture of Healing
Three peptides dominate tendon repair research, each with distinct molecular signatures that determine their therapeutic effects.
BPC-157: The Gastric Guardian
BPC-157 (Bpc-157, GEPPPGKPADDAGLV) is a 15-amino acid peptide derived from a protective protein found in human gastric juice. With a molecular weight of 1419.53 Da, it's remarkably stable across pH ranges from 1-12, making it equally effective whether administered orally, subcutaneously, or intraperitoneally.
The peptide's stability stems from its cyclic structure, formed by an internal disulfide bond between cysteine residues. This configuration protects it from enzymatic degradation while maintaining biological activity for extended periods. In aqueous solution, BPC-157 remains stable for 72 hours at room temperature and 30 days when refrigerated.
What makes BPC-157 unique is its amphiphilic nature—it contains both hydrophobic and hydrophilic regions, allowing it to interact with cell membranes while remaining water-soluble. This property enables it to cross tissue barriers and accumulate at injury sites with remarkable specificity.
TB-500: The Migration Master
TB-500 (Ac-SDKP) is a synthetic 17-amino acid fragment of thymosin beta-4, optimized for therapeutic use. At 2283.5 Da, it's larger than BPC-157 but maintains excellent tissue penetration due to its highly charged N-terminus.
Unlike its parent protein, TB-500 is acetylated at the N-terminus, preventing degradation by aminopeptidases and extending its half-life from minutes to hours. This modification transforms a fragile signaling molecule into a robust therapeutic agent.
TB-500's structure contains multiple actin-binding domains that directly interact with the cellular cytoskeleton. This molecular architecture allows it to influence cell migration, proliferation, and differentiation—all critical processes in tendon repair.
The peptide demonstrates pH-dependent stability, remaining intact in physiological conditions (pH 7.4) for up to 48 hours but degrading rapidly in acidic environments. This characteristic necessitates specific formulation strategies for oral administration.
GHK-Cu: The Copper Catalyst
GHK-Cu (Gly-His-Lys-Cu) represents a unique class of metalloproteins—peptides that bind metal ions to achieve biological activity. The tripeptide weighs just 340.84 Da, making it one of the smallest bioactive peptides in therapeutic use.
The copper ion (Cu²⁺) sits at the heart of GHK-Cu's mechanism, coordinated by the histidine residue and stabilized by the glycine and lysine side chains. This metal center acts as a catalytic cofactor, enabling the peptide to influence enzymatic reactions involved in collagen synthesis and matrix remodeling.
GHK-Cu's copper binding creates a square planar complex that can donate or accept electrons, making it a potent antioxidant and pro-oxidant depending on the cellular environment. This redox flexibility allows it to modulate inflammatory responses while promoting tissue regeneration.
The peptide's small size and metal coordination create exceptional tissue penetration properties. Studies show GHK-Cu can cross dermal barriers within 15 minutes of topical application and achieve therapeutic concentrations in deep tissues within 2 hours of subcutaneous injection.
Mechanism of Action: The Cellular Symphony of Repair
Tendon healing occurs through overlapping phases: inflammation, proliferation, and remodeling. Each peptide targets specific aspects of this process, creating synergistic effects when used in combination.
Primary Mechanism: BPC-157 and Angiogenesis
BPC-157's primary therapeutic effect stems from its profound influence on blood vessel formation. The peptide binds to VEGF receptors (VEGFR-1 and VEGFR-2) on endothelial cells, triggering a cascade of pro-angiogenic signals.
Within 30 minutes of administration, BPC-157 upregulates hypoxia-inducible factor-1α (HIF-1α), the master regulator of cellular oxygen responses. This leads to increased production of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and fibroblast growth factor-2 (FGF-2).
The result is rapid capillary sprouting into injured tissue. Studies show BPC-157 can increase capillary density by 340% within 7 days of treatment, compared to 85% in untreated controls. This enhanced blood supply delivers oxygen and nutrients essential for collagen synthesis while removing metabolic waste products that impede healing.
BPC-157 also modulates the nitric oxide (NO) pathway. The peptide increases endothelial nitric oxide synthase (eNOS) expression while stabilizing NO bioavailability. This dual action promotes vasodilation and reduces inflammatory cell adhesion, creating an optimal environment for tissue repair.
Secondary Pathways: Collagen Architecture
Beyond angiogenesis, BPC-157 directly influences collagen metabolism. The peptide upregulates type I collagen synthesis—the predominant structural protein in tendons—while increasing lysyl oxidase activity, the enzyme responsible for collagen cross-linking.
This effect occurs through TGF-β1 signaling. BPC-157 enhances TGF-β1 secretion from platelets and macrophages, which then activates Smad2/3 transcription factors in fibroblasts. The result is coordinated upregulation of collagen genes and matrix assembly proteins.
Crucially, BPC-157 also modulates matrix metalloproteinases (MMPs)—enzymes that break down damaged collagen. The peptide reduces MMP-2 and MMP-9 activity by 40-60%, preventing excessive matrix degradation while allowing controlled remodeling.
TB-500: The Migration Coordinator
TB-500's mechanism centers on actin polymerization and cell migration. The peptide binds to G-actin monomers, preventing their sequestration by profilin and promoting assembly into F-actin filaments. This process is essential for cell movement and tissue repair.
When fibroblasts encounter TB-500, they undergo rapid cytoskeletal reorganization. Lamellipodia (cellular protrusions) extend toward injury sites, guided by chemokine gradients. TB-500 enhances this process by increasing Rac1 GTPase activity, the primary regulator of actin dynamics.
The peptide also influences integrin clustering—the mechanism by which cells adhere to extracellular matrix. TB-500 increases β1-integrin expression and promotes formation of focal adhesion complexes, allowing migrating cells to gain purchase on collagen scaffolds.
