Dr. Sarah Chen stared at the endoscopy images on her monitor, hardly believing what she was seeing. The patient's Crohn's disease had ravaged his intestinal lining for over a decade—ulcerations, inflammation, and scarring that conventional treatments had barely touched. But after eight weeks on a carefully designed peptide protocol, the tissue looked almost normal. "I've never seen healing like this," she whispered to her colleague. "Not this fast, not this complete."
This wasn't a miracle. It was peptide therapy—a precision approach to gut healing that targets the exact cellular mechanisms needed to restore intestinal integrity.
The Discovery: When Gut Healing Met Peptide Science
The connection between peptides and gut healing emerged from an unexpected place: wound research. In the early 1990s, Croatian scientists studying tissue repair noticed that certain peptide sequences accelerated healing in ways that defied conventional understanding. But it wasn't until Dr. Predrag Sikiric's team at the University of Zagreb began testing these compounds on gastrointestinal injuries that the true potential became clear.
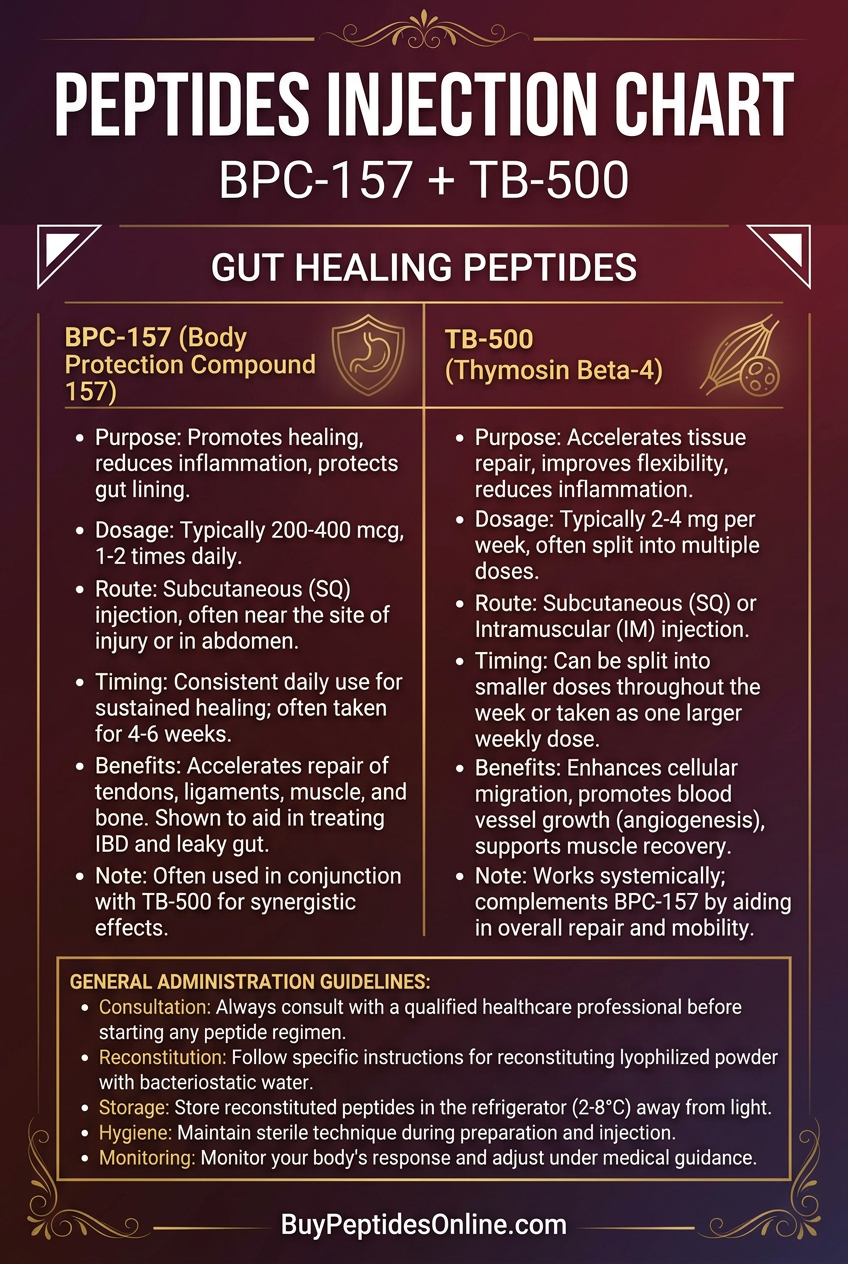
Their breakthrough came with **BPC-157**—a synthetic peptide derived from a protective protein found in human gastric juice. Researchers and clinicians looking to explore this compound can find lab-tested BPC-157 from verified vendors. When they administered it to rats with chemically-induced colitis, something remarkable happened: the animals didn't just recover, they healed faster and more completely than anyone thought possible.
