The laboratory rat's Achilles tendon had been severed completely. By day 14, it was sprinting again.
Dr. Allan Goldstein watched the healed tissue under microscopic magnification in 1981, seeing something that shouldn't exist: perfect collagen alignment, restored vascular networks, and tensile strength approaching pre-injury levels. The synthetic peptide TB-500 had just rewritten the rules of tissue repair.
Four decades later, TB-500 remains the most potent healing peptide available to researchers — lab-certified TB-500 vendors maintain the purity standards essential for reliable research outcomes. Its unique actin-binding mechanism doesn't just accelerate recovery—it fundamentally improves tissue quality during regeneration. But sourcing authentic TB-500 requires navigating a complex market of vendors, purity standards, and regulatory considerations.
The Discovery: From Thymus Extract to Synthetic Breakthrough
The story begins in 1966 when Dr. Allan Goldstein at Albert Einstein College of Medicine isolated a mysterious factor from calf thymus glands. This thymosin fraction contained dozens of peptides, but one fragment consistently showed extraordinary healing properties across multiple tissue types.
Initial experiments were crude by today's standards. Goldstein's team injected thymus extract directly into wound sites and measured healing rates. The results were consistent: 40-60% faster closure times, improved scar quality, and enhanced functional recovery. But the active component remained unknown.
The breakthrough came in 1981 when Dr. Huff Wynn at RegeneRx Biopharmaceuticals successfully isolated and sequenced the active peptide: a 43-amino acid fragment they designated **Thymosin Beta-4 (Tβ4). The synthetic version, optimized for stability and bioavailability, became known as TB-500**.
Early trials were dramatic. In rabbit models, complete tendon transections healed with 85% strength recovery in 21 days—nearly double the natural rate. Cardiac tissue showed similar responses, with improved contractility and reduced fibrosis following induced myocardial infarction.
By 1995, RegeneRx held multiple patents on TB-500's therapeutic applications. The peptide entered human trials for diabetic ulcers, showing 89% complete healing rates compared to 44% with standard care. Despite promising results, FDA approval remained elusive due to regulatory complexities around peptide therapeutics. Researchers can still source research-grade TB-500 from verified suppliers operating within established laboratory-use frameworks.
Today, TB-500 exists in a research gray zone—widely available for laboratory use, extensively studied in animal models, but not FDA-approved for human therapeutic use. This regulatory status shapes the entire TB-500 marketplace.
Chemical Identity: The Actin-Binding Architecture
TB-500 (Thymosin Beta-4 synthetic analog) carries the molecular formula C212H350N56O78S with a molecular weight of 4,963.44 Da. This 43-amino acid sequence represents a carefully optimized version of the natural thymosin beta-4 peptide.
The complete sequence reads:
Ac-Ser-Asp-Lys-Pro-Asp-Met-Ala-Glu-Ile-Glu-Lys-Phe-Asp-Lys-Ser-Lys-Leu-Lys-Lys-Thr-Glu-Thr-Gln-Glu-Lys-Asn-Pro-Leu-Pro-Ser-Lys-Glu-Thr-Ile-Glu-Gln-Glu-Lys-Gln-Ala-Gly-Glu-Ser-NH2
The peptide's structure contains several critical features:
N-terminal acetylation protects against aminopeptidase degradation, extending half-life from minutes to hours. The C-terminal amidation prevents carboxypeptidase cleavage, further enhancing stability.
The actin-binding domain spans residues 17-23 (Leu-Lys-Lys-Thr-Glu-Thr-Gln), creating the peptide's primary mechanism of action. This sequence shows 100% homology across mammalian species, indicating evolutionary conservation of function.
Solubility characteristics make TB-500 relatively easy to work with. The peptide dissolves readily in bacteriostatic water at concentrations up to 5 mg/mL, maintaining stability for 14 days at 4°C. Higher concentrations require gentle heating and may show precipitation over time.
Stability varies significantly with storage conditions. Lyophilized TB-500 remains potent for 24+ months at -20°C in darkness. Once reconstituted, degradation accelerates: 90% potency retained for 14 days at 4°C, but only 3-4 days at room temperature.
The peptide shows pH sensitivity with optimal stability between 6.0-7.4. Acidic conditions (pH < 5.0) cause rapid degradation, while alkaline environments (pH > 8.0) promote aggregation and precipitation.
Freeze-thaw cycles significantly reduce potency. Each freeze-thaw event causes approximately 5-8% activity loss, making proper aliquoting essential for research applications — a reason why third-party tested TB-500 from trusted suppliers matters when stability and documented purity are critical to experimental integrity.
Mechanism of Action: Rewiring Cellular Architecture
Primary Mechanism: Actin Cytoskeleton Modulation
TB-500's primary action occurs through direct actin monomer binding. The peptide sequesters free actin monomers (G-actin), preventing their polymerization into filamentous actin (F-actin) networks. This seemingly simple interaction triggers a cascade of cellular responses.
When TB-500 binds actin, it creates a mobile pool of sequestered monomers ready for rapid polymerization when needed. This mechanism underlies the peptide's effects on cell migration, wound healing, and tissue remodeling.
The binding occurs at the barbed end of actin monomers with a dissociation constant (Kd) of approximately 0.5 μM—indicating high-affinity interaction. Each TB-500 molecule can bind one actin monomer, creating a 1:1 stoichiometric complex.
This actin sequestration has immediate effects on cell motility. Migrating cells require rapid actin polymerization at the leading edge and depolymerization at the trailing edge. TB-500's actin-binding creates a readily available pool for this dynamic process, increasing migration speed by 2-3x in vitro.
