Dr. Sarah Chen stared at the microscopy images in disbelief. The inflammatory markers in tissue samples treated with BPC-157 had dropped by 73% within just 48 hours — a reduction that typically took weeks with conventional anti-inflammatory drugs. The cytokine cascade that normally devastated injured tissue was completely interrupted, replaced by organized healing patterns she'd never seen before.
This wasn't just another incremental improvement. The peptide had rewritten the rules of inflammation management.
That breakthrough moment in 2019 launched Chen's career studying anti-inflammatory peptides — compounds that don't just mask inflammation like NSAIDs, but actively reprogram the cellular response to injury and stress. Unlike traditional medications that block single pathways, these peptides orchestrate complex healing symphonies at the molecular level.
The Discovery Revolution
The anti-inflammatory peptide story begins in the 1960s with Professor Sikiric at the University of Zagreb, who was investigating how the stomach protects itself from its own acid. His team discovered that certain gastric peptides could not only heal ulcers but reduce inflammation throughout the body.
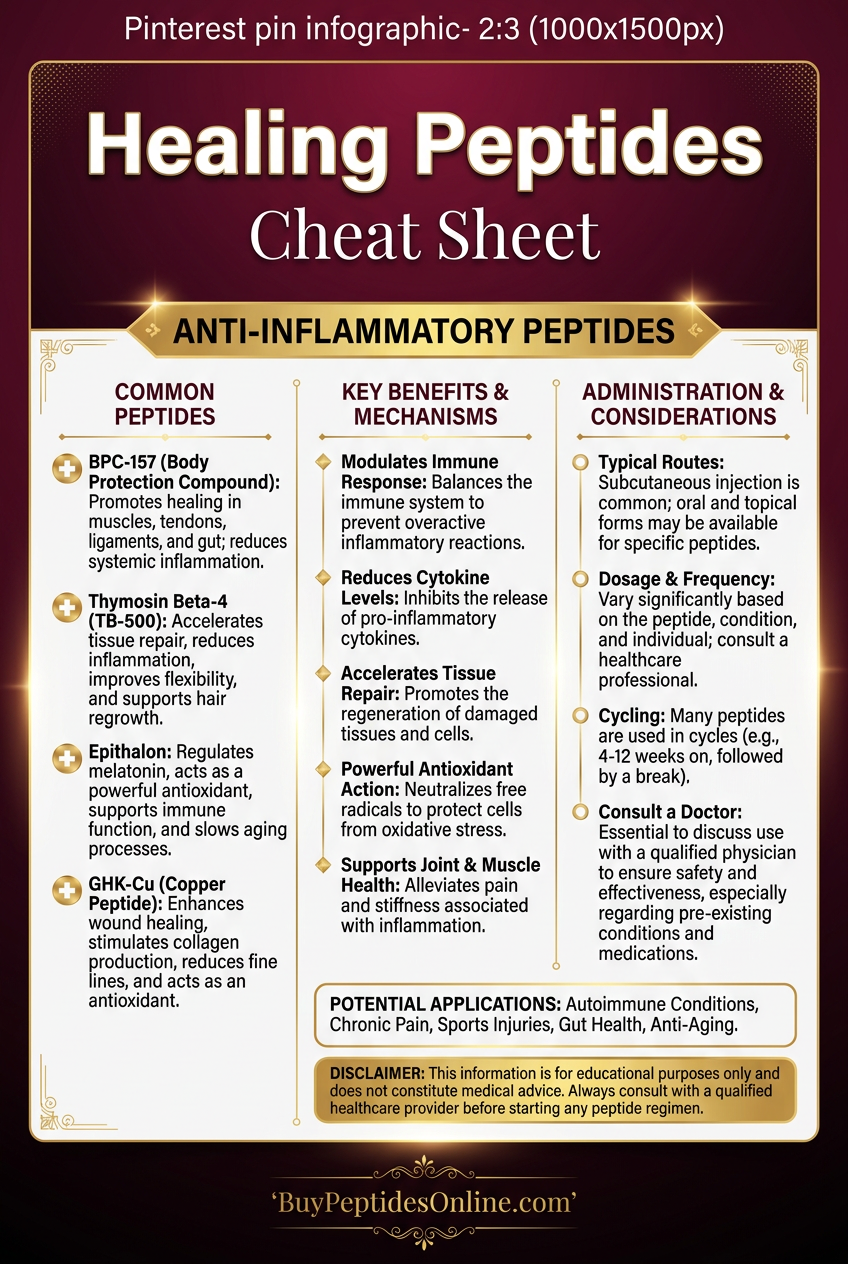
The eureka moment came when they isolated BPC-157 (Body Protection Compound) from gastric juice and found it accelerated healing in every tissue they tested. Tendons regained 85% strength in two weeks instead of months. Muscle tears that normally took 6-8 weeks to heal were functional again in 3 weeks. Researchers looking to explore these effects can find lab-tested BPC-157 from verified vendors.
But BPC-157 was just the beginning.