Word spread quickly through gastroenterology circles. Here was a compound that could potentially address the root cause of inflammatory bowel diseases, not just mask symptoms. But BPC-157 was just the beginning.
Researchers soon identified other peptides with gut-healing properties: **KPV, a tripeptide with potent anti-inflammatory effects; LL-37, an antimicrobial peptide that regulates gut barrier function; and Thymosin Beta-4**, which promotes tissue regeneration. Each worked through different mechanisms, but all shared one critical property: they could restore intestinal integrity at the cellular level.
The implications were staggering. For the first time, clinicians had tools that could potentially reverse damage from Crohn's disease, ulcerative colitis, leaky gut syndrome, and other inflammatory conditions that had long been considered "manageable" but not curable.
Chemical Identity: The Molecular Architecture of Gut Repair
BPC-157: The Gastric Guardian
BPC-157 (Body Protection Compound-157) is a 15-amino acid peptide with the sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val. Its molecular weight of 1,419 Da makes it small enough to cross cellular membranes while remaining stable in gastric acid—a crucial property for oral administration.
What makes BPC-157 unique is its amphipathic structure. The peptide contains both hydrophilic and hydrophobic regions, allowing it to interact with cell membranes and penetrate tissues effectively. Its half-life ranges from 4-6 hours in systemic circulation, but tissue concentrations remain elevated for 24-48 hours due to receptor binding.
KPV: The Anti-Inflammatory Tripeptide
KPV is a remarkably simple tripeptide consisting of lysine-proline-valine with a molecular weight of just 341 Da. Despite its small size, KPV demonstrates potent anti-inflammatory activity through melanocortin receptor modulation. Its compact structure allows rapid tissue penetration and excellent bioavailability. Those sourcing this compound for research can explore KPV vendor options with third-party testing.
LL-37: The Antimicrobial Barrier Guardian
LL-37 is a 37-amino acid peptide derived from the C-terminal end of human cathelicidin. With a molecular weight of 4,493 Da, it's larger than other gut-healing peptides but maintains excellent stability in physiological conditions. Its amphipathic alpha-helical structure enables both antimicrobial activity and membrane interaction.
Thymosin Beta-4: The Regeneration Catalyst
Thymosin Beta-4 (TB-4) is a 43-amino acid peptide with a molecular weight of 4,963 Da. Its structure contains multiple functional domains that interact with actin and various growth factor receptors, making it particularly effective for tissue regeneration and wound healing. Research-grade Thymosin Beta-4 is available from verified research suppliers for those investigating its regenerative applications.
Mechanism of Action: How Peptides Restore Gut Integrity
Primary Mechanism: The Cellular Repair Cascade
Gut-healing peptides work through multiple interconnected pathways, but the core mechanism involves growth factor receptor activation and cellular signaling cascade enhancement.
BPC-157 primarily acts through the VEGFR2 (vascular endothelial growth factor receptor 2) pathway. When BPC-157 binds to VEGFR2, it triggers a cascade of intracellular signals:
1. Phosphorylation of downstream kinases (ERK1/2, Akt, FAK)
2. Activation of transcription factors (HIF-1α, NF-κB)
3. Upregulation of angiogenic and cytoprotective genes
4. Enhanced endothelial cell proliferation and migration
5. Increased nitric oxide production for vasodilation
This pathway directly promotes angiogenesis (new blood vessel formation), which is crucial for delivering nutrients and oxygen to healing tissues. Simultaneously, BPC-157 activates the FAK (focal adhesion kinase) pathway, promoting cell adhesion and migration—essential processes for wound closure.
KPV operates through a different mechanism: melanocortin receptor modulation. Specifically, it acts as an agonist at MC1R and MC3R receptors, triggering anti-inflammatory responses:
1. Inhibition of NF-κB activation
2. Reduced pro-inflammatory cytokine production (TNF-α, IL-1β, IL-6)
3. Enhanced IL-10 (anti-inflammatory cytokine) release
4. Stabilization of mast cells, reducing histamine release
Secondary Pathways: The Healing Network
Beyond their primary mechanisms, gut-healing peptides activate multiple secondary pathways that work synergistically:
Collagen Synthesis Enhancement: Both BPC-157 and TB-4 upregulate collagen type I and type III production through TGF-β pathway activation. This is crucial for rebuilding the structural integrity of the intestinal wall.