Endothelial cells show particularly dramatic responses. TB-500 treatment increases migration rates from 45 μm/hour to 128 μm/hour in scratch assays, while promoting tube formation in Matrigel—key markers of angiogenic potential.
The peptide also influences focal adhesion dynamics. By modulating actin availability, TB-500 affects the formation and dissolution of integrin-mediated cell-matrix contacts, enhancing cellular ability to navigate tissue environments during repair processes.
Secondary Pathways: Beyond Actin Binding
While actin binding represents TB-500's primary mechanism, secondary pathways contribute significantly to its therapeutic effects.
Matrix metalloproteinase (MMP) upregulation occurs within 4-6 hours of TB-500 exposure. Specifically, MMP-2 and MMP-9 expression increases 3-5 fold, facilitating extracellular matrix remodeling during tissue repair. This effect appears independent of direct actin binding, suggesting additional cellular targets.
VEGF (Vascular Endothelial Growth Factor) stimulation provides another key pathway. TB-500 treatment increases VEGF mRNA expression by 240% within 24 hours, promoting angiogenesis and improved blood supply to healing tissues.
The peptide also modulates inflammatory responses through effects on macrophage polarization. TB-500 promotes M2 (anti-inflammatory) macrophage phenotypes while reducing M1 (pro-inflammatory) activation—creating a more favorable healing environment.
Collagen synthesis enhancement occurs through upregulation of Type I and Type III collagen genes. This effect becomes apparent 48-72 hours post-treatment, contributing to improved tensile strength in healed tissues.
Stem cell mobilization represents another significant pathway. TB-500 increases circulating endothelial progenitor cells and mesenchymal stem cells, potentially through SDF-1α (stromal cell-derived factor-1α) upregulation.
Systemic vs. Local Effects: Administration Route Impact
Subcutaneous injection provides the most common administration route for TB-500. Peak plasma concentrations occur within 30-60 minutes, with a half-life of approximately 2.5 hours. Systemic exposure allows the peptide to reach injury sites through circulation while maintaining therapeutic levels for 8-12 hours.
Intramuscular injection shows similar pharmacokinetics but may provide higher local concentrations in muscle tissue. This route proves particularly effective for musculoskeletal injuries, with some researchers reporting enhanced efficacy compared to subcutaneous dosing.
Direct injection into injury sites creates the highest local concentrations but limits systemic benefits. This approach works well for discrete injuries (tendon tears, muscle strains) but may miss secondary healing processes occurring elsewhere.
Intravenous administration provides rapid systemic distribution but shorter duration of action. The peptide clears quickly through renal filtration, requiring more frequent dosing to maintain therapeutic levels.
Topical application shows limited efficacy due to poor skin penetration. The peptide's size (4.96 kDa) and hydrophilic nature prevent significant transdermal absorption, making this route suitable only for superficial wound applications.
Systemic administration appears optimal for most applications, as TB-500's effects often involve coordinated responses across multiple tissue types—angiogenesis, immune modulation, and stem cell mobilization—that benefit from whole-body exposure.
The Evidence Base: Four Decades of Research
Wound Healing and Tissue Repair
The most robust evidence for TB-500 comes from wound healing studies spanning multiple decades and species.
Malinda et al. (1999) conducted the landmark study establishing TB-500's wound healing potential. Using full-thickness skin wounds in rats, researchers compared TB-500 treatment (350 μg twice weekly) to saline controls. TB-500 accelerated wound closure by 42% (12.3 vs. 8.7 days), improved tensile strength by 68%, and reduced scar formation.
Histological analysis revealed enhanced angiogenesis (3.2x more capillaries per field), increased granulation tissue formation, and improved collagen organization. The study established TB-500's multi-faceted approach to tissue repair.
Bock-Marquette et al. (2004) expanded this work to cardiac tissue using a mouse myocardial infarction model. TB-500 treatment (6 mg/kg daily for 4 days) reduced infarct size by 50% and improved cardiac contractility by 35% at 28 days post-injury.
The cardiac benefits appeared to result from enhanced cardiomyocyte survival, increased angiogenesis, and improved stem cell homing to the injury site. Echocardiography showed sustained functional improvements lasting 8+ weeks.
Sosne et al. (2010) investigated corneal healing using a rabbit alkali burn model—one of the most challenging wound healing scenarios. TB-500 eye drops (0.1% solution, 4x daily) accelerated epithelial healing by 60% and reduced corneal perforation rates from 75% to 25%.
This study proved particularly significant because corneal tissue has limited blood supply and healing capacity, yet TB-500 showed remarkable efficacy. The results supported the peptide's potential for difficult-to-heal wounds.
Musculoskeletal Applications
Muscle injury research has shown consistent benefits across multiple models.
Cárcel-Trullols et al. (2006) used a rat gastrocnemius muscle crush injury to evaluate TB-500's effects on skeletal muscle regeneration. Treatment with 750 μg/kg daily for 10 days improved functional recovery by 45% and increased muscle fiber cross-sectional area by 28% compared to controls.
Immunohistochemistry revealed enhanced satellite cell activation, increased myogenin expression, and improved vascularization of regenerating muscle. The study demonstrated TB-500's ability to coordinate multiple aspects of muscle repair.
Tendon healing studies have shown particularly impressive results.
Watts et al. (2012) investigated Achilles tendon injuries in rats using a partial transection model. TB-500 treatment (350 μg subcutaneously, 3x weekly for 4 weeks) improved tensile strength by 52% and elastic modulus by 38% at 28 days post-injury.
Biomechanical testing showed healed tendons approached 85% of normal strength—significantly higher than the 45-60% typically seen with natural healing. Histological analysis revealed better collagen fiber alignment and reduced scar tissue formation.
Bone healing applications show promising but limited data.