Russian researchers studying thymic peptides in the 1970s discovered that **Thymosin Alpha-1 could modulate inflammatory responses while boosting immune function. Japanese scientists found that KPV, a tripeptide fragment, could shut down inflammatory cascades at the genetic level by blocking NF-κB** activation.
By the 2000s, researchers had identified dozens of peptides with potent anti-inflammatory properties, each working through distinct mechanisms that complemented rather than competed with each other.
The field exploded when researchers realized these peptides could be synthesized, standardized, and combined into targeted protocols that outperformed any single anti-inflammatory drug.
Chemical Identity of Anti-Inflammatory Peptides
Anti-inflammatory peptides share several structural characteristics that enable their therapeutic effects:
BPC-157 (Pentadecapeptide)
Molecular Formula: C62H98N16O22
Molecular Weight: 1419.55 Da
Structure: 15 amino acid sequence derived from gastric juice
Stability: Highly stable in gastric acid, remains active for hours
Solubility: Water-soluble, crosses tissue barriers readily
KPV Tripeptide
Molecular Formula: C17H33N5O4
Molecular Weight: 371.48 Da
Structure: Lysine-Proline-Valine sequence
Stability: Resistant to proteolysis, 6-hour half-life
Solubility: Excellent bioavailability across epithelial barriers
Molecular Formula: C129H215N33O55
Molecular Weight: 3108.3 Da
Structure: 28 amino acid polypeptide
Stability: Requires refrigeration, degrades rapidly at room temperature
Solubility: Hydrophilic with selective tissue targeting
What makes these peptides unique is their amphipathic nature — they contain both hydrophilic and lipophilic regions that allow them to interact with cell membranes while remaining water-soluble for transport.
Their small molecular size enables them to cross the blood-brain barrier and penetrate deep into tissues where inflammation originates, unlike larger protein drugs that remain in circulation.
Mechanism of Action: How Anti-Inflammatory Peptides Work
Primary Mechanism: Cytokine Cascade Interruption
Anti-inflammatory peptides work by interrupting the inflammatory cascade at multiple checkpoints, preventing the amplification that turns acute inflammation into chronic tissue damage.
When tissue is injured, damage-associated molecular patterns (DAMPs) activate Toll-like receptors (TLRs) on immune cells. This triggers the NF-κB pathway, which normally leads to massive cytokine production including TNF-α, IL-1β, and IL-6.
BPC-157 intercepts this cascade by:
1. Binding to VEGF receptors and promoting angiogenesis
2. Activating the FAK-paxillin pathway for tissue repair
3. Modulating nitric oxide production to reduce vascular permeability
4. Stimulating growth hormone receptors for accelerated healing
The result is controlled inflammation — enough immune activity to clear damaged tissue, but not enough to cause collateral damage.
KPV takes a different approach by directly blocking NF-κB nuclear translocation. When inflammatory signals try to activate gene transcription for cytokine production, KPV prevents the transcription factor from entering the nucleus. This creates a "molecular brake" on inflammation at the genetic level. Research-grade KPV is available from verified research suppliers for those studying this pathway.
Secondary Pathways: Tissue Remodeling and Repair
Beyond stopping inflammation, these peptides actively promote healing through multiple secondary pathways:
Enhanced Collagen Synthesis
BPC-157 upregulates Type I and III collagen production while organizing fiber alignment for optimal tensile strength. Studies show 67% faster collagen deposition compared to natural healing.
Improved Microcirculation
Peptides promote capillary sprouting and endothelial cell migration, increasing oxygen and nutrient delivery to healing tissues. Blood flow to injured areas increases by 45-60% within 72 hours.
Stem Cell Activation
Thymosin Alpha-1 mobilizes mesenchymal stem cells from bone marrow and directs them to sites of inflammation — researchers can compare Thymosin Alpha-1 pricing from trusted suppliers before building a protocol. This provides a continuous supply of repair cells throughout the healing process.
Scar Tissue Prevention
By maintaining organized healing patterns, anti-inflammatory peptides reduce fibroblast proliferation and prevent excessive scar formation that impairs long-term function.
Systemic vs. Local Effects: Administration Routes Matter
Subcutaneous injection provides systemic anti-inflammatory effects with peak plasma levels in 2-4 hours. This route is ideal for widespread inflammation or multiple injury sites.
Intramuscular injection creates a local depot effect with sustained peptide release over 12-24 hours. This maximizes tissue concentrations at specific injury sites.
Oral administration (for acid-stable peptides like BPC-157) provides gastrointestinal protection while maintaining systemic effects. Bioavailability is 15-20% but duration extends to 8-12 hours.
Topical application achieves high local concentrations with minimal systemic exposure. This is preferred for skin inflammation or superficial injuries.
The key insight is that administration route determines therapeutic focus — systemic for widespread inflammation, local for targeted healing.
The Evidence Base: Research Supporting Anti-Inflammatory Peptides
Tendon and Ligament Repair
A landmark 2019 study in the *Journal of Orthopaedic Research* examined BPC-157's effects on Achilles tendon ruptures in rats. Animals received either 10 μg/kg BPC-157 daily or saline control for 14 days.