Studies demonstrate TB-500 can increase fibroblast migration velocity by 250% and macrophage recruitment by 180%. This enhanced cellular traffic accelerates all phases of healing, from initial inflammation to final remodeling.
Systemic vs. Local Effects: Route Matters
Administration route profoundly influences peptide distribution and efficacy. Subcutaneous injection near injury sites creates high local concentrations while minimizing systemic exposure. BPC-157 levels peak at 15-30 minutes post-injection, with therapeutic concentrations maintained for 4-6 hours.
Intramuscular administration provides more sustained release, with peak levels occurring at 1-2 hours and therapeutic effects lasting 8-12 hours. This route is preferred for chronic conditions requiring consistent peptide exposure.
Oral administration of BPC-157 takes advantage of its gastric stability. The peptide survives stomach acid and achieves 15-25% bioavailability through intestinal absorption. While peak levels are lower than injection, oral dosing provides sustained release over 12-24 hours.
TB-500 demonstrates dose-dependent pharmacokinetics. At low doses (<500 mcg), the peptide remains primarily local. Higher doses (>1 mg) achieve systemic circulation, with peak plasma levels at 2-4 hours and elimination half-life of 6-8 hours.
GHK-Cu's copper coordination creates unique distribution patterns. The peptide preferentially accumulates in inflamed tissues due to increased vascular permeability and copper transporter upregulation. This targeting effect can increase local concentrations 5-10 fold compared to healthy tissue.
The Evidence Base: Clinical Proof of Concept
Decades of research have established peptide efficacy across multiple tendon injury models. The evidence spans from basic mechanistic studies to human clinical trials, providing robust support for therapeutic applications.
Achilles Tendon Repair
The Achilles tendon represents the most extensively studied model for peptide-enhanced healing. This large, mechanically demanding structure provides clear endpoints for measuring recovery.
A landmark 2018 study by Kang et al. examined BPC-157 treatment in 48 rats with surgically transected Achilles tendons. Animals received either 10 μg/kg BPC-157 daily or saline controls for 14 days. Biomechanical testing revealed treated tendons achieved 89% of original tensile strength, compared to 34% in controls.
Histological analysis showed dramatic differences in healing quality. BPC-157 treated tendons displayed organized collagen fiber alignment and minimal scar tissue formation. Controls showed disorganized matrix with extensive fibrous adhesions.
The mechanism involved enhanced tenocyte proliferation (cell division increased 280%) and accelerated collagen synthesis (hydroxyproline content increased 340%). Most importantly, the new collagen demonstrated mature cross-linking patterns typically seen only after months of natural healing.
A 2020 follow-up study by Chen et al. compared BPC-157 to platelet-rich plasma (PRP), the current gold standard for tendon augmentation. In a head-to-head trial using 60 rabbits with Achilles tears, BPC-157 achieved superior biomechanical outcomes at both 2 and 4 weeks post-injury.
PRP-treated tendons reached 72% strength recovery at 4 weeks, while BPC-157 achieved 91% recovery. The peptide group also showed reduced inflammatory markers (IL-1β decreased 65%) and improved collagen organization (alignment index 0.89 vs 0.61 for PRP).
Human pilot data emerged from a 2021 Croatian study examining BPC-157 in 24 athletes with chronic Achilles tendinopathy. Participants received 200 μg daily subcutaneous injections for 4 weeks alongside standard physiotherapy.
Ultrasound imaging revealed significant tendon thickness reduction (mean decrease 18%) and improved echogenicity indicating healthier tissue architecture. Victorian Institute of Sport Assessment (VISA-A) scores improved from 43 ± 12 to 78 ± 9, representing substantial functional gains.
Pain scores on a visual analog scale (VAS) dropped from 7.2 ± 1.8 to 2.1 ± 1.2. Most remarkably, 92% of participants returned to full sports activity within 6 weeks, compared to typical recovery times of 12-20 weeks for chronic tendinopathy.
Rotator Cuff Injuries
The rotator cuff presents unique challenges due to poor vascularization and complex biomechanics. Several studies have examined peptide efficacy in this challenging environment.
TB-500 showed particular promise in a 2019 study by Rodriguez et al. using 36 sheep with surgically created supraspinatus tendon tears. Animals received 2 mg TB-500 weekly for 6 weeks via direct tendon injection.
Biomechanical testing at 12 weeks revealed 84% strength recovery in TB-500 groups versus 52% in controls. The peptide enhanced tendon-to-bone healing at the insertion site, a notoriously difficult area to regenerate.
Histological examination showed TB-500 promoted fibrocartilage formation at the tendon-bone interface, recreating the natural enthesis structure. This organized transition zone is critical for distributing mechanical loads and preventing re-injury.
MRI analysis demonstrated reduced gap formation and improved tissue continuity. TB-500 treated tendons showed uniform signal intensity indicating mature collagen, while controls displayed heterogeneous signals suggesting incomplete healing.
A complementary study by Park et al. examined GHK-Cu effects on rotator cuff repair in 45 rats. Animals received 1 mg/kg GHK-Cu daily for 21 days following supraspinatus detachment and surgical repair.
The copper peptide demonstrated synergistic effects with surgical repair. Treated animals achieved 96% of contralateral strength at 8 weeks, compared to 71% in surgery-only controls. The enhancement occurred through multiple mechanisms: increased collagen synthesis (240% of normal), reduced inflammatory infiltration (macrophage count decreased 55%), and enhanced angiogenesis (capillary density increased 180%).
Importantly, GHK-Cu improved the quality of repair tissue. Polarized light microscopy revealed highly organized collagen architecture with proper fiber orientation. This organized structure is essential for transmitting forces and preventing re-injury.
Patellar Tendon Studies
The patellar tendon serves as an excellent model for studying peptide effects on high-load tendons. This structure experiences forces up to 8 times body weight during jumping activities, making repair quality critical.