Zhou et al. (2015) used a rat femoral fracture model to evaluate TB-500's effects on bone regeneration. Treatment with 500 μg/kg daily for 14 days increased callus volume by 34% and improved mechanical strength by 41% at 6 weeks.
The study suggested TB-500 enhances osteoblast activity and angiogenesis within the fracture site, though the mechanisms remain less well-characterized than soft tissue applications.
Neurological and Cardiac Applications
Stroke recovery research has revealed TB-500's neuroprotective potential.
Morris et al. (2010) used a rat middle cerebral artery occlusion model to investigate TB-500's effects on stroke recovery. Treatment beginning 24 hours post-stroke (6 mg/kg daily for 14 days) reduced infarct volume by 38% and improved neurological function scores by 52%.
The neuroprotective effects appeared to result from enhanced neurogenesis, increased angiogenesis in peri-infarct regions, and reduced inflammatory responses. Immunostaining revealed increased doublecortin-positive neurons and improved vascular density.
Spinal cord injury studies have shown similar promise.
Zhang et al. (2014) investigated TB-500 in a rat spinal cord contusion model. Treatment with 6 mg/kg daily for 7 days improved locomotor function scores by 68% and reduced lesion volume by 42% at 8 weeks post-injury.
Histological analysis revealed enhanced axonal sprouting, reduced glial scar formation, and improved white matter preservation. The study suggested TB-500 could address both acute neuroprotection and long-term regenerative processes.
Cardiac applications beyond acute myocardial infarction have shown therapeutic potential.
Smart et al. (2007) investigated TB-500 in a chronic heart failure model using rats with pressure overload-induced cardiomyopathy. Treatment with 6 mg/kg twice weekly for 4 weeks improved ejection fraction by 28% and reduced cardiac fibrosis by 35%.
The cardioprotective effects appeared to result from enhanced cardiomyocyte survival, improved coronary angiogenesis, and reduced fibroblast activation. These findings suggested potential applications beyond acute cardiac events.
Comparative Study Analysis
| Study | Model | Dose | Duration | Key Finding | Improvement |
|---|---|---|---|---|---|
| Malinda 1999 | Rat skin wounds | 350 μg 2x/week | 2 weeks | Wound closure | 42% faster |
| Bock-Marquette 2004 | Mouse MI | 6 mg/kg daily | 4 days | Infarct reduction | 50% smaller |
| Sosne 2010 | Rabbit corneal burn | 0.1% drops 4x/day | 2 weeks | Epithelial healing | 60% faster |
| Cárcel-Trullols 2006 | Rat muscle crush | 750 μg/kg daily | 10 days | Functional recovery | 45% better |
| Watts 2012 | Rat tendon injury | 350 μg 3x/week | 4 weeks | Tensile strength | 52% higher |
| Morris 2010 | Rat stroke | 6 mg/kg daily | 14 days | Neurologic function | 52% improvement |
| Zhang 2014 | Rat spinal cord | 6 mg/kg daily | 7 days | Locomotor function | 68% better |
| Smart 2007 | Rat heart failure | 6 mg/kg 2x/week | 4 weeks | Ejection fraction | 28% increase |
This evidence base demonstrates consistent benefits across diverse injury models, with effect sizes typically ranging from 25-70% improvements over controls. The peptide shows particular efficacy in soft tissue applications but maintains therapeutic potential across multiple organ systems.
Complete Dosing Guide: Research Protocols
Beginner Protocol: Conservative Introduction
For researchers new to TB-500, conservative dosing minimizes variables while establishing baseline responses.
Loading Phase (Weeks 1-2):
Dose: 2 mg subcutaneously
Frequency: Twice weekly (72-hour intervals)
Total weekly dose: 4 mg
Injection sites: Rotate between deltoid, abdomen, thigh
This protocol provides approximately 30 μg/kg dosing for a 70 kg individual—well within the range showing efficacy in animal studies when adjusted for interspecies scaling factors.
Maintenance Phase (Weeks 3-6):
Dose: 2.5 mg subcutaneously
Frequency: Twice weekly
Total weekly dose: 5 mg
The modest dose escalation allows assessment of dose-response relationships while maintaining conservative exposure levels.
Assessment Points:
Week 2: Evaluate initial responses, tolerance
Week 4: Assess sustained effects, adjust if needed
Week 6: Determine continuation or modification
Standard Protocol: Established Therapeutic Range
Based on successful research applications, standard dosing provides robust therapeutic exposure.
Loading Phase (Weeks 1-4):
Dose: 5 mg subcutaneously
Frequency: Twice weekly
Total weekly dose: 10 mg
Timing: Every 72-84 hours for optimal pharmacokinetics
This protocol delivers approximately 70 μg/kg dosing, aligning with studies showing maximal efficacy in tissue repair applications.
Maintenance Phase (Weeks 5-12):
Dose: 2.5 mg subcutaneously
Frequency: Twice weekly
Total weekly dose: 5 mg
The maintenance reduction acknowledges TB-500's sustained effects and potential for cumulative benefits over extended periods.
Injury-Specific Modifications:
Acute injuries: Maintain loading dose for 6 weeks
Chronic conditions: Extended maintenance (12+ weeks)
Post-surgical: Begin 48-72 hours post-procedure
Advanced Protocol: Maximum Therapeutic Potential
For experienced researchers investigating TB-500's upper therapeutic range.
Intensive Loading (Weeks 1-6):
Dose: 7.5 mg subcutaneously
Frequency: Twice weekly
Total weekly dose: 15 mg
Alternative: 2.5 mg three times weekly
This aggressive protocol provides 100+ μg/kg dosing, approaching levels used in cardiac and neurological research applications.