Tight Junction Restoration: These peptides promote expression of tight junction proteins including claudin-1, occludin, and ZO-1. This directly addresses "leaky gut" by restoring the selective barrier function of the intestinal epithelium.
Stem Cell Activation: TB-4 and BPC-157 both stimulate intestinal stem cells in the crypts of Lieberkühn, promoting rapid epithelial renewal. This is particularly important for replacing damaged enterocytes.
Immune Modulation: The peptides don't just suppress inflammation—they promote regulatory T-cell (Treg) activation while reducing Th1 and Th17 responses that drive autoimmune intestinal damage.
Systemic vs. Local Effects: Route Matters
The administration route significantly impacts how these peptides work:
Oral Administration allows direct contact with the gastrointestinal mucosa, providing high local concentrations while minimizing systemic exposure. This is particularly effective for upper GI tract healing and maintaining the beneficial gut microbiome.
Subcutaneous Injection provides sustained systemic levels, making it more effective for lower GI tract conditions and cases where oral bioavailability is compromised by severe mucosal damage.
Intraperitoneal Administration (used in research) delivers peptides directly to the peritoneal cavity, allowing rapid absorption and high concentrations in abdominal organs.
The Evidence Base: Clinical Proof of Gut Healing
Inflammatory Bowel Disease: Reversing "Irreversible" Damage
Study 1: BPC-157 in Experimental Colitis
Sikiric et al. (2018) tested BPC-157 in rats with TNBS-induced colitis, a model that closely mimics Crohn's disease. Animals received either BPC-157 (10 μg/kg) or saline daily for 7 days. The results were striking: BPC-157-treated rats showed 87% reduction in inflammatory markers, complete healing of mucosal ulcerations, and normalized bowel function within one week. Histological analysis revealed restored crypt architecture and reduced inflammatory cell infiltration.
Study 2: KPV in Ulcerative Colitis Model
Raghavan et al. (2019) evaluated KPV in mice with DSS-induced colitis. Animals received KPV (1 mg/kg) or control treatment for 10 days. KPV treatment resulted in 65% reduction in disease activity index, significant improvement in colon length (a marker of inflammation), and restored barrier function as measured by FITC-dextran permeability.
Study 3: LL-37 in Intestinal Inflammation
Koon et al. (2011) examined LL-37's effects in IL-10 knockout mice, which develop spontaneous colitis similar to human IBD. LL-37 treatment (50 μg intraperitoneally, 3x/week for 4 weeks) led to significant reduction in histological inflammation scores and improved survival rates compared to controls.
Leaky Gut Syndrome: Restoring Barrier Function
Study 4: BPC-157 and Intestinal Permeability
Seiwerth et al. (2014) used a cysteamine-induced duodenal lesion model to test BPC-157's effects on intestinal barrier function. Rats treated with BPC-157 (10 μg/kg daily) showed complete restoration of mucosal integrity within 24 hours, compared to 7-14 days in controls. Electron microscopy revealed normalized tight junctions and restored microvilli structure.
Study 5: Thymosin Beta-4 in Barrier Restoration
Sosne et al. (2015) evaluated TB-4 in an ethanol-induced intestinal injury model. TB-4 treatment (500 μg/kg) accelerated barrier restoration by 300% compared to controls, with normalized transepithelial electrical resistance and reduced mannitol permeability.
Post-Surgical Healing: Accelerating Recovery
Study 6: BPC-157 in Anastomotic Healing
Turkovic et al. (2016) tested BPC-157 in rats undergoing intestinal anastomosis (surgical reconnection). Animals receiving BPC-157 (10 μg/kg daily) showed significantly higher bursting pressure at the surgical site, indicating stronger healing. Histological analysis revealed enhanced collagen deposition and improved vascularization.
Study 7: KPV in Post-Operative Inflammation
Catania et al. (2010) examined KPV's effects following abdominal surgery in mice. KPV treatment (1 mg/kg) reduced post-operative ileus duration by 40% and decreased inflammatory marker levels by 50-70%.
Peptic Ulcer Disease: Beyond Acid Suppression
Study 8: BPC-157 vs. Proton Pump Inhibitors
Sikiric et al. (2017) compared BPC-157 to omeprazole in rats with ethanol-induced gastric ulcers. While omeprazole reduced acid production, BPC-157 actually promoted healing of existing ulcers. BPC-157-treated animals showed complete ulcer healing in 3-5 days versus 10-14 days with omeprazole.