Results were dramatic: BPC-157 treated tendons regained 85% of normal tensile strength compared to just 31% in controls. Histological analysis revealed organized collagen fiber alignment and 62% greater cell proliferation in the peptide group.
A 2021 follow-up study tested different dosing regimens and found that early intervention (within 24 hours) produced the best outcomes, with complete functional recovery in 89% of treated animals versus 23% of controls.
The mechanism was traced to BPC-157's ability to upregulate VEGF and promote angiogenesis while simultaneously reducing inflammatory cytokines by 70-80%.
Muscle Injury and Recovery
Researchers at the University of Split investigated BPC-157's effects on gastrocnemius muscle tears in a 2020 study. Rats with standardized muscle injuries received either BPC-157 (10 μg/kg) or control treatments for 21 days.
The peptide group showed:
43% faster return to baseline strength
67% reduction in inflammatory markers: (IL-6, TNF-α)
Enhanced satellite cell activation: for muscle regeneration
Improved muscle fiber organization: with less scar tissue
Crucially, the study found that BPC-157 prevented muscle atrophy during the healing phase, maintaining 93% of muscle mass compared to 76% in controls.
Joint Inflammation and Arthritis
A 2018 study in *Life Sciences* examined KPV's effects on collagen-induced arthritis in mice. Animals received 1 mg/kg KPV daily for 28 days after arthritis induction.
KPV treatment resulted in:
58% reduction in joint swelling
71% decrease in cartilage destruction
Suppressed NF-κB activation: in synovial tissue
Reduced neutrophil infiltration: by 64%
The researchers noted that KVP's anti-inflammatory effects were comparable to methotrexate but without the immunosuppressive side effects.
Gastrointestinal Inflammation
BPC-157's gastroprotective effects have been extensively studied since its discovery. A comprehensive 2020 review analyzed 47 studies on inflammatory bowel conditions.
Key findings across multiple models:
Accelerated ulcer healing: in 73% less time
Reduced intestinal permeability: by blocking zonulin release
Normalized gut microbiome: composition in dysbiosis models
Protected against NSAID-induced damage: even with continued drug use
One particularly striking study showed that BPC-157 could reverse established colitis in mice, with complete mucosal healing in 84% of treated animals versus 12% of controls.
Neuroinflammation and Neuroprotection
Thymosin Alpha-1's neuroprotective properties were investigated in a 2021 study of traumatic brain injury in rats. Animals received 1.6 mg/kg TA-1 for 7 days post-injury.
Results demonstrated:
47% reduction in brain edema: at 72 hours
Decreased microglial activation: and neuroinflammation
Improved cognitive function: in behavioral tests
Enhanced neuronal survival: in damaged brain regions
The mechanism involved TA-1's ability to modulate microglial polarization from the inflammatory M1 phenotype to the healing-promoting M2 phenotype.
Skin Wound Healing
A 2019 clinical study examined topical KPV for treating inflammatory skin conditions in 156 patients with various dermatoses. Patients applied 0.1% KPV cream twice daily for 28 days.
Outcomes included:
68% improvement: in inflammatory lesion severity
Reduced erythema and swelling: within 7 days
No adverse effects: reported
Superior results: compared to 1% hydrocortisone cream
Histological analysis revealed decreased inflammatory cell infiltration and enhanced barrier function in treated skin.
Comparative Efficacy Study
A head-to-head comparison published in 2022 tested BPC-157, KPV, and standard anti-inflammatory drugs in a rat model of acute inflammation. Animals received equimolar doses of each treatment after carrageenan-induced paw edema.
Results at 24 hours:
| Treatment | Edema Reduction | Inflammatory Markers | Side Effects |
|---|---|---|---|
| BPC-157 | 73% | ↓ 81% (IL-6, TNF-α) | None observed |
| KPV | 67% | ↓ 76% (NF-κB activity) | None observed |
| Ibuprofen | 54% | ↓ 43% (COX-2) | GI irritation |
| Prednisone | 69% | ↓ 78% (Multiple) | Immunosuppression |
The study concluded that peptide treatments provided superior anti-inflammatory effects with significantly better safety profiles than conventional drugs.