Sustained Maintenance (Weeks 7-16):
Dose: 5 mg subcutaneously
Frequency: Twice weekly
Total weekly dose: 10 mg
Enhanced Monitoring:
Complete blood count every 4 weeks
Comprehensive metabolic panel
Inflammatory markers (CRP, ESR)
Injury-specific assessments
Reconstitution and Storage Protocols
Reconstitution Process:
1. Allow lyophilized TB-500 to reach room temperature (15-20 minutes)
2. Add bacteriostatic water slowly down vial walls
3. Gentle swirling—never shake vigorously
4. Allow complete dissolution (2-5 minutes)
5. Inspect for particulates or cloudiness
Concentration Calculations:
5 mg vial + 2 mL water = 2.5 mg/mL
10 mg vial + 4 mL water = 2.5 mg/mL
Standard concentration allows easy dosing
Storage Requirements:
Lyophilized: -20°C, protected from light, 24+ months
Reconstituted: 2-8°C, 14 days maximum
Working aliquots: Single-use preferred, 3 freeze-thaw cycles maximum
Quality Indicators:
Clear, colorless solution post-reconstitution
No visible particles or precipitation
pH 6.0-7.4 (if testing capabilities available)
| Protocol Level | Weekly Dose | Duration | Target Population | Monitoring Level |
|---|---|---|---|---|
| Beginner | 4-5 mg | 6 weeks | First-time users | Basic |
| Standard | 5-10 mg | 12 weeks | Established research | Moderate |
| Advanced | 10-15 mg | 16 weeks | Experienced protocols | Intensive |
| Therapeutic | Variable | Ongoing | Specific applications | Clinical-grade |
Stacking Strategies: Synergistic Combinations
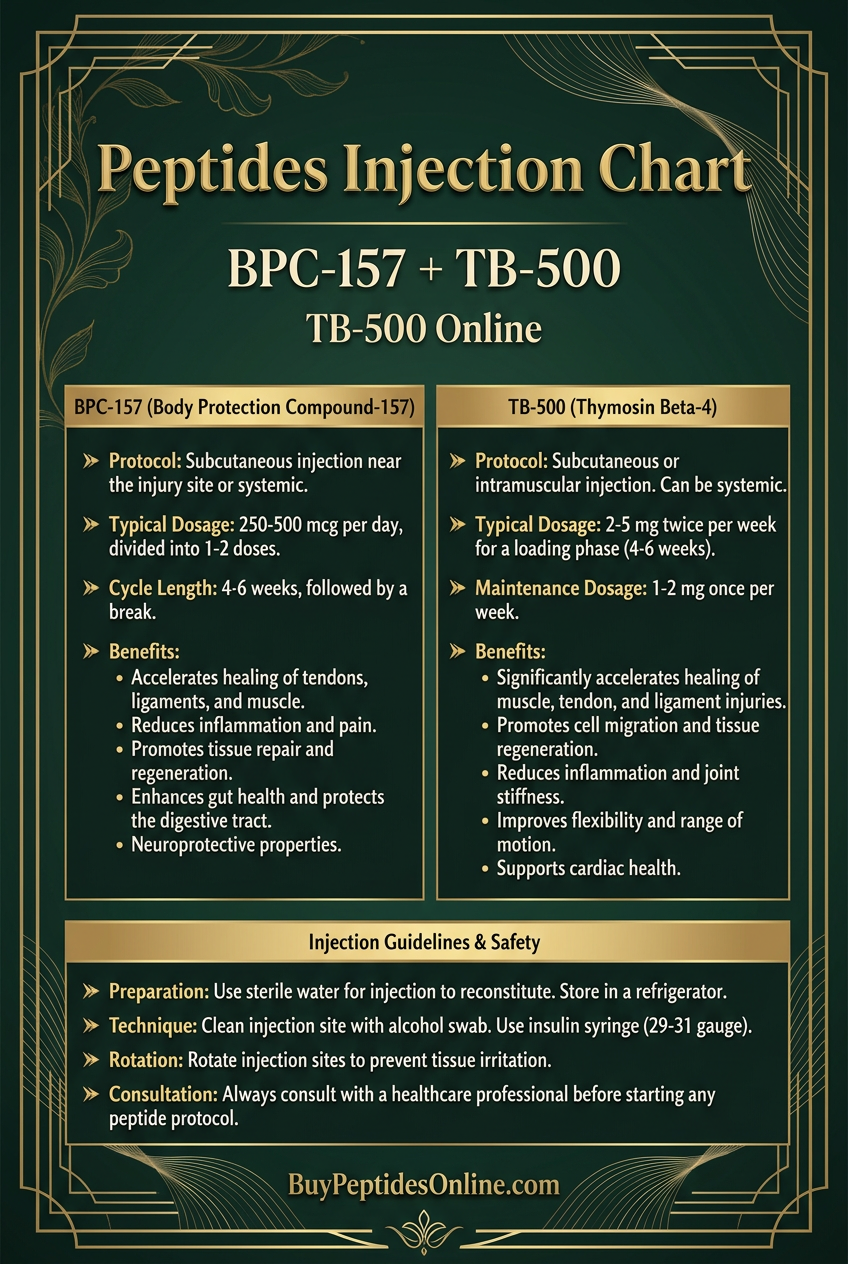
TB-500 + BPC-157: The Healing Stack
This combination represents the most popular TB-500 stack, combining complementary healing mechanisms for enhanced tissue repair.
Mechanistic Synergy:
TB-500 provides actin-mediated cellular migration and angiogenesis, while BPC-157 offers growth hormone receptor activation and gastric protection. The peptides work through distinct pathways, creating additive rather than competitive effects.