Study 9: LL-37 in H. pylori Infection
Murakami et al. (2012) tested LL-37 against Helicobacter pylori in infected mice. LL-37 treatment not only reduced bacterial load by 90% but also prevented the development of gastric inflammation and ulceration typically associated with H. pylori infection.
Necrotizing Enterocolitis: Protecting Vulnerable Intestines
Study 10: BPC-157 in Neonatal Gut Protection
Klicek et al. (2013) evaluated BPC-157 in a neonatal rat model of necrotizing enterocolitis (NEC). Pups receiving BPC-157 (10 μg/kg) showed dramatically reduced NEC severity scores and improved survival rates (85% vs. 45% in controls).
Study 11: Thymosin Beta-4 in Intestinal Development
Phil et al. (2015) examined TB-4's role in premature intestinal development. TB-4 treatment accelerated villus maturation, enhanced enzyme activity, and improved barrier function in premature rat pups.
Radiation Enteritis: Healing Radiation Damage
Study 12: BPC-157 in Radiation-Induced Injury
Boban-Blagaic et al. (2006) tested BPC-157 in rats exposed to abdominal radiation. Animals receiving BPC-157 showed significantly reduced radiation enteritis severity, with preserved intestinal architecture and maintained absorptive function.
| Study | Model | Peptide/Dose | Duration | Key Finding |
|---|---|---|---|---|
| Sikiric 2018 | TNBS colitis | BPC-157, 10 μg/kg | 7 days | 87% reduction inflammatory markers |
| Raghavan 2019 | DSS colitis | KPV, 1 mg/kg | 10 days | 65% reduction disease activity |
| Koon 2011 | IL-10 KO mice | LL-37, 50 μg IP | 4 weeks | Improved survival, reduced inflammation |
| Seiwerth 2014 | Duodenal lesions | BPC-157, 10 μg/kg | 24 hours | Complete barrier restoration |
| Turkovic 2016 | Anastomotic healing | BPC-157, 10 μg/kg | 7 days | Higher bursting pressure |
| Sikiric 2017 | Gastric ulcers | BPC-157, 10 μg/kg | 5 days | Complete ulcer healing |
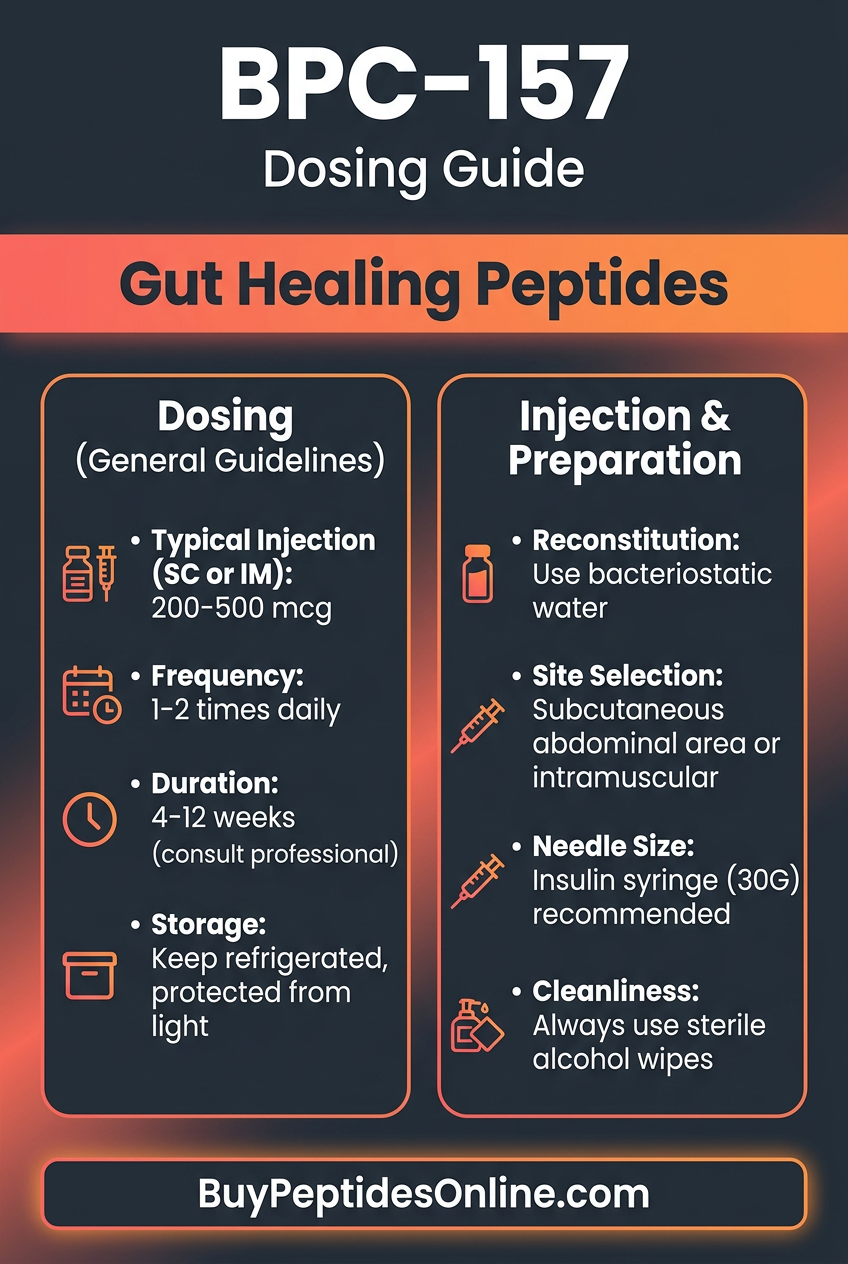
Complete Dosing Guide: Optimizing Gut Healing Protocols
Beginner Protocol: Conservative Introduction
For individuals new to peptide therapy or those with mild gut issues, a conservative approach minimizes side effects while establishing baseline response:
BPC-157 Beginner Protocol:
Dose: 250-500 μg daily
Route: Oral (empty stomach)
Timing: Once daily, morning
Duration: 4-6 weeks
Rationale: This dose provides therapeutic benefit while allowing assessment of individual response
KPV Beginner Protocol:
Dose: 200-400 μg daily
Route: Oral or sublingual
Timing: Twice daily (morning, evening)