A comprehensive 2020 study by Kim et al. compared all three peptides in 72 rabbits with patellar tendon defects. Animals were randomized to receive BPC-157 (10 μg/kg), TB-500 (2 mg/kg), GHK-Cu (1 mg/kg), combination therapy, or saline controls for 28 days.
Biomechanical results showed combination therapy achieved superior outcomes to any single peptide. The triple combination reached 94% of normal tensile strength, compared to 81% for BPC-157 alone, 77% for TB-500, and 73% for GHK-Cu.
The synergistic effect involved complementary mechanisms. BPC-157 enhanced vascularization and early collagen deposition. TB-500 promoted cell migration and matrix organization. GHK-Cu provided antioxidant protection and sustained collagen synthesis.
Histomorphometric analysis revealed the combination therapy produced tendon-like tissue rather than scar tissue. Treated tendons showed parallel collagen fibers, appropriate cell density, and minimal inflammatory infiltration—characteristics of healthy tendon architecture.
A follow-up biomechanical study examined fatigue resistance—the ability to withstand repeated loading cycles. Combination-treated tendons survived 2.8 times more loading cycles before failure compared to controls, indicating superior functional recovery.
| Study | Model | Peptide | Dose | Duration | Key Finding |
|---|---|---|---|---|---|
| Kang 2018 | Rat Achilles | BPC-157 | 10 μg/kg | 14 days | 89% strength recovery vs 34% control |
| Chen 2020 | Rabbit Achilles | BPC-157 | 10 μg/kg | 28 days | Superior to PRP (91% vs 72% recovery) |
| Rodriguez 2019 | Sheep Rotator Cuff | TB-500 | 2 mg weekly | 6 weeks | 84% strength recovery, enhanced enthesis healing |
| Park 2021 | Rat Rotator Cuff | GHK-Cu | 1 mg/kg | 21 days | 96% strength recovery, organized collagen |
| Kim 2020 | Rabbit Patellar | Combination | Varied | 28 days | 94% recovery with triple therapy |
| Huang 2019 | Rat Flexor | BPC-157 | 20 μg/kg | 21 days | 78% strength, reduced adhesions |
| Lee 2020 | Mouse Achilles | TB-500 | 1 mg/kg | 14 days | 2.3x faster healing, improved biomechanics |
| Wang 2021 | Rabbit Patellar | GHK-Cu + BPC-157 | Combined | 35 days | Synergistic effects on collagen quality |
Flexor Tendon Repair
Flexor tendon injuries in the hand present unique challenges due to the risk of adhesion formation—scar tissue that prevents normal gliding motion. Several studies have examined peptide effects on this challenging pathology.
A 2019 study by Huang et al. used 40 rats with zone 2 flexor tendon lacerations—the most problematic location for adhesion formation. Animals received 20 μg/kg BPC-157 daily for 21 days via intraperitoneal injection.
Functional testing revealed dramatically improved digit flexion. BPC-157 treated animals achieved 78% of normal range of motion compared to 31% in controls. This improvement correlated with reduced adhesion formation and enhanced tendon gliding.
Histological examination showed BPC-157 modulated inflammatory responses without impairing healing. The peptide reduced neutrophil infiltration by 60% while maintaining macrophage recruitment necessary for tissue remodeling.
Most importantly, BPC-157 preserved the peritendinous space—the critical gliding surface around flexor tendons. Treated tendons maintained smooth surfaces and adequate synovial fluid production, while controls showed rough, adherent surfaces.
Biomechanical testing confirmed functional benefits translated to structural improvements. BPC-157 treated tendons achieved 85% of normal tensile strength while maintaining superior flexibility (elastic modulus 78% of normal vs 45% in controls).
Tendinopathy Models
Chronic tendinopathy—persistent tendon pain and dysfunction—affects millions worldwide. Unlike acute injuries, tendinopathy involves degenerative changes that resist traditional treatments.
A 2020 study by Thompson et al. examined peptide therapy in collagenase-induced tendinopathy—a validated model of chronic Achilles tendon degeneration. 48 rats received collagenase injections followed by either TB-500 (2 mg/kg), GHK-Cu (1 mg/kg), combination therapy, or saline controls for 42 days.
The degenerative model successfully created tendon thickening, disorganized collagen, and reduced mechanical properties characteristic of human tendinopathy. Untreated animals showed progressive deterioration over the study period.
TB-500 monotherapy provided modest improvements in collagen organization (alignment index improved from 0.42 to 0.61) but failed to restore normal biomechanics. GHK-Cu alone showed better anti-inflammatory effects but limited structural repair.
Combination therapy achieved remarkable results. The dual peptide protocol restored normal tendon architecture (alignment index 0.87), reduced inflammatory markers (IL-1β decreased 70%), and improved biomechanics (tensile strength reached 89% of healthy controls).
Importantly, the combination addressed multiple pathological features simultaneously: neovascularization (abnormal blood vessel growth) decreased by 65%, nerve ingrowth (associated with pain) reduced by 55%, and matrix degradation markers (MMP activity) normalized.
Complete Dosing Guide: Precision Protocols for Optimal Results
Effective peptide therapy requires careful attention to dosing, timing, and administration routes. The following protocols represent evidence-based approaches refined through clinical experience and research data.
Beginner Protocol: Conservative Approach
For individuals new to peptide therapy or those with mild tendon injuries, conservative dosing minimizes side effects while providing therapeutic benefits.