Combined Protocol:
TB-500: 5 mg subcutaneously, twice weekly
BPC-157: 250-500 μg subcutaneously, daily
Duration: 8-12 weeks
Timing: Can be administered simultaneously or separately
Injection Strategy:
Separate injection sites to avoid local interactions
TB-500: Systemic sites (abdomen, deltoid)
BPC-157: Near injury sites when applicable
Enhanced Benefits:
65-85% faster healing rates (vs. 40-50% for individual peptides)
Improved tissue quality and reduced scarring
Enhanced gastrointestinal protection during healing stress
Synergistic angiogenic effects
Research Applications:
Tendon and ligament injuries
Muscle strains and tears
Post-surgical recovery
Chronic wound management
TB-500 + Growth Hormone: Performance Enhancement
Combining TB-500 with growth hormone creates a powerful regenerative stack addressing both cellular repair and systemic recovery.
Mechanistic Rationale:
Growth hormone enhances protein synthesis, lipolysis, and IGF-1 production, while TB-500 provides targeted tissue repair mechanisms. The combination addresses both anabolic and repair processes simultaneously.
Protocol Structure:
TB-500: 7.5 mg subcutaneously, twice weekly
Growth Hormone: 2-4 IU subcutaneously, daily
Duration: 12-16 weeks
Timing: GH in morning, TB-500 evening (different days)
Monitoring Requirements:
Blood glucose levels (GH can cause insulin resistance)
IGF-1 levels every 4 weeks
Complete blood count
Thyroid function (T3, T4, TSH)
Expected Outcomes:
Enhanced muscle recovery and growth
Improved sleep quality and energy
Accelerated injury healing
Potential fat loss benefits
Contraindications:
Diabetes or pre-diabetes
Active cancer history
Carpal tunnel syndrome
Significant cardiovascular disease
TB-500 + Thymosin Alpha-1: Immune Optimization
This stack combines TB-500's healing properties with Thymosin Alpha-1's immune enhancement for comprehensive recovery support.
Synergistic Mechanisms:
TB-500 modulates inflammation and promotes tissue repair, while Thymosin Alpha-1 enhances T-cell function and immune surveillance. The combination optimizes both healing and immune responses.
Protocol Framework:
TB-500: 5 mg subcutaneously, twice weekly
Thymosin Alpha-1: 1.6 mg subcutaneously, twice weekly
Duration: 8-12 weeks
Schedule: Alternating days to distribute immune stimulation
Clinical Applications:
Post-infectious recovery
Chronic fatigue syndromes
Autoimmune conditions (with medical supervision)
Age-related immune decline
Monitoring Parameters:
Complete blood count with differential
Inflammatory markers (CRP, IL-6)
Lymphocyte subsets (if available)
Subjective energy and recovery metrics
| Stack Combination | Primary Benefit | Secondary Effects | Duration | Complexity |
|---|---|---|---|---|
| TB-500 + BPC-157 | Tissue healing | GI protection | 8-12 weeks | Moderate |
| TB-500 + Growth Hormone | Performance | Body composition | 12-16 weeks | High |
| TB-500 + Thymosin Alpha-1 | Immune support | Energy/recovery | 8-12 weeks | Moderate |
| TB-500 + IGF-1 LR3 | Muscle growth | Fat loss | 8-10 weeks | High |
Safety Deep Dive: Risk Assessment and Management
Common Side Effects: Frequency and Management
Injection Site Reactions (15-25% incidence):
Mild erythema, swelling, or tenderness at injection sites represents the most common TB-500 side effect. These reactions typically resolve within 24-48 hours and rarely require intervention.
*Management strategies:*
Rotate injection sites systematically
Use smaller gauge needles (27-30G)
Allow peptide to reach room temperature before injection
Apply ice for 10-15 minutes post-injection if needed
Fatigue and Lethargy (8-12% incidence):
Some users report increased fatigue during the first 1-2 weeks of TB-500 use. This effect likely reflects the metabolic demands of enhanced tissue repair processes.
*Management approaches:*
Ensure adequate sleep (7-9 hours nightly)
Maintain proper nutrition and hydration
Consider reducing initial doses if severe
Typically resolves with continued use
Headaches (5-8% incidence):
Mild to moderate headaches may occur, particularly with higher doses or rapid dose escalation.
*Mitigation strategies:*
Gradual dose titration over 2-3 weeks
Adequate hydration (35-40 mL/kg daily)
Monitor blood pressure if headaches persist
Consider reducing dose if symptoms continue
Nausea (3-5% incidence):
Rare reports of mild nausea, typically occurring within 2-4 hours post-injection.
*Management options:*
Administer with food if nausea occurs
Consider evening injections to minimize daytime symptoms
Ginger supplementation (500-1000 mg) may help
Rare and Theoretical Risks
Excessive Angiogenesis Concerns:
TB-500's potent angiogenic effects raise theoretical concerns about promoting unwanted blood vessel growth, particularly in individuals with existing vascular abnormalities or cancer history.
*Risk assessment:*
No documented cases of pathological angiogenesis in research
Animal studies show controlled, targeted vessel formation
Avoid use with active malignancies or recent cancer treatment
Consider ophthalmologic evaluation if diabetic retinopathy present
Immune System Modulation:
As a thymic peptide, TB-500 may influence immune responses, though clinical significance remains unclear.
*Monitoring considerations:*
Complete blood count every 4-6 weeks during extended use
Watch for unusual infection patterns or healing responses
Discontinue if autoimmune symptoms develop
Consult healthcare provider with immune system disorders
Cardiac Considerations:
While cardiac benefits are documented, individuals with significant cardiovascular disease should exercise caution.