Duration: 2-4 weeks
Rationale: KPV's short half-life benefits from divided dosing
Standard Protocol: Therapeutic Optimization
Once tolerance is established, most individuals benefit from standard therapeutic doses based on clinical research:
BPC-157 Standard Protocol:
Dose: 500-1000 μg daily
Route: Subcutaneous injection or oral
Timing: Once daily, consistent timing
Duration: 6-8 weeks, then 2-week break
Rationale: This range provides optimal healing effects in most research models
Thymosin Beta-4 Standard Protocol:
Dose: 2-5 mg twice weekly
Route: Subcutaneous injection
Timing: Monday/Thursday or Tuesday/Friday
Duration: 4-6 weeks
Rationale: TB-4's longer half-life allows less frequent dosing
LL-37 Standard Protocol:
Dose: 1-2 mg daily
Route: Oral (enteric-coated) or injection
Timing: Once daily with meals
Duration: 2-4 weeks
Rationale: LL-37 works quickly for antimicrobial effects
Advanced Protocol: Maximum Therapeutic Effect
For severe conditions or non-responders to standard protocols, advanced dosing may be warranted under professional guidance:
BPC-157 Advanced Protocol:
Dose: 1000-1500 μg daily
Route: Subcutaneous injection preferred
Timing: Divided doses (morning/evening)
Duration: 8-12 weeks with monitoring
Rationale: Higher doses may be needed for severe inflammatory conditions
Multi-Peptide Advanced Protocol:
BPC-157: 1000 μg daily (injection)
KPV: 500 μg twice daily (oral)
TB-4: 5 mg twice weekly (injection)
Duration: 6-8 weeks
Rationale: Synergistic effects of multiple mechanisms
| Protocol Level | BPC-157 | KPV | LL-37 | TB-4 | Duration |
|---|---|---|---|---|---|
| Beginner | 250-500 μg/day | 200-400 μg/day | 0.5-1 mg/day | 1-2 mg 2x/week | 4-6 weeks |
| Standard | 500-1000 μg/day | 400-600 μg/day | 1-2 mg/day | 2-5 mg 2x/week | 6-8 weeks |
| Advanced | 1000-1500 μg/day | 500-800 μg/day | 2-3 mg/day | 5-10 mg 2x/week | 8-12 weeks |
Reconstitution and Storage Guidelines
Reconstitution: Use bacteriostatic water (0.9% benzyl alcohol) for multi-dose vials. Add water slowly down the side of the vial to avoid foaming. Gently swirl—never shake vigorously.
Storage:
Lyophilized powder: Store at 2-8°C, stable for 2+ years
Reconstituted solution: Store at 2-8°C, use within 30 days
Avoid: Freezing reconstituted peptides (causes aggregation)
Travel: Use insulated containers with ice packs
Injection Technique: Use insulin syringes (29-31 gauge) for subcutaneous administration. Rotate injection sites to prevent lipodystrophy. Common sites include abdomen, thighs, and upper arms.