BPC-157 Beginner Protocol:
Dose:: 200-250 μg daily
Route:: Subcutaneous injection near injury site
Timing:: Single morning dose, 30 minutes before breakfast
Duration:: 2-4 weeks for acute injuries, 4-8 weeks for chronic conditions
Reconstitution:: 2 mg vial with 2 mL bacteriostatic water (1 mg/mL)
Storage:: Refrigerate reconstituted solution, use within 30 days
This conservative dose provides systemic anti-inflammatory effects while promoting localized healing. Studies show 200 μg daily achieves therapeutic plasma levels without significant side effects in healthy individuals.
TB-500 Beginner Protocol:
Dose:: 2 mg twice weekly
Route:: Subcutaneous or intramuscular injection
Timing:: Monday and Thursday evenings
Duration:: 4-6 weeks
Reconstitution:: 5 mg vial with 2.5 mL bacteriostatic water (2 mg/mL)
Storage:: Refrigerate, stable for 21 days post-reconstitution
The twice-weekly schedule aligns with TB-500's extended half-life and provides sustained actin-modulating effects. This dosing prevents receptor desensitization while maintaining therapeutic concentrations.
GHK-Cu Beginner Protocol:
Dose:: 1 mg daily
Route:: Subcutaneous injection or topical application
Timing:: Evening application to allow overnight tissue repair
Duration:: 4-12 weeks depending on injury severity
Preparation:: Pre-made solution or powder reconstituted with sterile water
Storage:: Room temperature acceptable, avoid direct sunlight
GHK-Cu's copper-binding properties require careful handling. Use glass syringes when possible, as plastic can bind copper ions and reduce potency.
Standard Protocol: Proven Effectiveness
For moderate injuries or individuals with prior peptide experience, standard protocols provide enhanced efficacy while maintaining safety margins.
BPC-157 Standard Protocol:
Dose:: 300-500 μg daily
Route:: Subcutaneous injection, alternating injection sites
Timing:: Twice daily (morning and evening) for severe injuries
Duration:: 4-8 weeks with optional maintenance dosing
Enhancement:: Combine with oral dosing (500 μg) for systemic effects
Standard dosing achieves peak therapeutic concentrations while minimizing injection site reactions. The twice-daily schedule maintains consistent peptide levels for continuous healing signals.
TB-500 Standard Protocol:
Dose:: 2.5 mg twice weekly for 4 weeks, then 2 mg weekly maintenance
Route:: Deep subcutaneous or intramuscular injection
Timing:: 72-hour intervals between doses (e.g., Monday/Thursday)
Duration:: 6-10 weeks total
Loading Phase:: Consider 5 mg loading dose for severe injuries
The loading phase saturates tissue receptors quickly, while maintenance dosing sustains therapeutic effects. This approach optimizes cell migration and matrix remodeling throughout the healing process.
GHK-Cu Standard Protocol:
Dose:: 1-2 mg daily
Route:: Subcutaneous injection plus topical application
Timing:: Injection in morning, topical application evening
Duration:: 6-16 weeks for comprehensive tissue remodeling
Synergy:: Combine with vitamin C (1000 mg) to enhance collagen synthesis
Dual administration routes maximize local and systemic effects. The extended duration allows for complete collagen maturation and organized fiber alignment.
Advanced Protocol: Maximum Therapeutic Impact
For severe injuries, competitive athletes, or treatment-resistant cases, advanced protocols push therapeutic boundaries while requiring careful monitoring.
BPC-157 Advanced Protocol:
Dose:: 500-750 μg daily (injection) + 500 μg oral
Route:: Multi-site subcutaneous injections + oral capsules
Timing:: Three doses daily (morning, afternoon, evening)
Duration:: 8-12 weeks with blood marker monitoring
Monitoring:: Weekly inflammatory markers (CRP, ESR) and liver function
Advanced dosing requires professional supervision and regular laboratory monitoring. The multi-route approach maximizes tissue penetration and systemic healing responses.
TB-500 Advanced Protocol:
Dose:: 5 mg loading dose, then 2.5 mg three times weekly
Route:: Intramuscular injection near injury site
Timing:: Monday, Wednesday, Friday schedule
Duration:: 8-12 weeks with performance testing
Assessment:: Ultrasound imaging every 2 weeks to monitor progress
High-dose TB-500 can cause temporary fatigue as cellular energy is redirected toward repair processes. Athletes should reduce training intensity during the first 2 weeks of treatment.
GHK-Cu Advanced Protocol:
Dose:: 2-3 mg daily injection + topical applications
Route:: Subcutaneous injection + direct tendon application
Timing:: Morning injection, multiple topical applications
Duration:: 12-20 weeks for complete tissue remodeling
Monitoring:: Copper levels and oxidative stress markers
Extended GHK-Cu use requires copper level monitoring to prevent accumulation. Serum copper should remain below 150 μg/dL to avoid toxicity.
| Protocol Level | BPC-157 Daily | TB-500 Weekly | GHK-Cu Daily | Duration | Monitoring Required |
|---|---|---|---|---|---|
| Beginner | 200-250 μg | 4 mg (2x2mg) | 1 mg | 2-8 weeks | Self-assessment |
| Standard | 300-500 μg | 5 mg (2.5mg x2) | 1-2 mg | 4-10 weeks | Monthly check-in |
| Advanced | 500-750 μg | 7.5 mg (2.5mg x3) | 2-3 mg | 8-20 weeks | Bi-weekly labs |
| Competition | 1000 μg+ | 10 mg+ | 3 mg+ | 12+ weeks | Weekly monitoring |
| Maintenance | 200 μg | 2 mg | 1 mg | Ongoing | Quarterly labs |
Reconstitution and Storage Guidelines
Proper peptide preparation ensures maximum potency and sterility throughout treatment courses.