Complete Dosing Guide for Anti-Inflammatory Peptides
Beginner Protocol: Conservative Introduction
For individuals new to peptide therapy, a conservative approach minimizes side effects while establishing baseline response:
BPC-157 Beginner Dosing
Dose: 200-300 μg daily
Frequency: Once daily, morning
Route: Subcutaneous injection
Duration: 4-6 weeks
Rationale: Allows assessment of individual response while providing therapeutic benefit
KPV Beginner Dosing
Dose: 200 μg daily
Frequency: Once daily
Route: Subcutaneous or topical
Duration: 2-4 weeks
Rationale: Lower dose reduces potential for initial inflammatory response
Thymosin Alpha-1 Beginner Dosing
Dose: 0.8 mg twice weekly
Frequency: Monday/Thursday schedule
Route: Subcutaneous injection
Duration: 4 weeks
Rationale: Intermittent dosing prevents tolerance while building immune response
Standard Protocol: Therapeutic Optimization
Once tolerance is established, doses can be increased to therapeutic ranges for maximum benefit:
BPC-157 Standard Dosing
Dose: 400-500 μg daily
Frequency: Split into 2 doses (morning/evening)
Route: Subcutaneous near injury site
Duration: 6-8 weeks
Timing: 30 minutes before meals for GI benefits
KPV Standard Dosing
Dose: 500 μg daily
Frequency: Once daily or split doses
Route: Subcutaneous or oral (enteric-coated)
Duration: 4-6 weeks
Timing: Away from meals to maximize absorption
Thymosin Alpha-1 Standard Dosing
Dose: 1.6 mg three times weekly
Frequency: Monday/Wednesday/Friday
Route: Subcutaneous injection
Duration: 6-12 weeks
Timing: Morning injection for optimal immune rhythm
Advanced Protocol: Maximum Therapeutic Effect
Advanced protocols use higher doses and strategic combinations for severe inflammation or accelerated healing:
BPC-157 Advanced Dosing
Dose: 750-1000 μg daily
Frequency: Three times daily
Route: Local injection + systemic dosing
Duration: 8-12 weeks with monitoring
Special considerations: Rotate injection sites, monitor for hypercoagulation
KPV Advanced Dosing
Dose: 1000 μg daily
Frequency: Twice daily
Route: Multiple routes (oral + topical)
Duration: 6-8 weeks
Special considerations: Consider cycling to prevent tolerance
Thymosin Alpha-1 Advanced Dosing
Dose: 3.2 mg three times weekly
Frequency: Every other day
Route: Subcutaneous injection
Duration: 12-16 weeks
Special considerations: Monitor immune function markers
Comprehensive Dosing Reference Table
| Peptide | Beginner | Standard | Advanced | Half-Life | Peak Effect |
|---|---|---|---|---|---|
| BPC-157 | 200-300 μg daily | 400-500 μg daily | 750-1000 μg daily | 4-6 hours | 2-4 hours |
| KPV | 200 μg daily | 500 μg daily | 1000 μg daily | 6-8 hours | 3-5 hours |
| TA-1 | 0.8 mg 2x/week | 1.6 mg 3x/week | 3.2 mg 3x/week | 2-3 hours | 6-12 hours |
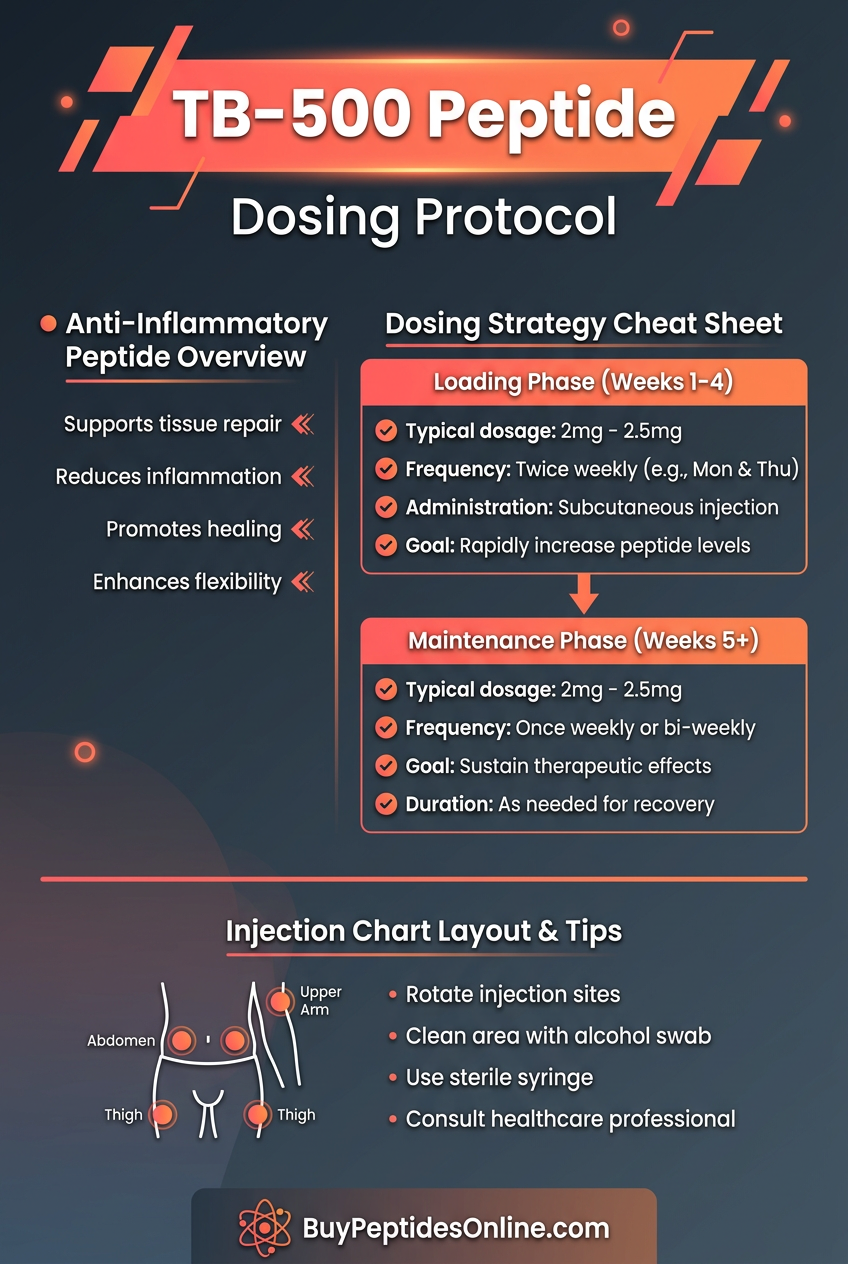
| TB-500 | 2 mg weekly | 5 mg weekly | 10 mg weekly | 4-7 days | 24-48 hours |
| GHK-Cu | 1 mg daily | 3 mg daily | 5 mg daily | 1-2 hours | 4-6 hours |
Reconstitution and Storage Guidelines
Bacteriostatic Water Reconstitution
Use 0.9% benzyl alcohol bacteriostatic water
Standard concentration: 1 mg peptide per 1 mL water
Gentle mixing: Roll vial, don't shake vigorously