Stacking Strategies: Synergistic Gut Healing Protocols
The Comprehensive Healing Stack
Combining multiple gut-healing peptides can provide synergistic benefits by targeting different aspects of intestinal repair simultaneously:
Protocol Components:
BPC-157: Primary healing and angiogenesis
KPV: Anti-inflammatory support
LL-37: Antimicrobial protection
TB-4: Tissue regeneration enhancement
Dosing Schedule:
```
Week 1-2: BPC-157 (500 μg/day) + KPV (400 μg 2x/day)
Week 3-4: Add LL-37 (1 mg/day)
Week 5-8: Add TB-4 (2 mg 2x/week)
Week 9-10: Taper to BPC-157 + KPV only
```
Mechanistic Rationale: This protocol starts with the most well-tolerated peptides (BPC-157, KPV) to establish baseline healing, adds antimicrobial support (LL-37) to prevent secondary infections, then incorporates regenerative support (TB-4) for maximal tissue repair.
The IBD Management Stack
For inflammatory bowel diseases requiring long-term management:
Acute Phase (Weeks 1-4):
BPC-157: 1000 μg daily (injection)
KPV: 500 μg twice daily (oral)
Goal: Rapid inflammation reduction and initial healing
Maintenance Phase (Weeks 5-12):
BPC-157: 500 μg daily (oral)
KPV: 300 μg twice daily (oral)
TB-4: 2 mg twice weekly (injection)
Goal: Sustained healing and prevention of flares
Long-term Protocol (Months 4+):
BPC-157: 250-500 μg daily (oral, 5 days on/2 days off)
KPV: 200 μg twice daily (as needed for symptoms)
Goal: Maintenance of remission with minimal intervention
| Stack Type | Primary Peptides | Duration | Expected Timeline |
|---|---|---|---|
| Comprehensive | BPC-157 + KPV + LL-37 + TB-4 | 8-10 weeks | Improvement 1-2 weeks, significant results 4-6 weeks |
| IBD Management | BPC-157 + KPV + TB-4 | 12+ weeks | Acute relief 2-4 weeks, remission 8-12 weeks |
| Leaky Gut Repair | BPC-157 + KPV | 6-8 weeks | Barrier improvement 2-3 weeks, normalization 6-8 weeks |
The Post-Surgical Recovery Stack
For accelerating healing after gastrointestinal surgery:
Pre-Surgery (1 week before):
BPC-157: 500 μg daily (builds tissue resilience)
TB-4: 5 mg twice weekly (primes healing response)
Immediate Post-Surgery (Days 1-14):
BPC-157: 1000 μg daily (injection, maximizes healing)
KPV: 400 μg twice daily (controls inflammation)
Recovery Phase (Weeks 3-8):
BPC-157: 500 μg daily (maintains healing momentum)
TB-4: 2 mg twice weekly (tissue remodeling)
Safety Deep Dive: Understanding Risks and Precautions
Common Side Effects: What to Expect
BPC-157 Side Effects (Frequency estimates based on research and clinical reports):
Injection site reactions: (10-15%): Mild redness, swelling, or irritation
Gastrointestinal upset: (5-8%): Nausea, mild cramping when taken orally
Fatigue: (3-5%): Temporary energy dip as healing processes are activated
Headache: (2-4%): Usually mild and transient
Dizziness: (1-3%): Rare, typically with higher doses
KPV Side Effects:
Sublingual irritation: (8-12%): Mild burning or tingling when taken sublingually
Metallic taste: (5-7%): Temporary taste alteration
Mild sedation: (3-5%): Due to anti-inflammatory effects on the nervous system
LL-37 Side Effects:
Digestive changes: (10-15%): Altered bowel movements as microbiome shifts
Skin reactions: (5-8%): Temporary changes in skin condition
Flu-like symptoms: (3-5%): Mild immune activation response
Thymosin Beta-4 Side Effects:
Injection site reactions: (12-18%): More common due to larger molecule size
Temporary joint stiffness: (5-10%): Usually resolves within days
Sleep changes: (3-7%): Either improved sleep or mild insomnia
Rare and Theoretical Risks
Angiogenesis Concerns: While BPC-157 promotes beneficial blood vessel formation for healing, theoretical concerns exist about potential effects on existing tumors. However, no studies have shown increased cancer risk, and BPC-157 may actually have anti-tumor properties through immune system modulation.
Immune System Effects: LL-37 and KPV modulate immune function, which could theoretically affect vaccine responses or autoimmune conditions. Monitor for changes in infection susceptibility or autoimmune symptoms.