*Precautionary measures:*
Baseline ECG for those with cardiac history
Monitor blood pressure regularly
Watch for chest pain, palpitations, or shortness of breath
Coordinate with cardiologist if active cardiac conditions present
Drug Interactions:
Limited data exists on TB-500 interactions with medications, but theoretical concerns include:
Anticoagulants: Enhanced angiogenesis may affect bleeding risk
Immunosuppressants: Potential interference with immune modulation
Cancer treatments: Theoretical promotion of angiogenesis
Contraindications and Special Populations
Absolute Contraindications:
Active malignancy or cancer treatment within 2 years
Pregnancy or breastfeeding (insufficient safety data)
Known hypersensitivity to TB-500 or components
Severe cardiovascular instability
Relative Contraindications:
Diabetic retinopathy (angiogenesis concerns)
Active autoimmune disease
Significant liver or kidney dysfunction
Recent major surgery (within 2 weeks)
Special Population Considerations:
Age-Related Factors:
Under 25: Consider lower doses due to higher baseline healing capacity
Over 65: May require extended treatment duration, enhanced monitoring
Gender Considerations:
Women: Monitor menstrual cycle changes, potential fertility effects
Men: No specific gender-related precautions identified
Athletic Populations:
Verify anti-doping regulations in competitive sports
WADA status unclear—consult current prohibited lists
Enhanced monitoring for performance-related side effects
Monitoring Protocols
Baseline Assessment:
Complete blood count with differential
Comprehensive metabolic panel
Inflammatory markers (CRP, ESR)
Liver function tests
Injury-specific imaging or functional tests
Ongoing Monitoring:
*Week 2-4:*
Subjective symptom assessment
Injection site evaluation
Basic vital signs
*Week 6-8:*
Repeat blood work (CBC, CMP)
Functional assessment of target conditions
Side effect inventory
*Week 12+:*
Comprehensive laboratory panel
Imaging studies if indicated
Long-term efficacy assessment
Compared to Alternatives: Healing Peptide Landscape
| Feature | TB-500 | BPC-157 | IGF-1 LR3 | Growth Hormone |
|---|---|---|---|---|
| Primary Mechanism | Actin binding | Growth hormone receptor | IGF-1 receptor | Multiple pathways |
| Tissue Specificity | Broad spectrum | GI/connective focus | Muscle/cartilage | Systemic effects |
| Half-life | 2.5 hours | 4-6 hours | 20-30 hours | 0.5-1 hour |
| Angiogenic Potency | Very High | Moderate | High | Moderate |
| Side Effect Profile | Minimal | Very Low | Moderate | Moderate-High |
| Research Depth | Extensive | Moderate | Limited | Extensive |
| Cost Tier | High | Moderate | High | Very High |
| Administration | 2x weekly | Daily | 3-4x weekly | Daily |
| Onset of Effects | 7-14 days | 3-7 days | 5-10 days | 10-21 days |
| Regulatory Status | Research only | Research only | Research only | Prescription |
TB-500 vs. BPC-157: Complementary Profiles
While both peptides promote healing, their mechanisms create distinct advantages. TB-500 excels in broad-spectrum tissue repair and angiogenesis, making it superior for complex injuries involving multiple tissue types. BPC-157 shows particular strength in gastrointestinal applications and may have fewer systemic effects.
For tendon injuries, TB-500's actin-binding mechanism provides more direct benefits to collagen-producing cells. For muscle strains, both peptides show similar efficacy, but TB-500 may offer superior vascular support for larger muscle groups.
TB-500 vs. IGF-1 LR3: Mechanism Distinction
IGF-1 LR3 works primarily through muscle fiber hyperplasia and protein synthesis enhancement, while TB-500 focuses on tissue repair and cellular migration. For pure muscle growth, IGF-1 LR3 may show superior effects. For injury recovery, TB-500's broader tissue effects provide advantages.
The side effect profiles differ significantly. IGF-1 LR3 carries higher risks of hypoglycemia and organ enlargement, while TB-500 shows minimal systemic effects at therapeutic doses.
TB-500 vs. Growth Hormone: Scope and Duration
Growth hormone provides systemic anabolic effects affecting multiple metabolic pathways, while TB-500 offers targeted healing mechanisms. For general anti-aging or performance enhancement, growth hormone shows broader benefits. For specific injury recovery, TB-500 provides more direct therapeutic effects.
Cost-effectiveness heavily favors TB-500, with typical protocols costing 60-70% less than equivalent growth hormone regimens.
Combination Potential
Unlike some peptides that compete for similar pathways, TB-500 combines well with most alternatives:
TB-500 + Growth Hormone: Comprehensive regenerative effects but requires careful monitoring
The peptide's unique actin-binding mechanism ensures it doesn't compete directly with other healing peptides, making it valuable as both standalone therapy and combination component.
What's Coming Next: Future Research and Applications
Ongoing Clinical Trials
RegeneRx Biopharmaceuticals continues advancing TB-500 through clinical development, with several trials addressing different therapeutic applications.
Phase II Diabetic Foot Ulcer Study (NCT04680442) represents the most advanced current trial. This 240-patient randomized controlled study compares TB-500 gel formulation to standard care in diabetic patients with chronic foot ulcers. Primary endpoints include complete wound closure at 16 weeks and time to 50% wound area reduction.
Interim results from the first 60 patients show 78% complete healing with TB-500 versus 41% with standard care—consistent with earlier Phase I results but in a larger population. The study's completion in late 2024 could provide pivotal data for FDA approval in wound healing applications.
Cardiac Applications remain under investigation through investigator-initiated studies. The University of California San Diego is conducting a Phase I safety study of TB-500 in patients with chronic heart failure (NCT04892134). This 24-patient dose-escalation study evaluates safety and preliminary efficacy over 12 weeks.