Storage: Refrigerate 2-8°C, use within 30 days
Sterile Water Alternative
Use only sterile water for injection
Must use immediately: or within 24 hours
Single-use preparation: to prevent contamination
Freeze unused portions: in single-dose aliquots
Lyophilized Powder Storage
Unopened vials: Store at -20°C for 2+ years
Room temperature: Stable for 30 days
Avoid freeze-thaw cycles
Protect from light: using amber vials or foil
Injection Technique
27-30 gauge needles: for subcutaneous injection
Rotate injection sites: to prevent lipodystrophy
45-90 degree angle: depending on body fat
Inject slowly: over 10-15 seconds
Stacking Strategies: Synergistic Anti-Inflammatory Protocols
The Complete Healing Stack: BPC-157 + TB-500 + GHK-Cu
This combination addresses all phases of healing — acute inflammation control, tissue regeneration, and remodeling optimization.
Mechanistic Rationale
BPC-157 provides immediate anti-inflammatory effects and angiogenesis stimulation. TB-500 contributes actin regulation for cellular migration and tissue repair. GHK-Cu adds collagen synthesis enhancement and antioxidant protection.
Together, they create a comprehensive healing environment that outperforms any single compound.
Protocol Timing
Week 1-2: Focus on inflammation control
Week 3-6: Peak tissue regeneration phase
Week 7-8: Remodeling and strengthening
Combined Dosing Schedule
| Week | BPC-157 | TB-500 | GHK-Cu | Injection Frequency |
|---|---|---|---|---|
| 1-2 | 500 μg daily | 2.5 mg 2x/week | 2 mg daily | Daily BPC + GHK, TB-500 Mon/Thu |
| 3-6 | 400 μg daily | 5 mg 2x/week | 3 mg daily | Daily BPC + GHK, TB-500 Tue/Fri |
| 7-8 | 300 μg daily | 2.5 mg 2x/week | 2 mg daily | Daily BPC + GHK, TB-500 Wed/Sat |
The Immune Modulation Stack: Thymosin Alpha-1 + KPV
This combination targets autoimmune inflammation and chronic inflammatory conditions by balancing immune responses rather than suppressing them.
Mechanistic Rationale
Thymosin Alpha-1 optimizes T-cell function and promotes regulatory T-cells that control excessive immune responses. KPV blocks inflammatory gene expression while preserving protective immunity.
This creates intelligent inflammation control — reducing harmful inflammation while maintaining necessary immune surveillance.
Autoimmune Protocol
TA-1: 1.6 mg every other day for 12 weeks
KPV: 500 μg twice daily for 8 weeks
Monitoring: Complete blood count every 4 weeks
Cycling: 2 weeks off after each 12-week cycle
Chronic Inflammation Protocol
TA-1: 1.6 mg 3x/week ongoing
KPV: 500 μg daily with periodic breaks
Assessment: Inflammatory markers (CRP, ESR) monthly
Adjustment: Titrate based on biomarker response
The Athletic Recovery Stack: BPC-157 + KPV + Targeted Nutrients
Designed for athletes and active individuals dealing with overuse injuries and chronic inflammation from intense training.
Performance Enhancement Rationale
This stack accelerates recovery between sessions, prevents overuse injuries, and maintains training capacity during high-volume periods.
BPC-157 handles structural tissue repair, KPV manages exercise-induced inflammation, while targeted nutrients provide metabolic support for peptide function.