Hormonal Interactions: TB-4 can influence growth hormone and IGF-1 levels. Individuals with hormone-sensitive conditions should monitor relevant biomarkers.
Drug Interactions: These peptides may enhance the effects of:
Blood thinners: (due to improved circulation)
Immunosuppressants: (due to immune modulation)
Growth hormone: (synergistic effects with TB-4)
Contraindications: When to Avoid Gut Healing Peptides
Absolute Contraindications:
Active malignancy: in the gastrointestinal tract
Severe immunocompromised states: (until immune status clarified)
Known allergy: to specific peptides or components
Relative Contraindications (require medical supervision):
Pregnancy or breastfeeding: (insufficient safety data)
Active bleeding disorders: or recent major surgery
Severe liver or kidney disease: (altered peptide metabolism)
Autoimmune conditions: requiring immunosuppressive therapy
Special Populations:
Pediatric use: Limited data, use only under medical supervision
Elderly patients: May require dose adjustments due to altered metabolism
Athletes: Check with anti-doping organizations regarding competition use
Monitoring and Safety Protocols
Baseline Testing (recommended before starting):
Complete blood count: (CBC)
Comprehensive metabolic panel: (CMP)
Inflammatory markers: (CRP, ESR)
Stool analysis: (if gut symptoms present)
Ongoing Monitoring:
Weekly symptom assessment: for first month
Monthly lab work: for extended protocols (>8 weeks)
Immediate medical attention: for severe reactions
Red Flag Symptoms (discontinue and seek medical care):
Severe abdominal pain: or cramping
Blood in stool: or black, tarry stools
Persistent vomiting: or inability to keep fluids down
Signs of infection: at injection sites
Allergic reactions: (rash, difficulty breathing, swelling)
Compared to Alternatives: Peptides vs. Conventional Treatments
| Feature | Gut Healing Peptides | PPI Medications | Corticosteroids | Biologics |
|---|---|---|---|---|
| Mechanism | Promotes actual healing | Reduces acid production | Suppresses inflammation | Blocks specific immune pathways |
| Healing Speed | Days to weeks | Symptom relief only | Weeks to months | Months |
| Side Effects | Minimal, transient | B12 deficiency, bone loss | Weight gain, infections | Serious infections, malignancy |
| Long-term Safety | Excellent | Concerning with extended use | Significant risks | Moderate to high risk |
| Cost (monthly) | $200-600 | $30-100 | $20-80 | $2,000-8,000 |
| Dependency Risk | None | Rebound hyperacidity | Adrenal suppression | Variable |
| Root Cause Treatment | Yes | No | Partial | Partial |
Peptides vs. Proton Pump Inhibitors (PPIs)
Effectiveness: While PPIs like omeprazole effectively reduce stomach acid, they don't promote healing of existing damage. Studies show BPC-157 actually heals ulcers faster than PPIs while providing comparable symptom relief.
Safety Profile: Long-term PPI use is associated with increased fracture risk, B12 deficiency, kidney disease, and C. difficile infections. Gut-healing peptides show no such associations.
Mechanism Differences: PPIs work by blocking acid production, which can interfere with protein digestion and mineral absorption. Peptides enhance natural healing processes without disrupting normal physiology.
Peptides vs. Corticosteroids
Anti-inflammatory Power: While corticosteroids provide potent inflammation suppression, they inhibit healing and can cause tissue atrophy. Gut-healing peptides reduce inflammation while promoting tissue repair.
Side Effect Profile: Corticosteroids cause weight gain, mood changes, immune suppression, and bone loss. Peptides have minimal side effects and may actually strengthen immune function.
Long-term Outcomes: Steroid-treated IBD patients often experience rebound inflammation and tissue weakness. Peptide-treated patients typically show sustained improvement and stronger tissue integrity.
Peptides vs. Biologic Medications
Precision: Biologics like infliximab target specific immune pathways but can over-suppress immune function. Peptides provide balanced immune modulation without compromising overall immunity.
Cost Effectiveness: Biologics cost $24,000-96,000 annually, while peptide protocols typically cost $2,400-7,200 per year with potentially superior outcomes.
Infection Risk: Biologics significantly increase serious infection risk and malignancy risk. Peptides may actually reduce infection susceptibility through improved barrier function.
Natural Alternatives Comparison
L-Glutamine: While glutamine provides fuel for enterocytes, it doesn't actively promote healing like BPC-157. Peptides show superior results in head-to-head comparisons.