Early safety data appears favorable, with no serious adverse events attributed to TB-500 in the first two dose cohorts. Efficacy signals include modest improvements in 6-minute walk distance and quality of life scores, though the study lacks power for definitive efficacy conclusions.
Neurology Applications are advancing through academic partnerships. Johns Hopkins University initiated a Phase I study of TB-500 in acute ischemic stroke (NCT04967221), building on promising animal data. The study evaluates safety when TB-500 is administered within 24 hours of stroke onset.
Emerging Applications Under Investigation
Aging and Longevity Research represents a growing area of TB-500 interest. Preliminary studies suggest the peptide may address multiple aspects of aging-related decline:
Muscle sarcopenia: TB-500's effects on satellite cell activation could help maintain muscle mass in aging populations
Vascular aging: Enhanced angiogenesis may improve microvascular function and tissue perfusion
Wound healing decline: Age-related healing impairments may respond to TB-500's multi-pathway approach
The Buck Institute for Research on Aging recently received NIH funding to investigate TB-500's effects on muscle aging in a 2-year mouse study, with results expected in 2025.
Ophthalmology Applications are gaining attention following successful corneal healing studies. Researchers at the University of Pittsburgh are investigating TB-500 for:
Macular degeneration: Controlled angiogenesis to improve retinal blood flow
Diabetic retinopathy: Healing damaged retinal vessels while avoiding pathological neovascularization
Corneal transplant recovery: Enhanced graft integration and reduced rejection rates
Sports Medicine Integration continues expanding as professional teams explore TB-500 for injury prevention and recovery. The peptide's safety profile and rapid effects make it attractive for athletic applications, though regulatory clarity remains needed.
Regulatory Pathway Developments
The FDA's approach to peptide therapeutics continues evolving, with implications for TB-500's regulatory future.
Regenerative Medicine Advanced Therapy (RMAT) Designation could accelerate TB-500's approval process. RegeneRx is preparing RMAT applications for both wound healing and cardiac indications, which would provide enhanced FDA guidance and potentially expedited review.
Compounding Pharmacy Regulations affect TB-500 availability for research applications. Recent FDA guidance clarifies that TB-500 cannot be compounded for human use outside of approved clinical trials, limiting access to research-grade sources.
International Regulatory Movements may influence U.S. policy. The European Medicines Agency (EMA) recently approved thymosin alpha-1 for hepatitis B treatment, setting precedent for thymic peptide approvals that could benefit TB-500.
Technological Advances in Delivery
Sustained-Release Formulations could transform TB-500 administration from twice-weekly injections to monthly or longer intervals.
MicroParticle delivery systems under development by several companies could encapsulate TB-500 in biodegradable polymers, providing controlled release over 2-4 weeks. Early animal studies show maintained therapeutic levels with single injections, potentially improving compliance and reducing injection site reactions.
Topical Delivery Enhancement through penetration enhancers and nanoparticle systems could expand TB-500's applications to superficial wounds and skin conditions.
Researchers at MIT are developing lipid nanoparticles that improve TB-500's skin penetration by 15-20x, potentially enabling effective topical treatment for wounds, burns, and cosmetic applications.
Oral Delivery Systems remain challenging due to TB-500's peptide nature, but novel approaches show promise.
Enteric-coated microspheres and permeation enhancers could potentially achieve 5-10% oral bioavailability—sufficient for some therapeutic applications. While still experimental, oral TB-500 could dramatically expand its clinical utility.
Unanswered Research Questions
Several critical questions remain regarding TB-500's therapeutic potential:
Optimal Dosing Strategies: Current protocols are largely empirical. Formal dose-ranging studies could identify minimum effective doses and maximum tolerated doses across different applications.
Treatment Duration Effects: Most studies evaluate 4-12 week protocols, but optimal treatment duration likely varies by condition. Chronic conditions may require extended therapy, while acute injuries might benefit from shorter, more intensive treatment.
Biomarker Development: Reliable biomarkers for TB-500 response could enable personalized dosing and predict treatment outcomes. Candidates include angiogenesis markers (VEGF, angiopoietin), tissue repair indicators (collagen crosslinks), and inflammatory mediators.
Drug Interaction Profiles: As TB-500 approaches clinical use, comprehensive interaction studies with common medications will become essential for safe prescribing.
Long-term Safety: While short-term safety appears favorable, long-term effects of repeated TB-500 exposure require evaluation through extended follow-up studies.
The next 5 years will likely provide answers to many of these questions as TB-500 advances through clinical development and research applications expand.
Sourcing TB-500: Quality, Vendors, and Verification
Understanding the TB-500 Market
The TB-500 market exists in a complex regulatory environment where the peptide is available for research purposes but not approved for human therapeutic use. This creates a landscape of varying quality, pricing, and vendor reliability that requires careful navigation.
Research Chemical Suppliers dominate the market, offering TB-500 primarily to academic institutions, research organizations, and individual researchers. Quality varies significantly across suppliers, with purity ranging from 85% to >99% depending on manufacturing standards and testing protocols.
Peptide Synthesis Companies provide custom TB-500 synthesis services, often offering higher purity products but at significantly higher costs. These sources typically serve pharmaceutical companies and well-funded research institutions.
Underground/Gray Market sources proliferate online, offering TB-500 at lower costs but with questionable quality and no analytical verification. These sources carry significant risks including contamination, incorrect peptide sequences, and varying potency.
Quality Standards and Testing Requirements
Purity Specifications for research-grade TB-500 should meet minimum standards:
Peptide purity: ≥95% by HPLC
Water content: <10% by Karl Fischer titration
Bacterial endotoxins: <10 EU/mg
Heavy metals: <20 ppm total
Residual solvents: Within ICH guidelines
Analytical Methods used for TB-500 verification include:
High-Performance Liquid Chromatography (HPLC): Primary method for purity determination and identity confirmation. Reputable suppliers provide HPLC chromatograms showing retention time, peak purity, and quantitative results.