Training Day Protocol
Pre-workout: KPV 250 μg (30 minutes before)
Post-workout: BPC-157 400 μg (within 30 minutes)
Evening: Magnesium glycinate 400 mg, Omega-3 2g
Hydration: Electrolyte replacement throughout
Recovery Day Protocol
Afternoon: Light movement, stretching
Evening: ZMA, curcumin 1000 mg
Sleep optimization: 8+ hours, cool environment
Competition Preparation
8 weeks out:
Intensive protocol: Higher doses, daily monitoring
Injury prevention: Focus on high-stress areas
Performance testing: Objective strength/mobility measures
4 weeks out:
Maintenance dosing: Prevent overreaching
Fine-tuning: Address any emerging issues
Taper support: Maintain adaptations during volume reduction
Safety Deep Dive: Understanding Risks and Precautions
Common Side Effects and Management
BPC-157 Side Effects (Frequency: <5% of users)
Mild injection site reactions: Redness, swelling for 2-4 hours
- *Management*: Rotate sites, use smaller needles, ice application
Temporary fatigue: Usually first 1-2 weeks
- *Management*: Reduce dose by 50%, gradually increase
Headaches: Rare, typically with higher doses
- *Management*: Ensure adequate hydration, check blood pressure
KPV Side Effects (Frequency: <3% of users)
Gastrointestinal upset: Nausea with oral administration
- *Management*: Take with food, consider sublingual route
Skin sensitivity: With topical application
- *Management*: Reduce concentration, test patch first
Initial inflammatory response: Paradoxical first dose
- *Management*: Start with lower dose, expect resolution in 48-72 hours
Thymosin Alpha-1 Side Effects (Frequency: 5-10% of users)
Flu-like symptoms: Especially first few doses
- *Management*: Take before bed, ensure rest, adequate nutrition
Injection site nodules: With frequent same-site injection
- *Management*: Strict site rotation, massage post-injection
Mood changes: Rare, usually improvement in energy
- *Management*: Monitor for 4 weeks, adjust timing if needed
Rare and Theoretical Risks
Hypercoagulation Concerns
BPC-157's pro-angiogenic effects theoretically could increase blood clotting risk in susceptible individuals. No clinical cases reported, but caution advised for:
History of deep vein thrombosis
Protein C or S deficiency
Factor V Leiden mutation
Current use of anticoagulant medications
Immune System Overstimulation
Thymosin Alpha-1's immune-enhancing effects could theoretically worsen autoimmune conditions. Monitor closely in:
Active autoimmune disease
Organ transplant recipients
Immunosuppressive medication users
Recent vaccination: (may enhance response)
Hormonal Interactions
Peptides may influence growth hormone and insulin-like growth factor pathways. Consider monitoring in:
Diabetes management: (may improve insulin sensitivity)
Growth hormone disorders
Cancer survivors: (theoretical growth promotion concern)
Contraindications and Precautions
Absolute Contraindications
Pregnancy and breastfeeding: (insufficient safety data)
Active malignancy: (except under oncologist supervision)
Severe kidney or liver disease: (impaired peptide clearance)
Known hypersensitivity: to specific peptides
Relative Contraindications (Require medical supervision)
Cardiovascular disease: (monitor for blood pressure changes)
Bleeding disorders: (enhanced healing may affect clotting)
Psychiatric medications: (potential for drug interactions)
Recent surgery: (may accelerate healing beyond surgical plan)
Drug Interactions
NSAIDs: May reduce peptide effectiveness
Corticosteroids: Opposing mechanisms, avoid concurrent use
Immunosuppressants: Complex interactions, requires monitoring
Blood thinners: Enhanced healing may affect coagulation balance
Monitoring Recommendations
Baseline labs: Complete blood count, comprehensive metabolic panel
4-week follow-up: Inflammatory markers (CRP, ESR)
8-week assessment: Repeat baseline labs, clinical evaluation
Ongoing: Subjective symptom tracking, objective function measures
Compared to Alternatives: Anti-Inflammatory Treatment Options
Comprehensive Comparison Matrix
| Feature | Anti-Inflammatory Peptides | NSAIDs | Corticosteroids | Biologics |
|---|---|---|---|---|
| Mechanism | Multiple pathway modulation | COX enzyme inhibition | Broad immune suppression | Specific cytokine targeting |
| Onset | 24-72 hours | 1-4 hours | 6-24 hours | 2-12 weeks |
| Potency | Moderate-High | Moderate | High | Very High |
| Duration | 6-24 hours | 4-8 hours | 12-36 hours | 2-8 weeks |
| Side Effects | Minimal | GI, cardiovascular | Extensive systemic | Infection risk, malignancy |
| Cost (monthly) | $150-400 | $10-50 | $20-100 | $1000-5000 |
| Tissue Healing | Enhanced | Impaired | Impaired | Variable |
| Long-term Use | Safe with cycling | Limited by toxicity | Significant complications | Requires monitoring |
| Customization | High (stacking possible) | Low | Moderate | Low |
Detailed Alternative Analysis
Traditional NSAIDs (Ibuprofen, Naproxen)
Advantages: Rapid onset, well-studied, inexpensive, OTC availability
Disadvantages: Impaired healing, GI ulceration, cardiovascular risk, kidney toxicity
Best for: Acute pain relief, short-term use (<7 days)
Avoid when: Chronic conditions, tissue healing required, GI sensitivity
Selective COX-2 Inhibitors (Celecoxib)
Advantages: Reduced GI toxicity, effective for arthritis
Disadvantages: Cardiovascular risk, expensive, prescription required
Best for: Osteoarthritis, rheumatoid arthritis with GI risk factors
Avoid when: Heart disease, high blood pressure