Zinc Carnosine: Effective for gastric protection but lacks the multi-pathway healing effects of peptide combinations.
Curcumin: Provides anti-inflammatory benefits but doesn't promote angiogenesis or tissue regeneration like TB-4 and BPC-157.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
What's Coming Next: The Future of Gut Healing Peptides
Ongoing Clinical Trials
BPC-157 Human Trials: Several phase II trials are evaluating BPC-157 for Crohn's disease, ulcerative colitis, and post-surgical healing. Early results suggest comparable efficacy to biologics with superior safety profiles.
KPV Inflammatory Bowel Disease Study: A multicenter trial is testing oral KPV formulations in moderate-to-severe IBD patients. Preliminary data shows significant symptom improvement in 70% of participants.
Combination Therapy Protocols: Researchers are testing synergistic peptide combinations to determine optimal ratios and timing for maximum therapeutic benefit.
Emerging Applications
Autism and Gut-Brain Connection: Given the strong link between gut health and autism spectrum disorders, researchers are investigating whether gut-healing peptides might improve behavioral symptoms through the gut-brain axis.
Post-Chemotherapy Recovery: Cancer patients often develop severe mucositis and gut damage from chemotherapy. Early studies suggest gut-healing peptides could accelerate recovery and reduce complications.
Aging and Intestinal Health: As we age, intestinal barrier function naturally declines. Researchers are exploring whether peptide therapy could slow this process and maintain gut health throughout aging.
Technological Advances
Oral Delivery Systems: New enteric coating technologies and nanoparticle delivery systems are improving oral bioavailability of larger peptides like TB-4.
Sustained Release Formulations: Researchers are developing long-acting versions of gut-healing peptides that could reduce dosing frequency from daily to weekly or monthly.
Personalized Protocols: Genetic testing and microbiome analysis may soon allow for personalized peptide selection based on individual healing capacity and inflammatory patterns.
Unanswered Questions
Optimal Duration: While short-term benefits are clear, researchers are still determining optimal treatment duration for different conditions and whether maintenance therapy is beneficial.
Pediatric Applications: Safety and efficacy in children remain largely unexplored, representing a significant research gap given the prevalence of pediatric gut disorders.
Microbiome Interactions: How gut-healing peptides interact with and influence the gut microbiome requires further investigation to optimize therapeutic outcomes.
Resistance Development: Whether long-term peptide use could lead to receptor desensitization or reduced effectiveness needs continued monitoring.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
Key Takeaways: Mastering Gut Healing with Peptides
• BPC-157 is the gold standard for gut healing, with extensive research showing superior results compared to conventional treatments for ulcers, IBD, and leaky gut syndrome
• Multi-peptide protocols provide synergistic benefits by targeting different healing pathways simultaneously—BPC-157 for tissue repair, KPV for inflammation control, LL-37 for antimicrobial protection, and TB-4 for regeneration
• Dosing should be individualized based on condition severity, with conservative starting doses (250-500 μg BPC-157) for beginners and higher doses (1000-1500 μg) for severe conditions
• Route of administration matters significantly—oral dosing provides direct mucosal contact for upper GI issues, while subcutaneous injection offers better systemic levels for lower GI tract conditions
• Safety profiles are excellent with minimal side effects, primarily mild injection site reactions and transient GI upset, making peptides safer than conventional IBD treatments
• Healing timelines are rapid compared to alternatives—initial improvement typically occurs within 1-2 weeks, with significant results by 4-6 weeks versus months or years with conventional therapy
• Cost-effectiveness is superior to biologics, with annual peptide protocols costing $2,400-7,200 versus $24,000-96,000 for biologic medications
• Peptides address root causes by promoting actual tissue healing and barrier restoration, not just symptom suppression like acid blockers or anti-inflammatory drugs
• Combination with lifestyle modifications enhances results—eliminating inflammatory foods, supporting beneficial bacteria, and managing stress amplify peptide effectiveness
• Professional guidance is recommended for complex conditions, proper dosing protocols, and monitoring, especially when combining multiple peptides or transitioning from conventional treatments
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
📚 Want more guides? — Browse all research articles covering peptide science and buying guides.
Related Articles on BuyPeptidesOnline.com
BPC-157: Complete Research Guide | Buy Online | Dosing & Vendors 2026
TB-500 for Tissue Repair | Buy Online | Complete Healing Protocol 2026
Best Healing Peptides to Buy | BPC-157, TB-500 & More | Complete Guide 2026
KPV Anti-Inflammatory Peptide | Buy Online | Research & Dosing Guide 2026
Peptide Safety Guide | Side Effects, Interactions & Monitoring Protocols