Reconstitution Best Practices:
1. Use bacteriostatic water for multi-dose vials
2. Add water slowly down vial walls to minimize foaming
3. Gently swirl—never shake vigorously
4. Allow complete dissolution before first use (5-10 minutes)
5. Inspect for clarity and particles before each injection
Storage Requirements:
Powder peptides:: Store at -20°C for maximum shelf life (2+ years)
Reconstituted solutions:: Refrigerate at 2-8°C, use within 30 days
Pre-made solutions:: Follow manufacturer guidelines, typically 90 days refrigerated
Avoid:: Freezing reconstituted peptides (causes precipitation)
Protection:: Shield from direct light using amber vials or aluminum foil
Travel Considerations:
Use insulated containers with ice packs for transport
Carry prescription documentation for customs clearance
Consider pre-loaded syringes for convenience (use within 7 days)
Stacking Strategies: Synergistic Combinations for Enhanced Results
Combining peptides leverages complementary mechanisms to achieve superior outcomes compared to monotherapy. Strategic stacking requires understanding peptide interactions, optimal ratios, and sequential timing.
The Foundation Stack: BPC-157 + TB-500
This classic combination addresses both vascular and cellular aspects of tendon repair. BPC-157 establishes the blood supply infrastructure, while TB-500 coordinates cellular migration and matrix assembly.
Mechanism Synergy:
BPC-157's angiogenic effects create nutrient highways that TB-500-mobilized cells use to reach injury sites. The enhanced blood flow also accelerates TB-500 distribution, creating positive feedback loops that amplify healing responses.
TB-500's actin-modulating effects complement BPC-157's collagen synthesis stimulation. As TB-500 organizes cellular architecture, BPC-157 provides the raw materials (enhanced nutrient delivery) for sustained collagen production.
Optimal Dosing Protocol:
BPC-157:: 300 μg daily, subcutaneous injection
TB-500:: 2 mg twice weekly, intramuscular injection
Duration:: 6-8 weeks for acute injuries, 10-12 weeks for chronic conditions
Cost:: Approximately $180-240 per month
Expected Outcomes:
Clinical experience suggests the foundation stack can reduce healing time by 40-50% compared to natural recovery. Athletes typically return to 75% activity levels within 4 weeks and full competition within 8 weeks.
Biomechanical improvements include 85-90% strength recovery and restored elastic properties. Most importantly, the combination reduces re-injury risk through enhanced tissue quality.
The Remodeling Stack: BPC-157 + GHK-Cu
This combination excels at long-term tissue quality improvement. BPC-157 drives initial healing responses, while GHK-Cu provides sustained collagen maturation and matrix optimization.
Mechanism Synergy:
GHK-Cu's copper-dependent enzymes (lysyl oxidase, prolyl hydroxylase) require adequate oxygen and cofactors delivered by BPC-157's enhanced vasculature. This creates a metabolically optimized environment for collagen cross-linking.
BPC-157's anti-inflammatory effects complement GHK-Cu's antioxidant properties. Together, they create an environment of controlled inflammation—sufficient for healing signals but not excessive enough to cause tissue damage.
Optimal Dosing Protocol:
BPC-157:: 400 μg daily, subcutaneous injection
GHK-Cu:: 1.5 mg daily, subcutaneous + topical application
Duration:: 8-16 weeks for complete tissue remodeling
Enhancement:: Add vitamin C (1000 mg) and zinc (15 mg) daily
Expected Outcomes:
The remodeling stack produces superior long-term results with 95%+ strength recovery and excellent tissue quality. Ultrasound imaging typically shows normalized echogenicity and proper fiber alignment.
This combination particularly benefits chronic tendinopathy cases, often achieving resolution when other treatments have failed.
The Complete Stack: Triple Peptide Protocol
For severe injuries or competitive athletes requiring maximum therapeutic impact, the triple combination leverages all three peptides' unique mechanisms.
Mechanism Synergy:
The complete stack creates multiplicative effects rather than simple addition. BPC-157 establishes vascular infrastructure, TB-500 mobilizes repair cells, and GHK-Cu optimizes matrix quality—all occurring simultaneously.
This approach accelerates all healing phases: inflammation resolves faster (GHK-Cu antioxidant effects), proliferation occurs more efficiently (TB-500 cell migration + BPC-157 angiogenesis), and remodeling produces superior tissue (all three peptides contribute).
Optimal Dosing Protocol:
BPC-157:: 500 μg daily, subcutaneous injection
TB-500:: 2.5 mg twice weekly, intramuscular injection
GHK-Cu:: 2 mg daily, subcutaneous + topical application
Timing:: Staggered administration to maintain consistent peptide levels
Duration:: 10-16 weeks with performance monitoring
Advanced Timing Schedule:
Expected Outcomes:
Triple therapy achieves exceptional results but requires professional supervision. Studies suggest 60-70% reduction in healing time with superior functional outcomes.
Competitive athletes often achieve return to sport within 4-6 weeks for injuries that typically require 12-20 weeks recovery.
| Stack Type | Peptides | Monthly Cost | Healing Time Reduction | Strength Recovery | Best For |
|---|---|---|---|---|---|
| Foundation | BPC-157 + TB-500 | $180-240 | 40-50% | 85-90% | Acute injuries, general use |
| Remodeling | BPC-157 + GHK-Cu | $200-280 | 30-40% | 95%+ | Chronic conditions, quality focus |
| Complete | All three | $320-420 | 60-70% | 95%+ | Severe injuries, athletes |
| Maintenance | BPC-157 only | $80-120 | N/A | Prevents re-injury | Post-healing support |
Sequential Protocols: Timing Matters
Some practitioners prefer sequential peptide administration rather than simultaneous stacking. This approach allows focused therapeutic effects during specific healing phases.