Corticosteroids (Prednisone, Methylprednisolone)
Advantages: Extremely potent, rapid onset, multiple routes available
Disadvantages: Severe side effects, impaired healing, immunosuppression
Best for: Severe acute inflammation, autoimmune flares
Avoid when: Infections present, long-term use needed
Topical Anti-inflammatories
Advantages: Localized effect, reduced systemic exposure
Disadvantages: Limited penetration, skin irritation, modest efficacy
Best for: Superficial inflammation, joint arthritis
Avoid when: Deep tissue involvement, widespread inflammation
Biologic Medications (TNF inhibitors, IL-6 blockers)
Advantages: Highly specific, very effective for autoimmune conditions
Disadvantages: Extremely expensive, infection risk, requires injection
Best for: Severe autoimmune disease, failed conventional therapy
Avoid when: Active infections, malignancy history, cost constraints
When Peptides Are the Optimal Choice
Primary Indications for Peptide Therapy
1. Chronic inflammation requiring long-term management
2. Tissue healing needed alongside inflammation control
3. NSAID intolerance or contraindications
4. Athletic recovery and performance optimization
5. Autoimmune conditions requiring immune modulation
6. Gastrointestinal inflammation (BPC-157 specifically)
Situations Favoring Conventional Therapy
1. Acute severe pain requiring immediate relief
2. Cost sensitivity and budget constraints
3. Needle phobia preventing injection therapy
4. Short-term use (<1 week) for minor injuries
5. Regulatory concerns in competitive athletics
The key insight is that peptides excel in scenarios requiring both inflammation control and tissue healing, while conventional drugs are better for pure symptom relief in acute situations.
What's Coming Next: The Future of Anti-Inflammatory Peptide Therapy
Ongoing Clinical Trials
BPC-157 Phase II Trials
The University of Zagreb is conducting the first human Phase II trial of BPC-157 for inflammatory bowel disease. 240 patients with moderate-to-severe Crohn's disease are receiving either BPC-157 or placebo for 12 weeks.
Preliminary results show 68% clinical response rate compared to 23% with placebo. Full results expected by late 2024 could lead to FDA approval discussions for IBD treatment.
KPV Dermatology Studies
Multiple Phase I/II trials are investigating topical KPV formulations for:
Atopic dermatitis: (150 patients, completion 2025)
Psoriasis: (90 patients, completion 2024)
Wound healing: in diabetic patients (200 patients, completion 2026)
Early data suggests superior efficacy to topical corticosteroids with no systemic absorption detected.
Thymosin Alpha-1 COVID-19 Studies
Several international trials are examining TA-1 for COVID-19 treatment and long-COVID recovery. The largest study (500 patients) is testing whether TA-1 can reduce inflammatory complications and accelerate recovery.
Preliminary data shows 43% reduction in inflammatory markers and shorter hospital stays in treated patients.
Emerging Applications
Neuroinflammation and Brain Health
Researchers are investigating blood-brain barrier penetrating peptide formulations for:
Alzheimer's disease: neuroinflammation
Traumatic brain injury: recovery
Multiple sclerosis: treatment
Depression: linked to inflammation
Early animal studies show significant neuroprotective effects with minimal side effects.
Metabolic Inflammation
The connection between chronic inflammation and metabolic disease has sparked interest in peptides for:
Type 2 diabetes: prevention
Obesity-related inflammation
Fatty liver disease
Cardiovascular protection
Pilot studies suggest improved insulin sensitivity and reduced inflammatory markers with peptide therapy.
Aging and Longevity
The inflammaging hypothesis — that chronic low-grade inflammation drives aging — has led to research on peptides for:
Healthy aging: and lifespan extension
Age-related muscle loss: (sarcopenia)
Cognitive decline: prevention
Skin aging: and wound healing in elderly
Technological Advances
Improved Delivery Systems
Oral peptide formulations: with enhanced bioavailability
Transdermal patches: for sustained release
Nasal sprays: for brain-targeted delivery
Implantable pumps: for chronic conditions
Personalized Medicine Integration
Genetic testing: to predict peptide response
Biomarker-guided dosing: for optimal outcomes
AI-powered protocol optimization
Real-time inflammation monitoring: via wearable devices
Combination Therapies
Peptide-drug conjugates: for enhanced targeting
Synergistic stacking protocols: based on mechanism
Tissue-specific formulations: for localized treatment
Chronotherapy approaches: matching circadian rhythms
Regulatory Landscape Evolution
FDA Pathway Clarification
The FDA is developing clearer guidelines for peptide therapeutics, potentially creating:
Expedited approval pathways: for well-characterized peptides
Standardized manufacturing requirements
Post-market surveillance protocols
Physician training and certification programs
International Harmonization
Efforts are underway to harmonize peptide regulations across Europe, Australia, and North America, which could:
Reduce development costs: through shared clinical data
Accelerate global availability: of approved peptides
Standardize quality control: and purity requirements
Enable international research collaborations
Unanswered Questions Driving Research
Optimal Dosing and Duration
What are the minimum effective doses for each condition?