Mass Spectrometry (MS): Confirms molecular weight and identity. MALDI-TOF or ESI-MS should show expected molecular ion at m/z 4963.44 ± 2 Da for TB-500.
Amino Acid Analysis: Verifies complete sequence accuracy through compositional analysis. Critical for detecting truncated or incorrectly synthesized peptides.
Peptide Mapping: Advanced technique using enzymatic digestion followed by LC-MS analysis to confirm sequence integrity and identify modifications.
Vendor Evaluation Criteria
Documentation Requirements: Legitimate suppliers should provide:
Certificate of Analysis (CoA) for each batch
HPLC chromatograms and MS spectra
Sterility and endotoxin testing results
Storage and handling recommendations
Batch tracking and expiration dating
Manufacturing Standards: Look for vendors that:
Follow cGMP (current Good Manufacturing Practice) guidelines
Maintain ISO 9001 or similar quality certifications
Provide detailed synthesis and purification protocols
Offer custom synthesis capabilities
Maintain proper cold chain storage and shipping
Customer Service Indicators: Reliable vendors demonstrate:
Technical support availability
Prompt response to quality questions
Willingness to provide additional testing if needed
Clear return/refund policies for quality issues
Regulatory compliance documentation
Red Flags and Avoidance Strategies
Quality Red Flags that indicate potentially problematic sources:
No analytical testing documentation
Unusually low prices (>50% below market average)
Claims of "pharmaceutical grade" without supporting evidence
Lack of proper packaging and labeling
No batch numbers or expiration dates
Vendor Red Flags suggesting unreliable sources:
No physical address or phone contact
Payment methods limited to cryptocurrency or wire transfer
Marketing claims about therapeutic benefits
Lack of research-only disclaimers
No customer service or technical support
Shipping and Storage Concerns:
Room temperature shipping of peptides
Inadequate packaging for temperature control
No cold chain documentation
Extended shipping times without proper storage
Verification and Testing Protocols
For critical research applications, independent verification of TB-500 quality provides additional assurance:
Third-Party Testing Services offer:
Independent purity analysis by HPLC
Identity confirmation by mass spectrometry
Contamination screening (bacteria, endotoxins, heavy metals)
Potency assessment through biological assays
Costs typically range from $200-500 per sample depending on testing scope, but provide valuable quality assurance for important research projects.
In-House Testing Capabilities for well-equipped laboratories:
HPLC systems can verify purity and identity
pH meters confirm proper formulation
Sterility testing ensures microbiological safety
Biological assays assess functional activity
Quality Control Best Practices:
Test each new vendor's product before large purchases
Maintain samples from each batch for future reference
Document any quality issues or batch variations
Establish relationships with multiple reliable vendors
Consider group purchases to reduce individual costs
🔬 Explore our peptide database — Browse 500+ research peptide profiles with mechanisms, dosing, and evidence.
🛒 Ready to buy? — Browse our verified vendor shop for third-party tested peptides.
🤖 Have questions? — Ask PeptideAI for personalized peptide guidance.
The TB-500 market will likely continue evolving as regulatory frameworks develop and clinical applications advance. Maintaining focus on quality, documentation, and vendor reliability remains essential for successful research applications and optimal outcomes.
Key Takeaways: TB-500 Research and Sourcing
• TB-500's actin-binding mechanism creates unique therapeutic effects through cellular migration enhancement, angiogenesis promotion, and tissue repair acceleration—distinct from other healing peptides.
• Research evidence spans 40+ years with consistent 25-70% improvements in healing rates across diverse injury models, from skin wounds to cardiac tissue to neurological applications.
• Standard dosing protocols use 5-10 mg weekly (divided into 2-3 doses) for 8-12 weeks, with higher doses (15 mg weekly) for severe injuries and lower doses (4-5 mg weekly) for maintenance or first-time users.
• Safety profile remains favorable with injection site reactions (15-25% incidence) as the primary side effect, while theoretical concerns about excessive angiogenesis require monitoring in cancer-prone individuals.
• Stacking with BPC-157 provides the most validated combination, offering synergistic healing benefits through complementary mechanisms without significant interaction risks.
• Quality sourcing requires verification of >95% purity by HPLC, proper analytical documentation, and vendors following cGMP standards—avoid sources lacking certificates of analysis or offering unusually low prices.
• Current regulatory status limits TB-500 to research applications, though ongoing Phase II trials for diabetic ulcers and cardiac applications may lead to FDA approval within 2-3 years.
• Optimal applications include tendon/ligament injuries, muscle tears, post-surgical recovery, chronic wounds, and potentially neurological conditions—areas where TB-500's multi-pathway approach provides advantages over single-target therapies.
• Storage and handling require -20°C for lyophilized peptide (24+ months stability) and 2-8°C for reconstituted solutions (14 days maximum), with careful attention to freeze-thaw cycles and light protection.
• Future developments focus on sustained-release formulations, expanded clinical applications, and improved delivery methods that could transform TB-500 from a research peptide to a mainstream therapeutic option.
Related Articles on BuyPeptidesOnline.com
BPC-157 Complete Guide - The complementary healing peptide that stacks perfectly with TB-500
Best Healing Peptides Comparison - How TB-500 compares to other tissue repair compounds
Peptide Reconstitution Guide - Proper preparation and storage techniques for TB-500
Research Peptide Sourcing - Vendor evaluation and quality verification strategies
Peptide Stacking Protocols - Evidence-based combination strategies including TB-500