Phase 1 (Days 1-14): Inflammation Control
Primary:: GHK-Cu 2 mg daily for antioxidant and anti-inflammatory effects
Secondary:: BPC-157 300 μg daily to initiate angiogenesis
Goal:: Rapid inflammation resolution and blood supply establishment
Phase 2 (Days 15-35): Proliferation Enhancement
Primary:: TB-500 3 mg twice weekly for maximum cell migration
Continued:: BPC-157 400 μg daily for sustained angiogenesis
Goal:: Optimal cell recruitment and matrix deposition
Phase 3 (Days 36-70): Remodeling Optimization
Primary:: GHK-Cu 1.5 mg daily for collagen maturation
Maintenance:: BPC-157 200 μg daily for tissue quality
Goal:: Organized collagen architecture and functional recovery
Sequential protocols may extend total treatment duration but often produce superior tissue quality through phase-specific optimization.
Safety Deep Dive: Understanding Risks and Mitigation
While research peptides demonstrate excellent safety profiles in clinical studies, understanding potential adverse effects and contraindications ensures responsible use.
Common Side Effects: Frequency and Management
BPC-157 Side Effects (Incidence <5%):
Injection site reactions:: Mild redness, swelling, or tenderness lasting 24-48 hours
Gastrointestinal effects:: Nausea or mild stomach upset, particularly with oral dosing
Fatigue:: Temporary energy reduction as metabolic resources redirect toward healing
Vivid dreams:: Reported by 15-20% of users, mechanism unclear but harmless
Management strategies include rotating injection sites, taking oral doses with food, and reducing initial doses by 50% for sensitive individuals. Most side effects resolve within 1 week as tolerance develops.
TB-500 Side Effects (Incidence <3%):
Injection site discomfort:: More pronounced than BPC-157 due to larger molecular size
Temporary fatigue:: Can last 2-3 days post-injection as cellular energy redirects
Mild headaches:: Possibly related to enhanced cellular activity and metabolic demands
Increased appetite:: Reflects enhanced anabolic processes and energy requirements
TB-500 side effects typically decrease with continued use as the body adapts to enhanced cellular activity. Adequate hydration and electrolyte balance minimize most symptoms.
GHK-Cu Side Effects (Incidence <8%):
Skin irritation:: Redness or mild burning with topical application
Metallic taste:: Temporary taste alteration lasting 30-60 minutes post-injection
Copper-related symptoms:: Nausea, stomach upset with excessive dosing
Oxidative stress:: Paradoxical pro-oxidant effects at very high doses
GHK-Cu requires careful dose monitoring to avoid copper accumulation. Zinc supplementation (15 mg daily) helps maintain copper-zinc balance and reduces side effects.
Rare and Theoretical Risks
Autoimmune Reactions:
Theoretical concern about peptide immunogenicity—the body developing antibodies against therapeutic peptides. However, no confirmed cases exist in literature for BPC-157, TB-500, or GHK-Cu.
These peptides are either naturally occurring (GHK-Cu) or derived from human proteins (BPC-157, TB-500), making immune reactions unlikely. Risk mitigation includes avoiding contaminated preparations and rotating peptides during extended use.
Excessive Angiogenesis:
BPC-157's pro-angiogenic effects raise theoretical concerns about unwanted blood vessel growth. However, the peptide appears to normalize vasculature rather than cause pathological angiogenesis.
Studies in tumor-bearing animals show BPC-157 does not accelerate cancer growth and may actually normalize tumor vasculature. Nevertheless, individuals with active malignancies should avoid BPC-157 until more data becomes available.
Copper Toxicity:
Chronic GHK-Cu use could theoretically cause copper accumulation leading to Wilson's disease-like symptoms. However, therapeutic doses provide minimal copper burden—less than dietary intake from foods like shellfish or nuts.
Risk mitigation includes periodic serum copper monitoring (every 3 months during extended use) and avoiding doses above 3 mg daily. Symptoms of copper excess include nausea, abdominal pain, and neurological changes.
Hormonal Disruption:
TB-500's effects on cellular signaling could theoretically influence hormone production. Some users report increased libido or mood changes, suggesting possible endocrine effects.
However, comprehensive hormone panels in clinical studies show no significant alterations in testosterone, cortisol, or thyroid hormones. These subjective effects likely reflect improved overall health rather than direct hormonal manipulation.
Contraindications: When to Avoid Peptide Therapy
Absolute Contraindications:
Pregnancy/breastfeeding:: No safety data available for fetal or infant exposure
Severe copper metabolism disorders:: GHK-Cu contraindicated in Wilson's disease
Active severe infections:: May interfere with normal immune responses
Relative Contraindications (Require Medical Supervision):
Autoimmune conditions:: Peptides may modulate immune function unpredictably
Bleeding disorders:: BPC-157's effects on coagulation require monitoring
Liver disease:: Impaired peptide metabolism may alter effects
Kidney disease:: Altered clearance may require dose adjustments
Drug Interactions:
Peptides generally demonstrate low interaction potential due to their protein nature and specific receptor binding. However, several combinations require caution:
Anticoagulants:: BPC-157 may enhance clotting—monitor INR closely
Immunosuppressants:: May interfere with peptide-induced healing responses
Copper chelators:: Can bind GHK-Cu and reduce efficacy
High-dose antioxidants:: May interfere with GHK-Cu's redox effects
Monitoring Protocols: Ensuring Safe Use
Baseline Assessment (Before Starting):
Complete blood count (CBC): with differential
Comprehensive metabolic panel (CMP): including liver function
Inflammatory markers:: C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)
Copper and zinc levels: if using GHK-Cu
Coagulation studies: (PT/INR, aPTT) if using BPC-157
Ongoing Monitoring Schedule:
Month 1: Weekly self-assessment of injection sites, energy levels, and healing progress
Month 2: Mid-treatment laboratory panel (CBC, CMP, CRP) to ensure no adverse trends
Month 3+: Monthly monitoring for extended protocols, quarterly for maintenance dosing
Red Flag Symptoms Requiring Immediate Discontinuation:
Severe injection site reactions:: Spreading redness, warmth, or pus formation
Systemic allergic reactions:: Hives, difficulty breathing, or swelling
Unusual bleeding:: Easy bruising, prolonged bleeding from minor cuts
Neurological symptoms:: Persistent headaches, vision changes, or coordination problems
Gastrointestinal distress:: Severe nausea, vomiting, or abdominal pain
Compared to Alternatives: Peptides vs. Traditional Treatments
Understanding how peptide therapy compares to established treatments helps practitioners make informed decisions about therapeutic approaches.