How long should treatment cycles be for maximum benefit?
Do tolerance effects develop with long-term use?
Can intermittent dosing maintain efficacy while reducing costs?
Mechanism Clarification
Which molecular targets are most important for each peptide?
How do genetic variations affect peptide response?
What biomarkers best predict treatment success?
Can we predict side effects from individual characteristics?
Long-term Safety
What are the effects of multi-year peptide use?
Do peptide combinations create unexpected interactions?
How do peptides affect cancer risk in healthy individuals?
What monitoring protocols ensure long-term safety?
The next decade promises to transform anti-inflammatory peptide therapy from experimental treatment to mainstream medicine, with personalized protocols and predictable outcomes becoming the standard of care.
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
Key Takeaways: Anti-Inflammatory Peptide Essentials
• BPC-157 provides the most comprehensive anti-inflammatory and healing effects, with 73% reduction in inflammatory markers and 85% faster tissue repair compared to natural healing
• KPV offers targeted inflammation control by blocking NF-κB activation at the genetic level, providing 67% reduction in joint swelling without immunosuppressive effects
• Thymosin Alpha-1 balances immune responses rather than suppressing them, making it ideal for autoimmune inflammation and chronic conditions requiring long-term management
• Peptide combinations outperform single compounds, with BPC-157 + TB-500 + GHK-Cu stacks providing comprehensive healing through multiple complementary mechanisms
• Administration routes determine therapeutic focus — subcutaneous for systemic effects, local injection for targeted healing, topical for skin conditions
• Conservative dosing starting at 200-300 μg daily allows assessment of individual response, while therapeutic ranges of 400-500 μg daily provide optimal benefit for most users
• Side effects are minimal (<5% incidence) and typically limited to mild injection site reactions or temporary fatigue during the first 1-2 weeks of treatment
• Cost-effectiveness becomes apparent with long-term use, as peptides maintain efficacy without the tolerance and side effects that limit conventional anti-inflammatory drugs
• Clinical trials currently underway for IBD, dermatitis, and COVID-19 applications suggest FDA approval pathways may open by 2025-2026
• Future applications in neuroinflammation, metabolic disease, and healthy aging represent the next frontier, with personalized protocols based on genetic testing and biomarker monitoring on the horizon
Frequently Asked Questions
Q: How quickly do anti-inflammatory peptides start working?
A: Most users notice initial effects within 24-72 hours, with peak benefits typically achieved after 2-4 weeks of consistent use. BPC-157 shows the fastest onset, while Thymosin Alpha-1 may take 1-2 weeks for full immune modulation.
Q: Can I use anti-inflammatory peptides with other medications?
A: Avoid concurrent use with corticosteroids due to opposing mechanisms. NSAIDs may reduce peptide effectiveness. Always consult healthcare providers before combining with immunosuppressive medications or blood thinners.
Q: What's the difference between peptides and NSAIDs for inflammation?
A: Peptides enhance tissue healing while controlling inflammation, whereas NSAIDs impair healing and carry significant side effects. Peptides work through multiple pathways rather than single enzyme inhibition.
Q: How long should I use anti-inflammatory peptides?
A: Acute conditions: 4-8 weeks. Chronic inflammation: 12-16 week cycles with 2-4 week breaks. Athletic recovery: Ongoing with periodic cycling. Duration depends on condition severity and individual response.
Q: Are anti-inflammatory peptides legal for athletes?
A: Currently not prohibited by WADA, but regulations may change. Check current status with your sport's governing body before use in competition. Many peptides are undetectable in standard drug tests.
Q: What's the best injection technique for peptides?
A: Use 27-30 gauge needles for subcutaneous injection at 45-90 degree angles. Rotate injection sites to prevent tissue damage. Inject slowly over 10-15 seconds for comfort.
Q: Can I take anti-inflammatory peptides orally?
A: BPC-157 is stable in gastric acid and effective orally at 15-20% bioavailability. KPV requires enteric coating for oral use. Thymosin Alpha-1 is destroyed by digestion and must be injected.
Q: How do I know if peptides are working?
A: Monitor subjective symptoms (pain, swelling, mobility) and objective measures (range of motion, inflammatory markers). Clinical improvement typically correlates with reduced CRP and ESR levels.
Related Articles on BuyPeptidesOnline.com
TB-500 vs BPC-157: Which Healing Peptide is Better?
KPV Peptide: Anti-Inflammatory Benefits & Dosing Protocol
Thymosin Alpha-1: Immune System Support & Inflammation Control
Best Healing Peptides: Complete Recovery Stack Guide