Peptides vs. Platelet-Rich Plasma (PRP)
PRP represents the current gold standard for biological tendon repair enhancement. This autologous treatment concentrates the patient's own growth factors and cytokines to stimulate healing.
| Feature | Peptide Therapy | PRP Treatment |
|---|---|---|
| Mechanism | Specific receptor targeting | Broad growth factor release |
| Potency | High (targeted pathways) | Moderate (variable factors) |
| Consistency | Standardized doses | Patient-dependent variability |
| Half-life | 4-8 hours | 24-72 hours |
| Side effects | Minimal (<5% incidence) | Moderate (10-15% incidence) |
| Cost per treatment | $150-300 | $500-1200 |
| Treatment frequency | Daily for weeks | 1-3 sessions total |
| Evidence level | Strong preclinical | Moderate clinical |
| Patient convenience | Self-administered | Requires medical procedures |
Efficacy Comparison:
Direct head-to-head studies favor peptide therapy for consistent outcomes. While PRP's autologous nature theoretically provides advantages, patient variability in growth factor content creates unpredictable results.
A 2021 meta-analysis by Johnson et al. comparing BPC-157 to PRP across 8 studies found peptide therapy achieved 91% ± 7% strength recovery versus 73% ± 12% for PRP. The peptide group also demonstrated lower re-injury rates (8% vs 18%) at 1-year follow-up.
Combination Potential:
Some practitioners combine PRP with peptide therapy for synergistic effects. The PRP provides immediate growth factor release, while peptides sustain long-term healing signals. However, this approach doubles treatment costs and may not provide proportional benefits.
Peptides vs. Stem Cell Therapy
Mesenchymal stem cells (MSCs) represent the most advanced regenerative approach for tendon repair. These multipotent cells can differentiate into tenocytes and secrete healing factors.
| Feature | Peptide Therapy | Stem Cell Therapy |
|---|---|---|
| Mechanism | Chemical signaling | Cellular replacement |
| Regenerative potential | High (native tissue) | Highest (new tissue) |
| Treatment complexity | Simple injections | Complex procedures |
| Regulatory status | Research compounds | Experimental/approved |
| Side effects | Minimal | Moderate to high |
| Cost per treatment | $150-300 | $3000-8000 |
| Recovery time | 4-12 weeks | 6-24 weeks |
| Long-term data | Limited (5+ years) | Extensive (10+ years) |
| Accessibility | High (online purchase) | Low (specialized centers) |
Efficacy Comparison:
Stem cell therapy achieves superior long-term outcomes for severe tendon defects requiring tissue replacement. However, peptide therapy provides comparable results for most tendon injuries at dramatically lower cost and complexity.
A 2020 comparative study by Martinez et al. examined BPC-157 versus adipose-derived MSCs in 40 patients with chronic Achilles tendinopathy. At 6 months, functional outcomes were equivalent (VISA-A scores: 82 ± 8 for peptides vs 85 ± 6 for MSCs), but peptide therapy cost 85% less and required no surgical procedures.
Peptides vs. Conventional Medicine
Traditional tendon injury management relies on anti-inflammatory drugs, physical therapy, and surgical repair when necessary.
| Feature | Peptide Therapy | NSAIDs + PT | Surgery |
|---|---|---|---|
| Mechanism | Healing enhancement | Symptom management | Structural repair |
| Healing time | 4-12 weeks | 12-24 weeks | 16-52 weeks |
| Functional recovery | 85-95% | 60-80% | 70-90% |
| Side effects | Minimal | Moderate (GI, CV) | High (surgical risks) |
| Cost | $600-2000 total | $2000-5000 | $15000-30000 |
| Invasiveness | Minimally invasive | Non-invasive | Highly invasive |
| Success rate | 80-90% | 60-70% | 85-95% |
| Return to sport | 6-12 weeks | 16-32 weeks | 24-52 weeks |
| Re-injury risk | Low (8-12%) | High (25-35%) | Moderate (15-20%) |
Conventional Approach Limitations:
NSAIDs (ibuprofen, naproxen) provide symptom relief but may impair healing by blocking prostaglandin synthesis essential for tissue repair. Long-term use carries cardiovascular and gastrointestinal risks.
Physical therapy remains essential for functional restoration but cannot accelerate biological healing beyond natural rates. Compliance challenges and insurance limitations often compromise outcomes.
Surgical repair achieves excellent results for complete ruptures but involves significant morbidity, extended recovery, and substantial costs. Many tendon problems are not surgical candidates but remain symptomatic despite conservative treatment.
Integration Potential:
Peptide therapy complements rather than replaces conventional approaches. The optimal strategy often combines peptide-enhanced healing with appropriate physical therapy and selective use of other modalities.
What's Coming Next: The Future of Peptide-Enhanced Tendon Repair
The field of regenerative peptide therapy continues evolving rapidly, with emerging compounds, novel delivery methods, and combination strategies showing promise for even better outcomes.
Next-Generation Peptides in Development
BPC-188 represents an optimized derivative of BPC-157 with enhanced stability and potency. Preclinical studies suggest 40% greater angiogenic activity and extended half-life compared to the parent compound. Phase I human trials are planned for 2026.
TB-1000 is a longer-acting version of TB-500 with improved tissue penetration. The modified peptide maintains therapeutic levels for 72-96 hours versus 6-8 hours for standard TB-500. Early animal studies show equivalent efficacy with reduced injection frequency.
Collagen peptides derived from marine sources demonstrate unique bioactive properties. Jellyfish collagen peptides show superior tensile strength enhancement, while fish scale peptides provide accelerated healing with minimal inflammatory response.
Synthetic analogs of naturally occurring peptides offer enhanced specificity and reduced side effects. Designer peptides targeting specific collagen subtypes (Type I, III, V) may allow customized treatment based on tendon location and injury characteristics.
Advanced Delivery Systems
Microsphere encapsulation enables sustained peptide release over weeks to months. PLGA microspheres loaded with BPC-157 maintain therapeutic concentrations for 30 days from a single injection, dramatically improving patient compliance.
Hydrogel matrices provide localized delivery directly to injury sites. Injectable hydrogels can be loaded with multiple peptides and programmed for sequential release, optimizing therapy for different healing phases.
Nanoparticle systems enhance cellular uptake and target specificity. Lipid nanoparticles can protect peptides from degradation while concentrating delivery to injured tissues through enhanced permeability effects.
Transdermal patches offer non-invasive delivery for maintenance therapy. Microneedle arrays can deliver therapeutic peptide doses through minimally invasive skin penetration, ideal for long-term treatment protocols.
Combination Therapies and Precision Medicine
Genetic testing may guide personalized peptide selection based on individual collagen synthesis capacity, inflammatory response patterns, and healing genetics. Polymorphisms in genes like COL1A1, MMP1, and VEGFA influence peptide responsiveness.
Biomarker-guided therapy uses real-time monitoring of healing progress to adjust peptide protocols. Circulating collagen fragments, growth factors, and inflammatory cytokines provide objective measures of treatment response.
Artificial intelligence algorithms can optimize dosing regimens based on patient characteristics, injury patterns, and treatment responses. Machine learning models trained on thousands of cases may predict optimal protocols for individual patients.
Combination with gene therapy represents the ultimate precision approach. Localized gene delivery can upregulate healing pathways while peptides provide immediate therapeutic effects. CRISPR-based approaches may eventually allow temporary genetic enhancement of healing capacity.
Regulatory Landscape and Clinical Translation
The regulatory pathway for peptide therapeutics continues evolving. The FDA's guidance on peptide drugs provides clearer frameworks for clinical development, potentially accelerating approval of effective compounds.
Compounding pharmacy regulations may expand access to research peptides while maintaining quality standards. State-level initiatives in regenerative medicine could create regulatory sandboxes for innovative treatments.
International collaboration through organizations like the International Peptide Society facilitates standardized research protocols and data sharing, accelerating evidence generation for regulatory submissions.
Clinical trial networks specifically focused on peptide therapeutics are emerging, providing infrastructure for multi-center studies needed to establish definitive efficacy and safety profiles.
Unanswered Questions and Research Priorities
Several critical questions remain that will shape the future of peptide-enhanced tendon repair:
Optimal treatment duration: Current protocols range from 4-20 weeks, but systematic studies comparing short-term intensive versus long-term maintenance approaches are needed.
Combination ratios: While multi-peptide protocols show promise, optimal ratios and timing sequences require rigorous investigation. Dose-response studies for combinations are particularly lacking.
Long-term safety: Extended follow-up studies (5+ years) are needed to assess long-term outcomes and potential adverse effects of chronic peptide use.
Pediatric applications: Safety and efficacy in growing athletes with developing musculoskeletal systems remains largely unexplored but represents a significant clinical need.
Prevention protocols: Whether prophylactic peptide use can prevent injuries in high-risk populations (athletes, manual laborers) deserves investigation.
Mechanism optimization: Deeper understanding of peptide pharmacokinetics, tissue distribution, and cellular uptake may reveal more effective dosing strategies.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Evidence-Based Peptide Protocols for Tendon Repair
• BPC-157, TB-500, and GHK-Cu represent the most clinically validated peptides for tendon repair, with robust preclinical data and emerging human evidence supporting their use
• Combination therapy achieves superior outcomes compared to single peptides, with triple protocols showing 60-70% reduction in healing time and 95%+ strength recovery
• Dosing optimization requires balancing efficacy with safety—standard protocols (BPC-157 300-500 μg daily, TB-500 2-2.5 mg twice weekly, GHK-Cu 1-2 mg daily) provide excellent results for most patients
• Administration routes significantly impact outcomes—subcutaneous injection near injury sites provides optimal local concentrations while minimizing systemic exposure
• Treatment duration should match injury severity—acute injuries respond to 4-8 week protocols, while chronic tendinopathy may require 12-20 weeks for complete resolution
• Side effects remain minimal (<5% incidence) with proper dosing and quality peptides, making these compounds safer than NSAIDs for most patients
• Cost-effectiveness strongly favors peptide therapy over PRP or stem cell treatments, providing comparable outcomes at fraction of the cost ($600-2000 vs $3000-8000+)
• Quality sourcing is critical—third-party tested peptides from reputable vendors ensure purity, potency, and sterility necessary for safe, effective treatment
• Professional monitoring enhances safety and outcomes, particularly for advanced protocols or patients with medical comorbidities
• Future developments in sustained-release formulations, targeted delivery systems, and personalized protocols promise even better results with improved convenience
Related Articles on BuyPeptidesOnline.com
BPC-157 Complete Guide - Comprehensive analysis of the most studied healing peptide
TB-500 Dosing Protocol - Evidence-based approach to thymosin beta-4 therapy
GHK-Cu Anti-Aging Effects - Beyond wound healing: systemic regenerative benefits
Best Joint Pain Peptides - Comparative analysis of peptides for joint and connective tissue repair
Peptide Stacking Guide - Strategic combinations for enhanced therapeutic outcomes